

Abstract
Introduction:
Aflatoxins are secondary toxic metabolites produced by certain group of Aspergillus species in suitable conditions. These toxins are highly toxic, immunosuppressive, mutagenic, teratogenic and carcinogenic metabolites. The purpose of this study was to detection aflatoxin M1 concentration in mother's milk from rural area of Khorrambid town of Fars Province.
Materials and Methods:
In this study, 87 milk samples of mothers were collected by cluster sampling methods in the period between June and July 2011 and the amount of aflatoxin M1 was measured by a competitive ELISA method.
Results:
From 87 mother's milk, 24 (27.6%) samples were contaminated with aflatoxin M1 with mean concentration of 0.56 ± 1.23 pg/ml (range 0.13-4.91 pg/ml).
Conclusion:
The amount of aflatoxin M1 in mothers’ milk was lower than 50 ng/l (Europe Union and Iranian standard). Detection of Aflatoxin M1 in mothers’ milk is due to consuming contaminated food. This contamination not only threatens the health of the mothers but also has irreversible effects on the growth and health of their babies.
Keywords: Aflatoxin M1, enzyme-linked immunosorbent assay, milk, mothers, mycotoxins
INTRODUCTION
Breastfeeding is useful for the health of both mothers and infants. Infants, who are exclusively breastfed, are protected from many diseases.[1] Sometimes some unwanted or unfavorable contaminants such as mycotoxins, which are associated with maternal diet, are secreted in milk.[2] Although nutrition is something vital for human survival, however consumption of contaminated foodstuffs is one of the most important ways for toxic and carcinogenic materials entering the body. In early life, breast-feeding is usually the main method of feeding. Because children, particularly newborns, are more susceptible to various diseases, therefore breast milk should be free from harmful substances and toxins. Mycotoxins are secondary toxic metabolites of filamentous fungi, which are produced under favorable conditions on variety of food and feedstuffs.[3,4,5] Several studies have proved the presence of aflatoxins in human body fluids including milk.[6,7,8] Preparation, processing and consumption of foods in a safe manner are very important. Aflatoxins are highly toxic, immunosuppressive, mutagenic, teratogenic and carcinogenic metabolites. Different species of Aspergillus, such as A. flavus, A. parasiticus and A. nomius can grow on foodstuffs under appropriate conditions, and their toxins are usually found in human and animal body fluids including milk.[5,6,8,9,10] Aflatoxins are found in nuts, corn, cotton seed and crops before harvest.[11] Aflatoxin M1 (AFM1) is the main secondary metabolites found in milk secreted by animals and nursing mothers who have consumed food contaminated with aflatoxin B1 (AFB1).[12] International Agency of Research on Cancer (IARC) has classified aflatoxin M1 and B1 in terms of carcinogenesis in human beings in class 1.[10] Children are considered to be more susceptible to mycotoxins than adults because of their lower body weight, higher metabolic rate, lower ability to detoxify and incomplete development of some organs and tissues, notably the central nervous system.[13–14] In our country, few studies have been conducted about the concentration of aflatoxin M1 in human breast milk. In the villages of Khorrambid Town, the possibility of fungal infections is higher because most people are employed in farm and livestock business and store most of the food and feedstuffs in traditional methods. Furthermore, fungal toxins in mother's milk can threaten the health of mother and her infant and consequently society's health. Therefore, this study was designed in order to determine the concentration of aflatoxin M1 in mothers’ milk samples.
MATERIALS AND METHODS
Informed written consent was obtained from all the women before inclusion in this study. A total of 87 mother breast milk samples (5-10 ml) collected into sterile glass bottles by self-extraction from 7 rural health centers in Khorrambid-Iran, during June-July 2011. The criteria for inclusion was the health of nursing mothers who had healthy infants who were full term and breastfed, aged less than one year with normal birth weight, and with no chronic disease. All samples were kept at −20°C until the time of analysis. The samples were thawed gradually at 4°C and then vigorously mixed and were centrifuged for 15 min at 3500 g/10°C. Then, the upper creamy layer was completely removed by using a Pasteur pipette and the skimmed milk (lower phases) was used directly for testing AFM1.
The quantitative detection of AFM1 in the samples was performed according to the instructions of the competitive enzyme immunoassay using Euroclone kits (Italy). The test is based on the antigen-antibody reaction. The wells in the microtiter strips were coated with specific antibodies to AFM1. 200 μl of samples (standard solutions and milk samples) were added to the wells to occupy the binding sites proportionately then mixed gently and incubated for 30 min at room temperature in the dark. Then the liquid was poured out of the wells and the wells were filled with 300 μl washing buffer and poured out the liquid. Then other steps were done by the kit instruction. The mean lower detection limit of the Euroclone AFM1 test was 5 ppt. Data were analysed using the software PASW-18, with descriptive statistical methods (calculation of the pollution, the mean and Standard Deviation) and tests of Mann-Whitney, Kruskal-Wallis and the correlation coefficient.
RESULTS
Our results showed out of 87 breast milk samples, 24 were contaminated by aflatoxin M1 that is, the mean concentration levels of aflatoxin M1 were 0.56 ± 1.23 and ranging from 0.13 to 4.91 pg/ml [Table 1].
Table 1.
Occurrence of AFM1 in mother's breast milk

Mean and standard deviation of data related to anthropometric characteristics of 87 mothers and their infants and their correlation with aflatoxin M1 concentration are presented in Table 2. In this study, 11.5%, 28.7% and 5.7% of the mothers were respectively underweight, overweight and obese and 54% of mothers had a normal BMI. Also, 55 (63.2%) and 52 (59.8%) of mothers worked on farms and livestock, respectively. Twenty (23%) mothers also had natural miscarriage. Besides, in terms of education, 57 (65.5%), 24 (27.6%) and 6 (6.9%) were high school drop-outs, had high school diploma, and had higher education, respectively.
Table 2.
Maternal and infant's descriptive data and their correlation with the Aflatoxin M1 Concentration in breast milk samples
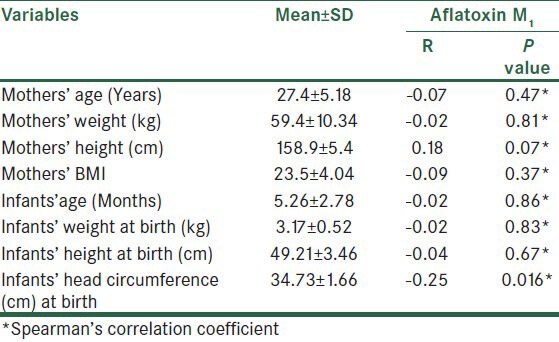
In the present study, the relationship between the concentration of aflatoxin M1 and the villages being sampled, was significant (P = 0.005). As shown in Table 2, Spearman's correlation test showed that there is a significant reverse linear relationship between aflatoxin M1 and infants’ head circumference (r = −0.25 and P = 0.016). However, based on this test, no significant relationship was observed between aflatoxin M1 concentration with other variables related to mother and child [Table 2]. Non-parametric Mann-Whitney test showed that in the studied mothers, the relationship between the concentration of aflatoxin M1 with livestock, farming activities and abortion was not significant (P > 0.05) and non-parametric Kruskal-Wallis test showed that no relationship was observed between the level of mothers’ education with the concentrations of aflatoxin M1 (P = 0.78).
DISCUSSION
Spore of different fungi including Aspergillus, Penicillium and Fusarium easily contaminate agricultural products under appropriate conditions during various stages of planting, growing and harvesting. Humans and animals are exposed to receiving fungal toxins due to consumption of contaminated foods.[15] Exposure of human to aflatoxins can be determined by a combination of food analysis and food intake studies or by monitoring levels of aflatoxins in biological fluids. Monitoring the levels of aflatoxins in biological fluids is more reliable indicator of actual exposure.[6] Aflatoxin M1 is considerably toxic and carcinogenic. However, the health risk of this toxin has not been well assessed in breast-fed infants.[16] The presence of aflatoxin M1 in the breast milk indicates that mother has consumed foods contaminated with Aflatoxin B1, and her embryo or her infant exposed with the contaminated milk.[5,17] Considering the fact that mother milk with natural and healthful properties is unique for nutrition of an infant, breast feeding is encouraging all over the world yet. People including nursing mothers in lactating period, are exposed with different naturally occurring and/or synthetic contaminants, and nearly all nutrients are also polluted with these types of contaminants in different degrees. Therefore, importance of feeding with natural and safe foods including milk is becoming popular day by day.[18]
In our study, aflatoxin M1 has a significant reverse relationship with infants’ head circumference at birth (P = 0.016). However, in previous studies from Iran, like those by Mahdavi[19] in Tabriz and Sadeghi[20] in Tehran, the relationship between the infants’ height and this toxin was reported significant (P < 0.05). In our study, the relationship between mother's height and aflatoxin M1 was not significant (P = 0.07), however, this relationship might become significant in a study with more samples.
As our results demonstrated, out of 87 samples, 24 samples (27.6%) were positive for AFM1. Aflatoxin M1 concentration in this study was less than that found in a study in Egypt with ranges of 6.3-497 pg/ml and 4.2-108 pg/ml.[21] The contamination rate and range in the present study were less than those in Egypt (36% of contamination with range of (10.27-21.43 pg/ml).[22] The mean of aflatoxin M1 concentration in this study was reported lower than that in other studies such as 71 pg/ml in Victoria,[6] 560 pg/ml in the United Arab Emirates,[9] 664 pg/ml in Thailand,[6] 2100-9200 pg/ml in Gambia,[5] 20-1816 ng/l in Liverpool, Britain[23] and 6.96 pg/ml in Tabriz.[19] Besides, the frequency of aflatoxin M1 contamination in this study was reported lower than that in Ahwaz with 1300-12500 pg/ml.[24] A reason may be the hot and humid climate of Khuzestan, which provides appropriate conditions for growing fungi on the food and agricultural products and also fungal contaminations. However, in the present study, the studied region has a temperate cold and dry weather which may provide more restricted conditions for the growth of aflatoxigenic species of Aspergillus and the reason for the low incidence of AFM1 contamination in milk of mothers in this region may contribute to this issue. The number and prevalence percentage of AFM1 contamination of mothers’ milk in a study in Tabriz consisted of 20 samples and 22%, respectively which to a great extent is consistent with the present study and perhaps, it is due to similarities of climatic conditions of both the regions (cold weather).
CONCLUSION
Based on the results of this study, the milk samples were contaminated with aflatoxin M1 which can have some adverse effects on infants’ growth parameters. However restriction of breast feeding is not an acceptable advice for mothers. Specific regulations for control of AFB1 in feeds and a systematic program monitoring of Aflatoxin M1 in milks is emphasized to reduce the level of such toxins. This requires a regular program to prevent the growth of the toxigenic fungi in all agricultural and food products. More investigations are necessary to determine the level of this toxin in human body fluids and nutrition diets to find the relationship between this toxin and health parameters.
ACKNOWLEDGMENTS
This study was supported by a grant no. 390272, Isfahan University of Medical Sciences, Isfahan, Iran. This study would not have been possible without the help and participation of the health centers and all mothers who volunteered their milk samples. Many thanks for cooperating of Shiraz University of medical Sciences and all of the staffs in health centers of Khorrambid, Iran.
Footnotes
Source of Support: This study was supported by a grant no. 390272, Isfahan University of Medical Sciences, Isfahan, Iran.
Conflict of Interest: None declared.
REFERENCES
- 1.WHO (World Health Organization) Geneva, Switzerland: World Health Organization; 2003. Global strategy for infant and young child feeding. [Google Scholar]
- 2.Jensen AA, Slorach SA. Boston: CRC Press; 1991. Levels and trends of environmental chemicals in human milk. [Google Scholar]
- 3.Jørgensen K, Rasmussen G, Thorup I. Ochratoxin A in Danish cereals 1986-1992 and daily intake by the Danish population. Food Addit Contam. 1996;13:95–104. doi: 10.1080/02652039609374384. [DOI] [PubMed] [Google Scholar]
- 4.Speijers GJA, Van Egmond HP. Worldwide ochratoxin a levels in food and feeds. In: Creppy EE, Castegnaro M, Dirheimer G, editors. Human Ochratoxicosis and Its Pathologies. Vol. 231. Colloque INSERM/John Libbey Eurotext; 1993. pp. 85–100. [Google Scholar]
- 5.Zarba A, Wild CP, Hall AJ, Montesano R, Hudson GJ, Groopman JD. Aflatoxin M1 in human breast milk from The Gambia, west Africa, quantified by combined monoclonal antibody immunoaffinity chromatography and HPLC. Carcinogenesis. 1992;13:891–4. doi: 10.1093/carcin/13.5.891. [DOI] [PubMed] [Google Scholar]
- 6.el-Nezami HS, Nicoletti G, Neal GE, Donohue DC, Ahokas JT. Aflatoxin M1 in human breast milk samples from Victoria, Australia and Thailand. Food Chem Toxicol. 1995;33:173–9. doi: 10.1016/0278-6915(94)00130-g. [DOI] [PubMed] [Google Scholar]
- 7.Galvano F, Pietri A, Bertuzzi T, Gagliardi L, Ciotti S, Luisi S, et al. Maternal dietary habits and mycotoxin occurrence in human mature milk. Mol Nutr Food Res. 2008;52:496–501. doi: 10.1002/mnfr.200700266. [DOI] [PubMed] [Google Scholar]
- 8.Navas SA, Sabino M, Rodriguez-Amaya DB. Aflatoxin M(1) and ochratoxin A in a human milk bank in the city of São Paulo, Brazil. Food Addit Contam. 2005;22:457–62. doi: 10.1080/02652030500110550. [DOI] [PubMed] [Google Scholar]
- 9.Abdulrazzaq YM, Osman N, Yousif ZM, Al-Falahi S. Aflatoxin M1 in breast-milk of UAE women. Ann Trop Paediatr. 2003;23:173–9. doi: 10.1179/027249303322296484. [DOI] [PubMed] [Google Scholar]
- 10.IARC (International Agency for Research on Cancer) IARC Monograph on the Evaluation of Carcinogenic Risks to Humans. Vol. 56. Lyon, France: World Health Organization; 1993. Some naturally occurring substances: Food items and constituents, heterocyclic aromatic amines and mycotoxins; pp. 245–395. [Google Scholar]
- 11.Dhanasekaran D, Shanmugapriya S, Thajuddin N. Aflatoxins and aflatoxicosis in human and animals. In: Guevara-Gonzaález RG, editor. Aflatoxins -Biochemistry and Molecular Biology Croatia. Croatia: InTech; 2011. pp. 221–54. [Google Scholar]
- 12.Wild CP, Pionneau FA, Montesano R, Mutiro CF, Chetsanga CJ. Aflatoxin detected in human breast milk by immunoassay. Int J Cancer. 1987;40:328–33. doi: 10.1002/ijc.2910400308. [DOI] [PubMed] [Google Scholar]
- 13.Galvano F, Galofaro V, Galvano G. Occurrence and stability of aflatoxin M1 in milk and milk products: a worldwide review. J. Food Protect. 1996;59:1079–90. doi: 10.4315/0362-028X-59.10.1079. [DOI] [PubMed] [Google Scholar]
- 14.Kuiper-Goodman T. Risk assessment of mycotoxins. In: Natori S, Hashimoto K, Ueno Y, editors. Mycotoxins and Phycotoxins. Amsterdam: Elsevier Science Publishers B. V; 1989. pp. 257–64. [Google Scholar]
- 15.Sherif SO, Salama EE, Abdel-Wahhab MA. Mycotoxins and child health: The need for health risk assessment. Int J Hyg Environ Health. 2009;212:347–68. doi: 10.1016/j.ijheh.2008.08.002. [DOI] [PubMed] [Google Scholar]
- 16.Hendrickse RG, Maxwell SM. Aflatoxins and child health in the tropics. [Last accessed on Jun 24 2012];Toxin Reviews. 1989 8:31–41. Available in: http://informahealthcare.com/doi/abs/10.3109/15569548909059736 . [Google Scholar]
- 17.Wild CP, Rasheed FN, Jawla MF, Hall AJ, Jansen LA, Montesano R. In-utero exposure to aflatoxin in west Africa. Lancet. 1991;337:1602. doi: 10.1016/0140-6736(91)93295-k. [DOI] [PubMed] [Google Scholar]
- 18.Gürbay A, Sabuncuoğlu SA, Girgin G, Sahin G, Yiğit S, Yurdakök M, et al. Exposure of newborns to aflatoxin M1 and B1 from mothers’ breast milk in Ankara, Turkey. Food Chem Toxicol. 2010;48:314–9. doi: 10.1016/j.fct.2009.10.016. [DOI] [PubMed] [Google Scholar]
- 19.Mahdavi R, Nikniaz L, Arefhosseini SR, Vahed Jabbari M. Determination of aflatoxin M(1) in breast milk samples in Tabriz-Iran. Matern Child Health J. 2010;14:141–5. doi: 10.1007/s10995-008-0439-9. [DOI] [PubMed] [Google Scholar]
- 20.Sadeghi N, Oveisi MR, Jannat B. Incidence of aflatoxin M1 in human breast milk in Tehran, Iran. [Last accessed on Jun 24 2012];Food control. 2009 20:75–8. Available in: http://www.sciencedirect.com/science/article/pii/S095671350800056X and ELSEVIER . [Google Scholar]
- 21.Polychronaki N, West RM, Turner PC, Amra H, Abdel-Wahhab M, Mykkänen H, et al. A longitudinal assessment of aflatoxin M1 excretion in breast milk of selected Egyptian mothers. Food Chem Toxicol. 2007;45:1210–5. doi: 10.1016/j.fct.2007.01.001. [DOI] [PubMed] [Google Scholar]
- 22.Polychronaki N, Turner P C, Mykkänen H, Gong Y, Amra H, Abdel-Wahhab M, et al. Determinants of aflatoxin M1 in breast milk in a selected group of Egyptian mothers. Food Addit Contam. 2006;23:700–8. doi: 10.1080/02652030600627222. [DOI] [PubMed] [Google Scholar]
- 23.Lamplugh SM, Hendrickse RG, Apeagyei F, Mwanmut DD. Aflatoxins in breast milk, neonatal cord blood, and serum of pregnant women. Br Med J (Clin Res Ed) 1988;296:968. doi: 10.1136/bmj.296.6627.968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Heidarinia A. PhD Thesis. Ahvaz: Iran Faculty of Medicine, Ahvaz University; 1995. Detection of aflatoxin M1 in breast milk. [Google Scholar]