

Abstract
Purpose
Tracheoesophageal Puncture (TEP) is an effective rehabilitation method for postlaryngectomy speech and has already been described as a procedure that is safely performed in the office. We review our long-term experience with office-based TEP over the past seven years in the largest cohort published to date.
Materials and Methods
A retrospective chart review was performed of all patients who underwent TEP by a single surgeon from 2005 through 2012, including office-based and operating room procedures. Indications for the chosen technique (office versus operating room) and surgical outcomes were evaluated.
Results
59 patients underwent 72 TEP procedures, with 55 performed in the outpatient setting and 17 performed in the operating room, all without complication. The indications for performing TEP’s in the operating room included 2 primary TEP’s, 14 due to concomitant procedures requiring general anesthesia, and 1 due to failed attempt at office-based TEP. 19 patients with prior rotational or free flap reconstruction successfully underwent office-based TEP.
Conclusions
TEP in an office-based setting with immediate voice prosthesis placement continues to be a safe method of voice rehabilitation for postlaryngectomy patients, including those who have previously undergone free flap or rotational flap reconstruction. Office-based TEP is now our primary approach for postlaryngectomy voice rehabilitation.
Keywords: Laryngectomy, Tracheoesophageal puncture, Voice rehabilitation, TEP
INTRODUCTION
Following total laryngectomy, a tracheoesophageal puncture (TEP) and subsequent placement of a voice prosthesis in the puncture tract is an effective way to restore speech.(1) The puncture may be performed primarily at the time of the laryngectomy, or as a secondary procedure subsequent to the laryngectomy. Though primary TEP may result in earlier acquisition of speech after laryngectomy, it may also be associated with higher rates of complications such as pharyngocutaneous fistula.(2) Additionally, secondary TEP is required when a patient’s TEP becomes dislodged and the prosthesis tract closes.
The secondary TEP procedure is traditionally performed in the operating room under general anesthesia via rigid esophagoscopy and the patient is sent home with a catheter placed through the puncture tract. After 3 to 5 days, the catheter is replaced with a TEP prosthesis by the speech language pathologist (SLP). With more widespread adoption of office-based unsedated trans-nasal esophagoscopy (TNE), several techniques for office-based unsedated TEP placement have been described.(3-6)
Office-based TEP has obvious benefits of decreased procedure time and cost as well as increased convenience for both surgeon and patient, especially since the prosthesis can be placed immediately after the puncture. We previously published our initial experience with office-based TEP in 13 patients, confirmed its feasibility, and found improved post-procedure outcomes compared to operating room TEP.(6) Additionally, for patients with laxity of the party wall and poor visualization, we developed a catheter system to allow placement with decreased risk to the posterior esophageal wall.(6) However, we did not perform office-based TEP in patients who had undergone rotational or free flap reconstruction. With more surgical experience and improved technical expertise, we continue to see the benefits of office-based TEP over operating room TEP, and have now expanded use of this puncture technique to patients who have undergone pharyngoesophageal reconstruction with a flap, including immediate prosthesis placement at the time of puncture. Office-based TEP has become the standard of care at our institution, resulting in the largest clinical experience reported in the literature to date. We undertook this investigation to evaluate our long-term experience with this technique over the past seven years.
MATERIALS AND METHODS
Approval for this study was obtained from the University of California, Los Angeles Institutional Review Board. A retrospective chart review was performed for all patients who underwent TEP by a single surgeon (DKC) from 2005 through 2012. Clinic and hospital records were examined, including history and physical examinations, operative notes, procedure notes, physician progress notes, and SLP progress notes. Historical data, procedure descriptions, and postoperative findings were recorded.
Prior to TEP placement, all patients underwent pre-TEP evaluation and counseling by an experienced SLP. Additionally, pre-TEP evaluation by the surgeon included TNE to evaluate adequate visualization and laxity of the party wall, evaluation of stoma size and location, and assessment for any esophageal stenosis and dysphagia symptoms. If a patient was deemed an inappropriate candidate for in-office TEP due to poor tolerance of endoscopy or unclear anatomy, or required additional procedures under general anesthesia, he or she was scheduled for TEP in the operating room.
TEP in the operating room was performed under general anesthesia. A 16-French introducer set was used to make the puncture and place a red rubber catheter through the puncture site as published previously.(6) The catheter remained in place for 3 to 5 days postoperatively, when it was replaced with a voice prosthesis by the SLP.
For those patients deemed appropriate for in-office TEP, the procedure was performed as previously described and is summarized in Table 1 and Figure 1.(7) Of note, the techniques of the procedure have evolved over the study period with a few important changes, highlighted below. First, the nasal cavity is anesthetized and decongested with topical 4% lidocaine and 1% neosynephrine. The tracheal stoma is also sprayed with 4% lidocaine solution. Less than 1 cc of 1% lidocaine with 1:100,000 parts epinephrine is injected to the posterior tracheal wall at the proposed puncture site, approximately 5 to 10 mm from the mucocutaneous junction. Additionally, 5 ml of viscous 2% lidocaine is applied to the base of tongue, and the patient allows this to flow into the esophagus. A transnasal esophagoscope was then passed through the nasal cavity and into the cervical esophagus (Figure 1). The esophagus was insufflated, and the proposed puncture site was identified using a 25 or 27 gauge needle. Under direct visualization, a number 11 blade was passed through the party wall at this location, and was turned 180 degrees within the stab incision (without withdrawing the blade) once visualized within the esophageal lumen. A hemostat was then passed through the puncture site and spread widely, which reduced the chances of the subsequently placed dilator encountering resistance or falling into a false tract. The puncture site was then dilated with an 18 French TEP dilator, followed by sizing with a voice prosthesis sizer. This was followed by immediate placement of the voice prosthesis using a gel-cap insertion system. At the conclusion of the procedure, the patient was taken to a counseling room to discuss TEP voicing and care by the assisting SLP.
Table 1.
Surgical Steps of Unsedated Tracheoesophageal Puncture (TEP) and Prosthesis Placement in the Office
| 1 | Local anesthesia of nasal cavity, pharynx, and stoma |
| 2 | Transnasal esophagoscopy performed to the level of the cervical esophagus |
| 3 | Identification of the puncture site using a 27-gauge needle (Figure 1A) |
| 4 | #11 blade used to make a stab incision at this location, followed by 180 degree rotation of the blade (Figure 1B) |
| 5 | Hemostat used to spread puncture site (Figure 1C) |
| 6 | Insertion of 18 French TEP dilator (Figure 1D) |
| 7 | Prosthesis sizer used to assess party wall thickness (Figure 1E) |
| 8 | Prosthesis placed by SLP using standard gel-cap insertion system (Figure 1F) |
Figure 1. View of Surgical Steps as Seen from the Transnasal Esophagoscope.
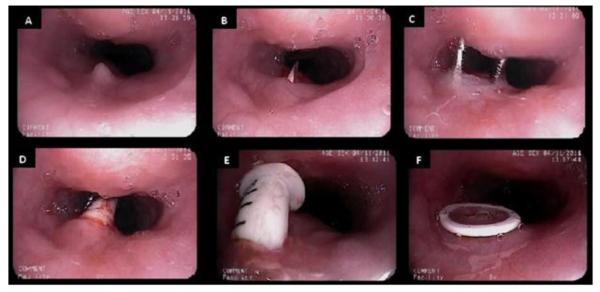
A. A 27 gauge needle is placed at proposed TEP site. B. A #11 blade is passed through party wall into esophageal lumen. C. Hemostat is spread widely within puncture site. D. 18 French TEP dilator is passed through puncture site. E. TEP prosthesis sizer is placed to determine size of prosthesis. F. Prosthesis is placed and visualized until gel-cap dissolves.
RESULTS
Within the study period, 72 TEP procedures were performed on 59 patients. 55 (76.4%) TEP’s were performed in the office, and 17 (23.6%) TEP’s were performed in the operating room. Office-based TEP’s were performed in times ranging from 2-15 minutes. Procedures in the operating room required in-room times ranging from approximately 45 minutes to 1.5 hours. There were no complications from the surgery. Patient demographics are presented in Table 2.
Table 2.
Tracheoesophageal Puncture Patients
| All Cases | Operating Room | Office-based | ||||
|---|---|---|---|---|---|---|
| N | (%) | N | (%) | N | (%) | |
| Number of Cases | 72 | (100.0%) | 17 | (23.6%) | 55 | (76.4%) |
| Average Age | 67 | 64 | 68 | |||
| Prior Radiation | 55 | (76.4%) | 13 | (76.5%) | 42 | (76.4%) |
| Prior Laryngeal or Hypopharyngeal Cancer |
67 | (93.1%) | 16 | (94.1%) | 51 | (92.7%) |
| Flap Reconstruction | 26 | (36.1%) | 7 | (41.2%) | 19 | (34.5%) |
| Pectoralis | 7 | 2 | 5 | |||
| Radial Forearm | 10 | 3 | 7 | |||
| Anterolateral Thigh | 8 | 2 | 6 | |||
| Latissimus | 1 | 0 | 1 | |||
| Failed Prior Operating Room Attempt |
2 | (2.8%) | 0 | (0.0%) | 2 | (3.6%) |
| Previous TEP Tract Closed (All Patients) |
24 | (33.3%) | 6 | (35.3%) | 18 | (32.7%) |
| Previous TEP Tract Closed (Initial TEP by Senior Author) |
13 | (18.1%) | 3 | (23.1%) | 10 | (76.9%) |
24 (33.3%) TEP’s were performed on patients who had a prior TEP that had closed. 10 (16.9%) patients underwent multiple TEP placements by the senior author. Of these repeat patients, 8 underwent a second TEP placement, 1 patient required two additional TEP placements, and 1 patient required three additional TEP placements. All thirteen repeat procedures were for accidental loss of TEP. Ten of these were performed in the office, and three were performed in the operating room.
Of the 17 TEP’s performed in the operating room, 2 were performed at the time of laryngectomy. 14 patients were taken to the operating room for secondary TEP because of additional planned concurrent procedures, including cricopharyngeal myotomy, esophageal dilation, and wide local excision of skin cancer. Only 1 patient was taken to the operating room solely for TEP placement, following a failed attempt in the office. This was due to severe collapse of the tracheoesophageal party wall and excessive secretions, resulting in inadequate visualization during the procedure. Since this single failed attempt in 2011, all subsequent TEP’s (13 consecutive cases) have been successfully performed in the office.
Early in the study period, most patients who had previously undergone free flap or rotational flap reconstruction were taken to the operating room for TEP with concurrent esophageal dilation at the anastomotic site. More recently, patients with prior flap reconstruction have had in-office TEP placements (and dilations) without difficulty or complication. 26 (36.1%) cases were for patients who were status post free or rotational flap reconstruction, and 19 of these TEP’s were successfully performed in the office. Additionally, we did not start applying viscous lidocaine to the tongue base until later in the study period. We found that the application of 2% viscous lidocaine to the tongue base improved patient tolerance of the procedure, and reduced gagging that was encountered in patients who previously considered office-based esophageal procedures to be difficult and uncomfortable.
There were no major complications in any of the office or operating room TEP procedures, although one office-based procedure was aborted and later performed in the operating room (as discussed above). There was one documented problem of excess granulation tissue formation. This patient developed such severe granulation tissue at the TEP site that he never attained adequate speech, and his prosthesis was subsequently removed. 5 patients decided to no longer use TEP speech after the prosthesis was placed. Of these 5 patients, 3 had fully intelligible speech with a TEP as judged by the SLP based on perceptual evaluation; however they chose to have the TEP removed as they did not like the TEP voice and/or maintenance required of the prosthesis. One patient developed severe stomal stenosis, making TEP speech difficult, and had the TEP removed. The single patient who underwent TEP placement 3 times due to accidental loss had speech that was documented as poorly intelligible after each placement. This patient had a prior near-total glossectomy in addition to his laryngectomy, causing marked dysarthria, which contributed greatly to his intelligibility; however, this patient preferred TEP speech to alternative forms of communication.
DISCUSSION
Primary TEP is at times preferred over secondary TEP, but it is not always feasible. Even in situations where primary TEP placement is performed, secondary TEP may eventually be necessary, as demonstrated in one-third of our patient population. Even with regular maintenance, accidental extrusion, failure to replace, and fistula site closure does occur.(8) These patients will require a revision secondary TEP placement in order to regain tracheoesophageal speech. It is the senior author’s experience that the timing of the revision puncture depends on resolution of any granulation tissue at the prior puncture site. Once all granulation tissue is completely resolved, we will perform the revision puncture. This has been done as soon as three weeks after closure without complications.
While secondary TEP in the operating room is still a reasonable option, laryngectomy patients often pose a challenge. The cardiac and pulmonary comorbidities of smoking often accompanying laryngeal cancer may preclude general anesthesia. Additionally, radiation-induced fibrosis may prevent adequate mouth opening or neck extension for rigid esophagoscopy. Of note, for 2 of our patients who underwent TEP in the operating room (concurrent with other procedures requiring general anesthesia), the procedure was performed with a trans-nasal esophagoscope, as would be done in the office, due to inadequate neck extension. These reasons, as well as the decreased cost and increased convenience, have been the impetus for performing TEP’s in the office setting in an unsedated manner.
Office-based TEP was first introduced more than ten years ago, and several technique modifications have since been presented in the literature.(3, 9-11) With our experience, we have gained further surgical expertise and management strategies that has led to increased patient comfort, improved technique, and broadened the indications for the procedure. Changes from our prior publications also include adding topical anesthesia to the tongue base and cervical esophagus. This adds to patient comfort and decreases gagging, which has drastically improved visualization for the procedure. Previously, the incision made with the number 11 blade was described as a cruciate incision; however we now find it simpler to simply pass the blade once and turn it 180 degrees once in place, rather than pass it twice through the party wall. This reduces the chances of creating a false passage. What was previously described as a gentle spread with a hemostat after the incision is made is now a very generous spreading motion with the hemostat. By spreading widely, we find that there is a lower probability of the dilator, sizer, or prosthesis encountering resistance during insertion and entering into a false tract. Interestingly, we do not experience leakage around the prosthesis despite this generous spread, as confirmed by a swallow test performed in the office immediately after voice prosthesis placement.
A difference in our technique from that described by other authors is that we place the TEP prosthesis immediately after creating the puncture. We have previously published the benefits of immediate prosthesis placement, including improved prosthesis sizing and fewer prosthesis replacements needed before achieving stable prosthesis length.(7) Others have also described immediate placement of a voice prosthesis at the time of primary TEP, with successful restoration of voice.(12-13) We do, however, place a rubber catheter in the tract on the rare occasion that the procedure requires use of guidewire technique due to party wall collapse. The latter technique, which we previously described, has not been required in any case performed in the last 12 months.(6) Since 2011, all TEP’s by the senior author (DKC) have been performed successfully in the clinic with none requiring a trip to the operating room. In fact, one TEP that could not be performed in the operating room by another experienced surgeon due to bulky free flap reconstruction was successfully performed by the senior author in the office.
Prior to our office-based TEP experience, our initial follow-up algorithm was for the SLP to see patients every two weeks for the first two month after prosthesis placement, primarily for prosthesis re-sizing. We found that this frequency was no longer necessary after we began performing office-based TEP with immediate voice prosthesis placement. The patient now sees the SLP at one month after initial placement, and thereafter on an as needed basis. The most common reason for voice prosthesis replacement is due to yeast colonization, resulting in an average lifespan of four months.(14) This has been consistent with our own experience with prosthesis replacement, regardless of the manner of initial puncture.
Though office-based TEP has been reported multiple times in the literature to be a feasible procedure, most studies are preliminary and technical, reporting only a few cases, and without long-term follow-up. As office-based TEP has become the standard practice at our institution, we are able to report the largest series to date of office-based TEP, including cases involving flap-reconstructed pharyngoesophageal segments, which we previously considered a contra-indication to office-based TEP. This was due to concerns regarding the altered pharyngoesophageal anatomy, fear of damaging the vascular pedicle, and fear of not being able to adequately insufflate the esophagus at the operative site. However, we performed 19 out of 26 TEP’s for such patients in the office during the study period, suggesting that this is a safe and reliable option.
Weaknesses of this study include its retrospective nature and the relatively small number of TEP’s performed in the operating room compared to the office, which limits any statistical analysis. Though the procedures were all performed by a single surgeon, evolution of surgical technique over seven years is an additional variable.
CONCLUSION
TEP in an office-based setting continues to be a safe method of voice rehabilitation for post-laryngectomy patients, as seen with long-term follow-up. Office based TEP is an appropriate option for those who have previously undergone free flap or rotational flap reconstruction and is now our primary approach to all post-laryngectomy voice rehabilitation.
Acknowledgments
Financial Disclosure: This study was supported by Grant No. RO1 DC011300 from the National Institutes of Health.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of Interest: None
The authors have no other financial disclosures to make.
This article was presented as a poster at the 2013 American Broncho-Esophagological Association section of the Combined Otolaryngology Spring Meetings on April 10, 2013, in Orlando, FL.
Author Contributions: Jennifer Bergeron: collection and review of data, writing manuscript; Nausheen Jamal: collection and review of data, writing/editing manuscript; Andrew Erman: review of data, review/editing manuscript; Dinesh Chhetri: review of data, review/editing manuscript.
REFERENCES
- [1].Singer MI, Blom ED. An endoscopic technique for restoration of voice after laryngectomy. Ann Otol Rhinol Laryngol. 1980;89:529–33. doi: 10.1177/000348948008900608. [DOI] [PubMed] [Google Scholar]
- [2].Emerick KS, Tymycx L, Bradford C, Lyden TH, Chepeha DB, Wolf GT, Teknos TN. Primary versus secondary tracheoesophageal puncture in salvage total laryngectomy following chemoradiation. Otolaryngol Head Neck Surg. 2009;140:386–90. doi: 10.1016/j.otohns.2008.10.018. [DOI] [PubMed] [Google Scholar]
- [3].Bach KK, Postma GN, Koufman JA. In-Office Tracheoesophageal Puncture Using Transnasal Esophagoscopy. Laryngoscope. 2003;113:173–6. doi: 10.1097/00005537-200301000-00032. [DOI] [PubMed] [Google Scholar]
- [4].Doctor VS. In-office unsedated tracheoesophageal puncture. Current Opinion in Otolaryngol Head Neck Surg. 2007;15:405–8. doi: 10.1097/MOO.0b013e3282f151e6. [DOI] [PubMed] [Google Scholar]
- [5].Doctor VS, Enepekides DJ, Farwell DG, Belafsky PC. Transnasal oesophagoscopy-guided in-office secondary tracheoesophageal puncture. J Laryngol & Otol. 2008;122:303–6. doi: 10.1017/S0022215107000084. [DOI] [PubMed] [Google Scholar]
- [6].Sidell D, Ghadiali M, Chhetri DK. Unsedated office-based tracheoesophageal puncture using a novel guidewire technique. Otolaryngol Head Neck Surg. 2010;142:284–5. doi: 10.1016/j.otohns.2009.09.030. [DOI] [PubMed] [Google Scholar]
- [7].Sidell D, Shamouelian D, Erman A, Gerratt BR, Chhetri D. Improved Tracheoesophageal Prosthesis Sizing in Office-Based Tracheoesophageal Puncture. Annals Otol Rhinol Laryngol. 2010;119:37–41. doi: 10.1177/000348941011900107. [DOI] [PubMed] [Google Scholar]
- [8].Izdebski K, Reed CG, Ross JC, Hilsinger RL. Problems With Tracheoesophageal Fistula Voice Restoration in Totally Laryngectomized Patients. Arch Otolaryngol Head Neck Surg. 1994;120:841–5. doi: 10.1001/archotol.1994.01880320042010. [DOI] [PubMed] [Google Scholar]
- [9].Erenstein SRJ, Schouwenburg PF. Secondary Tracheoesophageal Puncture With Local Anesthesia. Laryngoscope. 2002;112:634–7. doi: 10.1097/00005537-200204000-00008. [DOI] [PubMed] [Google Scholar]
- [10].Postma GN, Cohen JT, Belafsky PC, Halum SL, Gupta SK, Back KK, Koufman JA. Transnasal Esophagoscopy: Revisited (over 700 Consecutive Cases) Laryngoscope. 2005;115:321–3. doi: 10.1097/01.mlg.0000154741.25443.fe. [DOI] [PubMed] [Google Scholar]
- [11].Snelling JD, Price T, Montgomery PQ, Blagnys BL. How we do it: Secondary tracheoesophageal puncture under local anaesthetic, using trans-nasal flexible laryngooesophagoscope (TNFLO) Logopedics Phoniatrics Vocology. 2007;32:80–2. doi: 10.1080/14015430600712205. [DOI] [PubMed] [Google Scholar]
- [12].Deschler DG, Bunting GW, Lin DT, Emerick K, Rocco J. Evaluation of voice prosthesis placement at the time of primary tracheoesophageal puncture with total laryngectomy. Laryngoscope. 2009;119(7):1353–7. doi: 10.1002/lary.20490. [DOI] [PubMed] [Google Scholar]
- [13].Divi V, Lin DT, Emerick K, Rocco J, Deschler DG. Primary TEP placement in patients with laryngopharyngeal free tissue reconstruction and salivary bypass tube placement. Otolaryngol Head Neck Surg. 2011;144(3):474–6. doi: 10.1177/0194599810391960. [DOI] [PubMed] [Google Scholar]
- [14].Bauters TGM, Moerman M, Vermeersch H, Nelis HJ. Colonization of voice prostheses by Albicans and non-Albicans Candida species. Laryngoscope. 2002;112:708–12. doi: 10.1097/00005537-200204000-00021. [DOI] [PubMed] [Google Scholar]