

Abstract
Background
Diclofenac is a non-steroidal anti-inflammatory drug (NSAID), available as a potassium salt (immediate-release) or sodium salt (delayed-release). This review updates an earlier review published in The Cochrane Database of Systematic Reviews (Issue 2, 2004) on ‘Single dose oral diclofenac for postoperative pain’.
Objectives
To assess single dose oral diclofenac for the treatment of acute postoperative pain.
Search methods
Cochrane CENTRAL, MEDLINE, EMBASE, Biological Abstracts, the Oxford Pain Relief Database, and reference lists of articles were searched; last search December 2008.
Selection criteria
Randomised, double-blind, placebo-controlled clinical trials of single dose, oral diclofenac (sodium or potassium) for acute postoperative pain in adults.
Data collection and analysis
Two review authors independently assessed studies for inclusion and quality, and extracted data. The area under the pain relief versus time curve was used to derive the proportion of participants with at least 50% pain relief over 4 to 6 hours, using validated equations. Relative benefit (risk) and number needed to treat to benefit (NNT) were calculated. Information on adverse events, time to remedication, and participants needing additional analgesia was also collected.
Main results
Fifteen studies (eight additional studies) with 1512 participants more than doubled the information available at each dose. Overall 50% to 60% of participants experienced at least 50% pain relief over 4 to 6 hours at any dose with diclofenac, compared to 10 to 20% with placebo, giving NNTs of about 2.5 for doses of 25 mg to 100 mg (similar to earlier review); no dose response was demonstrated. At 50 mg and 100 mg, NNTs for diclofenac potassium (2.1 (1.8 to 2.4) and 1.9 (1.7 to 2.2)) were significantly lower (better) than for diclofenac sodium (6.7 (4.2 to 17) and 4.5 (3.2 to 7.7)). The median time to use of rescue medication was 2 hours for placebo, 4.3 hours for diclofenac 50 mg and 4.9 hours for diclofenac 100 mg. Adverse events were reported at a similar rate to placebo, with no serious events.
Authors’ conclusions
Oral diclofenac is an effective single-dose treatment for moderate to severe postoperative pain. Significantly more participants experienced at least 50% pain relief over 4 to 6 hours with diclofenac potassium than with diclofenac sodium. There was no significant difference between diclofenac and placebo in the incidence of adverse events.
Medical Subject Headings (MeSH): Acute Disease; Administration, Oral; Anti-Inflammatory Agents, Non-Steroidal [*administration & dosage; adverse effects]; Chemistry, Pharmaceutical; Cyclooxygenase Inhibitors [administration & dosage; adverse effects]; Diclofenac [*administration & dosage; adverse effects]; Pain, Postoperative [*drug therapy]; Randomized Controlled Trials as Topic
MeSH check words: Adult, Humans
BACKGROUND
This review is an update of a previously published review in The Cochrane Database of Systematic Reviews (Issue 2, 2004) on ‘Single dose oral diclofenac for postoperative pain’ (Barden 2004a), which itself was an update of two earlier non-Cochrane reviews (Collins 1998; Collins 1999). The title now states that the review is limited to adults.
Acute pain occurs as a result of tissue damage either accidentally due to an injury or as a result of surgery. Acute postoperative pain is a manifestation of inflammation due to tissue injury. The management of postoperative pain and inflammation is a critical component of patient care. The aim of this series of reviews is to present evidence for relative analgesic efficacy through indirect comparisons with placebo, in very similar trials performed in a standard manner, with very similar outcomes, and over the same duration. Such relative analgesic efficacy does not in itself determine choice of drug for any situation or patient, but guides policy-making at the local level.
Recent reviews include lumiracoxib (Roy 2007) and celecoxib (Derry 2008), and will include updates of existing reviews like aspirin (Oldman 2000).
Single dose trials in acute pain are commonly short in duration, rarely lasting longer than 12 hours. The numbers of participants is small, allowing no reliable conclusions to be drawn about safety. To show that the analgesic is working it is necessary to use placebo (McQuay 2005). There are clear ethical considerations in doing this. These ethical considerations are answered by using acute pain situations where the pain is expected to go away, and by providing additional analgesia, commonly called rescue analgesia, if the pain has not diminished after about an hour. This is reasonable, because not all participants given an analgesic will have significant pain relief. Approximately 18% of participants given placebo will have significant pain relief (Moore 2005), and up to 50% may have inadequate analgesia with active medicines. The use of additional or rescue analgesia is hence important for all participants in the trials.
Clinical trials measuring the efficacy of analgesics in acute pain have been standardised over many years. Trials have to be randomised and double blind. Typically, in the first few hours or days after an operation, patients develop pain that is moderate to severe in intensity, and will then be given the test analgesic or placebo. Pain is measured using standard pain intensity scales immediately before the intervention, and then using pain intensity and pain relief scales over the following 4 to 6 hours for shorter acting drugs, and up to 12 or 24 hours for longer acting drugs. Pain relief of half the maximum possible pain relief or better (at least 50% pain relief) is typically regarded as a clinically useful outcome. For patients given rescue medication it is usual for no additional pain measurements to be made, and for all subsequent measures to be recorded as initial pain intensity or baseline (zero) pain relief (baseline observation carried forward). This process ensures that analgesia from the rescue medication is not wrongly ascribed to the test intervention. In some trials the last observation is carried forward, which gives an inflated response for the test intervention compared to placebo, but the effect has been shown to be negligible over 4 to 6 hours (Moore 2005). Patients usually remain in the hospital or clinic for at least the first six hours following the intervention, with measurements supervised, although they may then be allowed home to make their own measurements in trials of longer duration.
Clinicians prescribe non-steroidal anti-inflammatory drugs (NSAIDs) on a routine basis for a range of mild-to-moderate pain. NSAIDs are the most commonly prescribed analgesic medications worldwide, and their efficacy for treating acute pain has been well demonstrated (Moore 2003). They reversibly inhibit cyclooxygenase (prostaglandin endoperoxide synthase), the enzyme mediating production of prostaglandins and thromboxane A2 (Fitzgerald 2001). Prostaglandins mediate a variety of physiological functions such as maintenance of the gastric mucosal barrier, regulation of renal blood flow, and regulation of endothelial tone. They also play an important role in inflammatory and nociceptive processes. However, relatively little is known about the mechanism of action of this class of compounds aside from their ability to inhibit cyclooxygenase-dependent prostanoid formation (Hawkey 1999). Since NSAIDs do not depress respiration and do not impair gastrointestinal motility as do opioids (BNF 2002) they are clinically useful for treating pain after minor surgery and day surgery, and have an opiate-sparing effect after more major surgery (Grahame-Smith 2002).
Diclofenac is a benzene acetic acid derivative used to treat the pain and swelling associated with rheumatic disorders since 1974 (Fineschi 1997), and is one of the most widely used NSAIDs in the world, especially outside the USA. Almost eight million prescriptions for diclofenac were dispensed in England in 2007 (PACT 2007), the most common doses being 75 mg and 150 mg given daily in divided doses. It is available in two different formulations, diclofenac potassium and diclofenac sodium, with the sodium salt used much more frequently (7.9 of the eight million prescriptions in England in 2007). Diclofenac potassium is formulated to be released and absorbed in the stomach. Diclofenac sodium, usually distributed in enteric-coated tablets, resists dissolution in low PH gastric environments, releasing instead in the duodenum (Olson 1997). The potassium and sodium formulations present different hypothetical advantages; the immediate-release potassium formulation might provide pain relief more quickly (Bakshi 1992), whereas the delayed-release formulation might minimise gastric exposure theoretically minimising the risk of adverse gastrointestinal events (this is unlikely as NSAID-related gastrointestinal adverse effects are more closely linked with systemic (overall) concentration). The clinical bearing of these differences has yet to be established.
A major concern regarding the use of conventional NSAIDs postoperatively is the possibility of bleeding from both the operative site (because of the inhibition of platelet aggregation) (Forrest 2002) and from the upper gastrointestinal tract, (especially in patients stressed by surgery, the elderly, frail, or dehydrated). Other potentially serious adverse events include acute liver injury, acute renal injury, heart failure, and adverse reproductive outcomes (Hernández-Díaz 2001). Research has also implicated diclofenac in haematological abnormalities (Martindale 1996). However, such complications are more likely to occur with chronic use and NSAIDs generally present fewer risks if used in the short term, as in the treatment of postoperative pain (Rapoport 1999).
The previous review included seven studies in which 581 participants were treated with diclofenac and 364 with placebo. For doses of 25 mg to 100 mg, two to three participants needed to be treated for one to achieve at least 50% pain relief who would not have done so with placebo. The median time to use of rescue medication was 7.2 hours with diclofenac 100 mg, compared to 2.0 hours for placebo. There was no significant difference in numbers of participants experiencing any adverse event between diclofenac and placebo. Since that review, a number of new studies have been published, which should permit calculation of more robust estimates of both efficacy and harm.
OBJECTIVES
To evaluate the analgesic efficacy and safety of oral diclofenac in the treatment of acute postoperative pain, using methods that permit comparison with other analgesics evaluated in the same way, using criteria of efficacy recommended by an in-depth study at the individual patient level (Moore 2005).
METHODS
Criteria for considering studies for this review
Types of studies
Studies were included if they were full publications of double blind trials of a single dose oral diclofenac against placebo for the treatment of moderate to severe postoperative pain in adults, with at least ten participants randomly allocated to each treatment group. Multiple dose studies were included if appropriate data from the first dose were available, and cross-over studies were included provided that data from the first arm were presented separately.
Studies were excluded if they were:
posters or abstracts not followed up by full publication;
reports of trials concerned with pain other than postoperative pain (including experimental pain);
studies using healthy volunteers;
studies where pain relief was assessed by clinicians, nurses or carers (i.e., not patient-reported);
studies of less than 4 hours’ duration or which failed to present data over 4 to 6 hours post-dose.
Types of participants
Studies of adult participants (15 years old or above) with established moderate to severe postoperative pain were included. For studies using a visual analogue scale (VAS), pain of at least moderate intensity was assumed when the VAS score was greater than 30 mm (Collins 1997). Studies of participants with postpartum pain were included provided the pain investigated resulted from episiotomy or Caesarean section (with or without uterine cramp). Studies investigating participants with pain due to uterine cramps alone were excluded.
Types of interventions
Orally administered diclofenac sodium or potassium with matched placebo administered as a single oral dose for post-operative pain.
Types of outcome measures
Data collected included the following:
characteristics of participants;
pain model;
patient-reported pain at baseline (physician, nurse, or carer reported pain will not be included in the analysis);
patient-reported pain relief and/or pain intensity expressed hourly over 4 to 6 hours using validated pain scales (pain intensity and pain relief in the form of VAS or categorical scales, or both), or reported total pain relief (TOTPAR) or summed pain intensity difference (SPID) at 4 to 6 hours;
patient-reported global assessment of treatment (PGE), using a standard five-point scale;
number of participants using rescue medication, and the time of assessment;
time to use of rescue medication;
withdrawals - all cause, adverse event;
adverse events - participants experiencing one or more, and any serious adverse event, and the time of assessment.
Search methods for identification of studies
For the earlier review the following electronic databases were searched using a sensitive search strategy:
The Cochrane Library (Issue 3, 2001).
The Specialised Register of the Cochrane Pain, Palliative and Supportive Care group (November 2002).
MEDLINE (1966 to May 1996).
EMBASE (1980 to 1996).
Biological Abstracts (1985 to 1996).
PubMed (August 2001).
Oxford Pain database (Jadad 1996a).
For this update the following electronic databases were searched:
Cochrane CENTRAL (Issue 4, 2008).
MEDLINE via Ovid (1996 to December 2008).
EMBASE via Ovid (1996 to December 2008).
See Appendix 1 for the MEDLINE search strategy, Appendix 2 for the EMBASE search strategy and Appendix 3 for the CENTRAL search strategy.
Additional studies were sought in reference lists of retrieved articles and reviews.
Language
No language restriction was applied.
Unpublished studies
Abstracts, conference proceedings and other grey literature were not searched. Merck provided details of two unpublished studies for the original review, but manufacturers were not contacted for this update.
Data collection and analysis
Selection of studies
Two review authors independently assessed and agreed the search results for studies that might be included in the updated review. Disagreements were resolved by consensus or referral to a third review author.
Quality assessment
Two review authors independently assessed the included studies for quality using a five-point scale (Jadad 1996b).
The scale used is as follows:
Is the study randomised? If yes give one point.
Is the randomisation procedure reported and is it appropriate? If yes add one point, if no deduct one point.
Is the study double blind? If yes then add one point.
Is the double blind method reported and is it appropriate? If yes add 1 point, if no deduct one point.
Are the reasons for patient withdrawals and dropouts described? If yes add one point.
The results are described in the ‘Methodological quality of included studies’ section below, and ‘Characteristics of included studies’ table.
Data management
Data were extracted by two review authors and recorded on a standard data extraction form. Data suitable for pooling were entered into RevMan 5.0.16.
Data analysis
QUOROM guidelines were followed (Moher 1999). For efficacy analyses we used the number of participants in each treatment group who were randomised, received medication, and provided at least one post-baseline assessment. For safety analyses we used number of participants who received study medication in each treatment group. Analyses were planned for different doses. Sensitivity analyses were planned for pain model (dental versus other postoperative pain), trial size (39 or fewer versus 40 or more per treatment arm), and quality score (two versus three or more), salt preparation (Na versus K salt), and formulation (tablet versus dispersible). A minimum of two studies and 200 participants were required for any analysis (Moore 1998).
Primary outcome
Number of participants achieving at least 50% pain relief
For each study, mean TOTPAR (total pain relief) or SPID (summed pain intensity difference) for active and placebo groups were converted to %maxTOTPAR or %maxSPID by division into the calculated maximum value (Cooper 1991). The proportion of participants in each treatment group who achieved at least 50%maxTOTPAR was calculated using verified equations (Moore 1996; Moore 1997a; Moore 1997b). These proportions were then converted into the number of participants achieving at least 50%maxTOTPAR by multiplying by the total number of participants in the treatment group. Information on the number of participants with at least 50%maxTOTPAR for active treatment and placebo was then used to calculate relative benefit (RB) and number needed to treat to benefit (NNT).
Pain measures accepted for the calculation of TOTPAR or SPID were:
five-point categorical pain relief (PR) scales with comparable wording to “none, slight, moderate, good or complete”;
four-point categorical pain intensity (PI) scales with comparable wording to “none, mild, moderate, severe”;
VAS for pain relief;
VAS for pain intensity.
If none of these measures were available, numbers of participants reporting “very good or excellent” on a five-point categorical global scale with the wording “poor, fair, good, very good, excellent” were taken as those achieving at least 50% pain relief (Collins 2001). Further details of the scales and derived outcomes are in the glossary (Appendix 4).
Secondary outcomes
1. Use of rescue medication
Numbers of participants requiring rescue medication were used to calculate relative risk and numbers needed to treat to prevent (NNTp) use of rescue medication for treatment and placebo groups. Median (or mean) time to use of rescue medication was used to calculate the weighted mean of the median (or mean) for the outcome. Weighting was by number of participants.
2. Adverse events
Numbers of participants reporting adverse events for each treatment group were used to calculate relative risk and numbers needed to treat to harm (NNH) estimates for:
any adverse event;
any serious adverse event (as reported in the study);
withdrawal due to an adverse event.
3. Withdrawals
Withdrawals for reasons other than lack of efficacy (participants using rescue medication - see above) and adverse events were noted, as were exclusions from analysis where data were presented.
Relative benefit or risk estimates were calculated with 95% confidence intervals (CI) using a fixed-effect model (Morris 1995). NNT, NNTp and NNH with 95% CI were calculated using the pooled number of events by the method of Cook and Sackett (Cook 1995). A statistically significant difference from control was assumed when the 95% CI of the relative benefit did not include the number one.
Homogeneity of studies was assessed visually (L’Abbé 1987). The z test (Tramèr 1997) was used to determine if there was a significant difference between NNTs for different doses of active treatment, or between groups in the sensitivity analyses.
RESULTS
Description of studies
See: Characteristics of included studies; Characteristics of excluded studies.
The earlier review included seven studies (Ahlstrom 1993; Bakshi 1992; Bakshi 1994; Herbertson 1995; Mehlisch 1995; Nelson 1994; Olson 1997). The new searches identified an additional nine potentially relevant studies. One (Tam 2001) was excluded after reading the full paper, and eight were included (Chang 2002; Cooper 1996; Desjardins 2004; Hersh 2004; Hofele 2006; Kubitzek 2003; Torres 2004; Zuniga 2004). In total 15 studies were included in this review update. Details are in the relevant ‘Characteristics of studies’ tables.
In the 15 included studies, a total of 1512 participants were treated with diclofenac and 793 with placebo.
Diclofenac 25 mg was used in four studies (Hersh 2004; Kubitzek 2003; Nelson 1994; Olson 1997), diclofenac 50 mg in 11 studies (13 treatment arms) (Ahlstrom 1993; Bakshi 1992; Bakshi 1994;Chang 2002; Cooper 1996; Herbertson 1995; Hersh 2004; Hofele 2006; Mehlisch 1995; Nelson 1994; Olson 1997), diclofenac 75 mg in one study (Torres 2004), and diclofenac 100 mg in seven studies (eight treatment arms) (Desjardins 2004; Herbertson 1995; Hersh 2004; Mehlisch 1995; Nelson 1994; Olson 1997;Zuniga 2004).
Thirteen studies used diclofenac tablets (Bakshi 1992; Bakshi 1994; Chang 2002; Cooper 1996; Desjardins 2004; Herbertson 1995; Mehlisch 1995; Nelson 1994; Olson 1997), three used a dispersible (drinkable) preparation (Ahlstrom 1993; Bakshi 1994;Hofele 2006), and one used a softgel preparation (Zuniga 2004). Three studies used diclofenac sodium (Na) (Chang 2002; Cooper 1996; Desjardins 2004), seven used diclofenac potassium (K) (Herbertson 1995; Hersh 2004; Hofele 2006; Kubitzek 2003;Mehlisch 1995; Nelson 1994; Olson 1997), two compared the same dose of Na and K salt preparations (Bakshi 1992; Zuniga 2004), one used the free acid (Bakshi 1994) and two did not specify the salt preparation used (Ahlstrom 1993; Torres 2004).
Eleven studies were in participants with dental pain following surgical extraction of one or more impacted third molars (Ahlstrom 1993; Bakshi 1992; Bakshi 1994; Chang 2002; Cooper 1996;Hersh 2004; Hofele 2006; Kubitzek 2003; Mehlisch 1995; Nelson 1994; Zuniga 2004), and one each in participants with pain following bunionectomy (Desjardins 2004), general gynaecological surgery (Herbertson 1995), post episiotomy (Olson 1997), and inguinal hernia (Torres 2004).
Trial duration was 6 hours in seven studies (Ahlstrom 1993; Bakshi 1992; Bakshi 1994; Cooper 1996; Hersh 2004; Kubitzek 2003;Nelson 1994), eight hours in three studies (Herbertson 1995;Mehlisch 1995; Olson 1997), 24 hours in four studies (Chang 2002; Desjardins 2004; Hofele 2006; Zuniga 2004), and 36 hours in one study (Torres 2004).
Risk of bias in included studies
Methodological quality of included studies
All included studies were both randomised and double blind. Five studies were given a quality score of five (Chang 2002; Desjardins 2004; Hersh 2004; Hofele 2006; Zuniga 2004), six a score of four (Ahlstrom 1993; Bakshi 1994; Kubitzek 2003; Nelson 1994;Mehlisch 1995; Olson 1997) and four a score of three (Bakshi 1992; Cooper 1996; Herbertson 1995; Torres 2004).
Full details are in the ‘Characteristics of included studies’ table.
Effects of interventions
All 15 included studies provided some data for quantitative analysis. Fourteen trials contributed data to the primary efficacy outcome. One trial looking at 75 mg dose (Torres 2004) did not report baseline pain intensity, so that SPID could not be calculated.
Number of participants achieving at least 50% pain relief (see Summary of results A)
Diclofenac 25 mg versus placebo
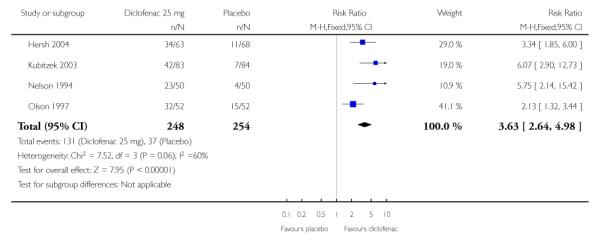
Four studies with 502 participants provided data (Hersh 2004;Kubitzek 2003; Nelson 1994; Olson 1997) (please see Table 1 and Figure 1).
The proportion of participants experiencing at least 50% pain relief over 4 to 6 hours with diclofenac 25 mg was 53% (131/248; range 46% to 62%).
The proportion of participants experiencing at least 50% pain relief with placebo was 15% (37/254; range 8% to 29%).
The relative benefit of treatment compared with placebo was 3.6 (2.6 to 5.0), giving an NNT for at least 50% pain relief over 4 to 6 hours of 2.6 (2.2 to 3.3).
Table 1.
Summary of outcomes: analgesia and rescue medication
| Analgesia | Rescue medication | |||||
|---|---|---|---|---|---|---|
| Study ID | Treatment | PI or PR | Number with 50% PR | PGR: v good or excellent | Median time to use (hr) | % using |
| Ahlstrom 1993 | 1) Diclofenac (soluble) 50 mg, n = 35 (2) Ibuprofen (tablets) 400 mg, n = 32 (3) Placebo, n = 30 |
TOTPAR 6: (1) 153 mm (3) 292 mm |
(1) 21/35 (3) 3/50 |
at 6 hours: (1) 23/35 (3) 5/30 |
no data | at 6 hours: (1) 40 (3) 77 |
| Bakshi 1992 | (1) Diclofenac K 50 mg, n = 51 (2) Diclofenac Na (enteric coated) 50 mg, n = 54 (3) Placebo, n = 46 |
TOTPAR 6: (1) 10 (2) 7.3 (3) 5.2 |
(1) 35/51 (2) 16/54 (3) 10/46 |
no usable data | no usable data | at 6 hours: (1) 33 (2) 41 (3) 59 |
| Bakshi 1994 | (1) Diclofenac (soluble) 50 mg, n = 83 (2) Ibuprofen 400 mg, n = 80 (3) Placebo, n = 82 |
TOTPAR 6: (1) 15.5 (3) 8.9 |
(1) 62/83 (3) 31/82 |
no usable data | Mean: (1) 5.35 (3) 3.36 |
at 6 hours: (1) 24 (3) 65 |
| Chang 2002 | (1) Diclofenac Na (enteric coated) 50 mg, n = 121 (2) Rofecoxib 50 mg, n = 121 (3) Placebo, n = 63 |
TOTPAR 6: (1) 5.8 (3) 4.3 |
(1) 32/121 (3) 8/63 |
no usable data | (1) 1.62 (3) 1.62 |
at 8 hours: (1) 67 (3) 76 |
| Cooper 1996 | (1) Diclofenac Na 50 mg, n = 18 (2) Misoprostol 200 μg, n = 21 (3) Diclofenac Na + misoprostol 50 mg/200 μg, n = 20 (4) Placebo, n = 11 |
TOTPAR 6: (1) 12.5 (4) 1.9 |
(1) 10/18 (4) 0/11 |
no usable data | Mean: (1) 4.68 (4) 2.11 |
no data |
| Desjardins 2004 | (1) Diclofenac Na 100 mg, n = 85 (2) Rofecoxib 50 mg, n = 85 (3) Placebo, n = 82 |
TOTPAR 6: (1) 4.8 (3) 2.9 |
(1) 13/85 (3) 4/82 |
at 8 hours: (1) 6/85 (3) 3/82 |
(1) 2.03 (3) 1.41 |
no data |
| Herbertson 1994 | (1) Diclofenac K 50 mg, n = 52 (2) Diclofenac K 100 mg, n = 52 (3) Aspirin 650 mg, n = 53 (4) Placebo, n = 52 |
TOTPAR 6: (1) 12.1 (2) 12.2 (4) 3.7 |
(1) 29/52 (2) 29/52 (4) 5/52 |
at 8 hours: (1) 28/52 (2) 25/52 (4) 6/52 |
(1) 5.6 (2) 6.1 (4) 1.5 |
at 6 hours: (1) 50 (2) 54 (4) 82 |
| Hersh 2004 | (1) Diclofenac K 25 mg, n = 63 (2) Diclofenac K 50 mg, n = 68 (3) Diclofenac K 100 mg, n = 66 (4) Placebo, n = 68 |
TOTPAR 6: (1) 11.68 (2) 13.86 (3) 16.16 (4) 4.99 |
(1) 43/63 (2) 44/68 (3) 52/66 (4) 11/68 |
no usable data | (1) 5.83 (2) >6 (3) >6 (4) 1.67 |
at 6 hours: (1) 51 (2) 37 (3) 32 (4) 79 |
| Hofele 2006 | (1) Diclofenac K sachet 50 mg, n = 74 (2) Diclofenac K tablet 50 mg, n = 71 (3) Placebo, n = 39 |
TOTPAR 6: (1) 15.5 (2) 14.1 (3) 7.2 |
(1) 55/74 (2) 47/71 (3) 11/39 |
no usable data | Kaplan-Meier estimate Mean: (1) 8.7 (2) 8.9 (3) 4.5 |
at 8 hours: 1) 37 (2) 37 (3) 72 |
| Kubitzek 2003 | (1) Diclofenac K 25 mg, n = 83 (2) Paracetamol 1000 mg, n = 78 (3) Placebo, n = 84 |
TOTPAR 6: values not given | (1) 42/83 (3) 7/84 |
at 6 hours: (1) 25/83 (3) 1/84 |
(1) 3.94 (3) 1.47 |
at 6 hours: (1) 77 (3) 89 |
| Mehlisch 1994 | (1) Diclofenac K 50 mg, n = 53 (2) Diclofenac K 100 mg, n = 52 (3) Aspirin 650 mg, n = 51 (4) Placebo, n = 52 |
TOTPAR 6: (1) 11.6 (2) 14.3 (4) 3.3 |
(1) 28/53 (2) 35/52 (4) 4/52 |
no usable data | (1) 5.9 (2) 7.3 (4) 1.8 |
at 6 hours: (1) 49 (2) 30 (4) 84 |
| Nelson 1994 | (1) Diclofenac K 25 mg, n = 50 (2) Diclofenac K 50 mg, n = 50 (3) Diclofenac K 100 mg, n = 50 (4) Aspirin 650 mg, n = 50 (5) Placebo, n = 50 |
TOTPAR 6: (1) 10.5 (2) 12.2 (3) 14.8 (5) 3.6 |
(1) 23/50 (2) 28/50 (3) 35/50 (5) 4/50 |
no data | (1) 5.3 (2) >8 (3) >8 (5) 2.8 |
at 6 hours: (1) 57 (2) 39 (3) 32 (5) 65 |
| Olson 1997 | (1) Diclofenac K 25 mg, n = 52 (2) Diclofenac K 50 mg, n = 50 (3) Diclofenac K 100 mg, n = 51 (4) Aspirin 650 mg, n = 50 (5) Placebo, n = 52 |
TOTPAR 4: (1) 8.9 (2) 9.5 (3) 10.1 (5) 4.9 |
(1) 32/52 (2) 34/50 (3) 37/51 (5) 15/52 |
no usable data | (1) 5.4 (2) 3.0 (3) 5.4 (5) 2.3 |
at 6 hours: (1) 4 (2) 2 (3) 0 (5) 37 |
| Torres 2004 | (1) Diclofenac SR 75 mg, n = 68 (2) Valdecoxib 20 mg, n = 68 (3) Valdecoxib 40 mg, n = 69 (4) Placebo, n = 67 |
SPID 6 could not be calculated because baseline pain was not reported | no data | no usable | data no usable data | at 12 hours: (1) 39 (4) 52 |
| Zuniga 2004 | (1) Diclofenac K 100 mg, n = 31 (2) Diclofenac Na softgel 100 mg, n = 29 (3) Placebo, n = 15 |
TOTPAR 6: (1) 9.7 (2) 12.2 (3) 0.91 |
(1) 13/31 (2) 16/29 (3) 0/15 |
at 6 hours: (1) 14/31 (2) 21/29 (3) 1/15 |
Mean: (1) 4.5 (2) 5 (3) 1.1 |
at 6 hours: (1) 71 (2) 69 (3) 100 |
Figure 1.

Forest plot of comparison: 1 Diclofenac 25 mg v placebo, outcome: 1.1 Participants with at least 50% pain relief over 4 to 6 hours.
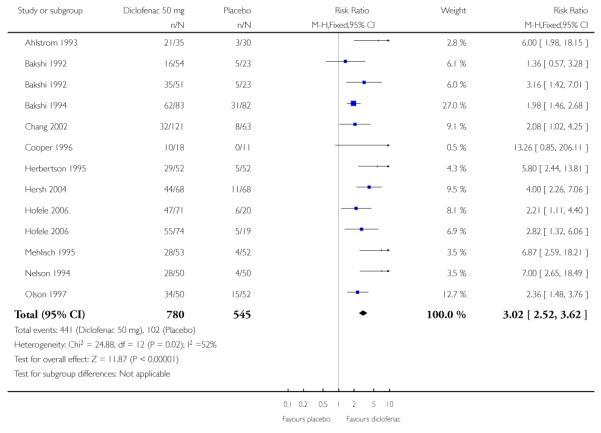
Diclofenac 50 mg versus placebo
Eleven studies (13 treatment arms) with 1325 participants provided data (Ahlstrom 1993; Bakshi 1992; Bakshi 1994; Chang 2002; Cooper 1996; Herbertson 1995; Hersh 2004; Hofele 2006;Mehlisch 1995; Nelson 1994; Olson 1997) (please see Table 1 and Figure 2).
The proportion of participants experiencing at least 50% pain relief over 4 to 6 hours with diclofenac 50 mg was 57% (441/780; range 26% to 75%).
The proportion of participants experiencing at least 50% pain relief with placebo was 19% (102/545; range 5% to 30%).
The relative benefit of treatment compared with placebo was 3.0 (2.5 to 3.6), giving an NNT for at least 50% pain relief over 4 to 6 hours of 2.7 (2.4 to 3.0).
Figure 2.

Forest plot of comparison: 2 Diclofenac 50 mg v placebo, outcome: 2.1 Participants with at least 50% pain relief over 4 to 6 hours.
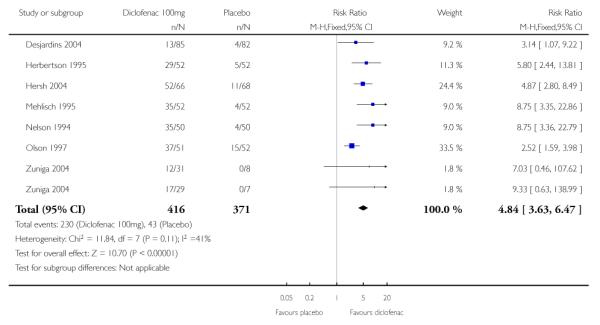
Diclofenac 100 mg versus placebo
Seven studies (eight treatment arms) with 787 participants provided data (Desjardins 2004; Herbertson 1995; Hersh 2004;Mehlisch 1995; Nelson 1994; Olson 1997; Zuniga 2004) (please see Table 1 and Figure 3).
The proportion of participants experiencing at least 50% pain relief over 4 to 6 hours with diclofenac 100 mg was 56% (231/416; range 15% to 79%).
The proportion of participants experiencing at least 50% pain relief with placebo was 12% (44/371; range 5% to 29%).
The relative benefit of treatment compared with placebo was 4.8 (3.6 to 6.4), giving an NNT for at least 50% pain relief over 4 to 6 hours of 2.3 (2.0 to 2.5).
Figure 3.

Forest plot of comparison: 3 Diclofenac 100 mg v placebo, outcome: 3.1 Participants with at least 50% pain relief over 4 to 6 hours.
Summary of results A.
Number of participants with ≥50% pain relief over 4 to 6 hours
| Dose | Studies | Participants | Diclofenac (%) | Placebo (%) | NNT (95%CI) |
|---|---|---|---|---|---|
| 25 mg | 4 | 502 | 53 | 15 | 2.6 (2.2 to 3.3) |
| 50 mg | 11 | 1325 | 57 | 19 | 2.7 (2.4 to 3.0) |
| 100 mg | 7 | 787 | 56 | 12 | 2.3 (2.0 to 2.6) |
Sensitivity analysis of primary outcome (see Summary of results B)
Methodological quality
All studies scored three or more for methodological quality, so no sensitivity analysis was carried out for this criterion.
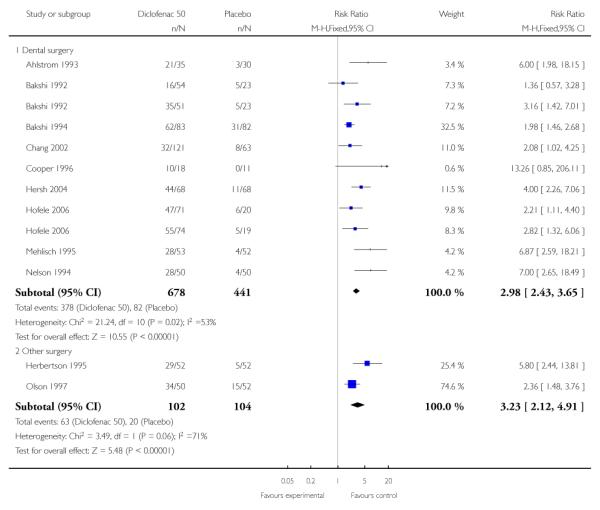
Pain model; dental versus other surgery
Diclofenac 50 mg
(Please see Figure 4)
Figure 4.

Forest plot of comparison: 2 Diclofenac 50 mg v placebo, outcome: 2.4 Participants with at least 50% pain relief over 4 to 6 hours, dental or other surgery.
Nine studies reporting the primary outcome were in dental pain (Ahlstrom 1993; Bakshi 1992; Bakshi 1994; Chang 2002; Cooper 1996; Hersh 2004; Hofele 2006; Mehlisch 1995; Nelson 1994). The proportion of participants with at least 50% pain relief was 56% (378/678) for diclofenac 50 mg, and 19% (82/441) for placebo. The relative benefit was 3.0 (2.4 to 3.7), and the NNT was 2.7 (2.4 to 3.1).
Two studies reporting the primary outcome were in other types of surgery (Herbertson 1995; Olson 1997). The proportion of participants with at least 50% pain relief was 62% (63/102) for diclofenac 50 mg, and 19% (20/104) for placebo. The relative benefit was 3.2 (2.1 to 4.9), and the NNT was 2.4 (1.8 to 3.3). The 95% CI for dental and other surgery overlap, indicating that there was no significant difference for this outcome between dental and other types of surgery in these studies.
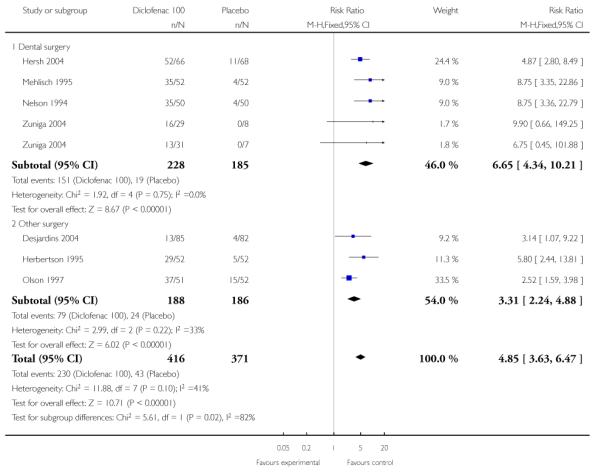
Diclofenac 100 mg
(Please see Figure 5)
Figure 5.

Forest plot of comparison: 3 Diclofenac 100 mg v placebo, outcome: 3.6 Participants with at least 50% pain relief over 4 to 6 hours, dental or other surgery.
Four studies reporting the primary outcome were in dental pain (Hersh 2004; Mehlisch 1995; Nelson 1994; Zuniga 2004). The proportion of participants with at least 50% pain relief was 66% (151/228) for diclofenac 100 mg, and 10% (19/185) for placebo. The relative benefit was 6.6 (4.3 to 10), and the NNT was 1.8 (1.6 to 2.1).
Three studies reporting the primary outcome were in other types of surgery (Desjardins 2004; Herbertson 1995; Olson 1997). The proportion of participants with at least 50% pain relief was 42% (79/188) for diclofenac 100 mg, and 13% (24/186) for placebo. The relative benefit was 3.3 (2.2 to 4.9), and the NNT was 3.4 (2.7 to 4.9).
There was a statistically significant difference for this outcome between dental and other surgery in these studies (z = 4.6, P < 0.0001)
There was insufficient data to analyse the 25 mg dose separately.
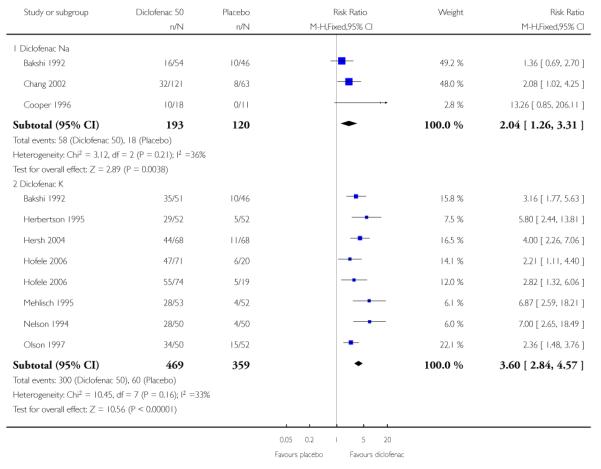
Salt preparation: sodium (Na) versus potassium (K)
Diclofenac 50 mg
(Please see Figure 6)
Figure 6.

Forest plot of comparison: 2 Diclofenac 50 mg v placebo, outcome: 2.11 Participants with at least 50% pain relief over 4 to 6 hours, Na or K salt.
Three studies reporting the primary outcome used diclofenac Na (Bakshi 1992; Chang 2002; Cooper 1996). The proportion of participants with at least 50% pain relief was 30% (58/193) for diclofenac Na 50 mg, and 15% (18/120) for placebo. The relative benefit was 2.0 (1.3 to 3.3), and the NNT was 6.7 (4.2 to 17).
Seven studies reporting the primary outcome used diclofenac K (Bakshi 1992; Herbertson 1995; Hersh 2004; Hofele 2006;Mehlisch 1995; Nelson 1994; Olson 1997). The proportion of participants with at least 50% pain relief was 64% (300/469) for diclofenac K 50 mg, and 17% (60/359) for placebo. The relative benefit was 3.6 (2.8 to 4.6), and the NNT was 2.1 (1.9 to 2.4).
All the studies using diclofenac Na were in dental surgery. For the five studies using diclofenac K 50 mg in dental surgery, the proportion with at least 50% pain relief was 65% (237/367) for diclofenac and 16% (40/255) for placebo. The relative benefit was 3.8 (2.8 to 5.0), and the NNT was 2.1 (1.9 to 2.4). There was a statistically significant difference between the two salt preparations for this outcome (z = 5.90, P < 0.0001).
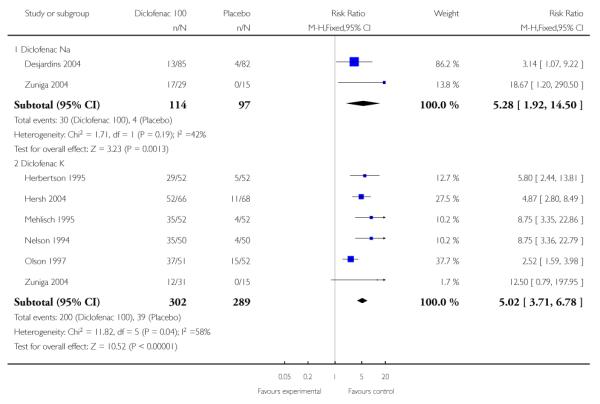
Diclofenac 100 mg
(Please see Figure 7)
Figure 7.

Forest plot of comparison: 3 Diclofenac 100 mg v placebo, outcome: 3.7 Participants with at least 50% pain relief over 4 to 6 hours, Na or K salt.
Two studies reporting the primary outcome used diclofenac Na (Desjardins 2004; Zuniga 2004). The proportion of participants with at least 50% pain relief was 26% (30/114) for diclofenac Na 100 mg, and 4% (4/97) for placebo. The relative benefit was 5.3 (1.9 to 15), and the NNT was 4.5 (3.2 to 7.6).
Six studies reporting the primary outcome used diclofenac K (Herbertson 1995; Hersh 2004; Mehlisch 1995; Nelson 1994;Olson 1997; Zuniga 2004). The proportion of participants with at least 50% pain relief was 66% (200/302) for diclofenac K 100 mg, and 13% (39/289) for placebo. The relative benefit was 5.0 (3.7 to 6.8), and the NNT was 1.9 (1.7 to 2.2).
The 95% CIs for the two salt preparations at 100 mg do not overlap, suggesting a statistically significant difference between them for this outcome, but there were insufficient data for diclofenac Na 100 mg to permit comparison in dental studies only.
There were insufficient data to analyse the 25 mg dose separately.
Formulation: tablet versus dispersible
There were insufficient data for dispersible preparations to carry out this sensitivity analysis.
Study size: 40 or more participants per treatment arm versus fewer than 40
Only three studies, one at each dose (Ahlstrom 1993; Cooper 1996; Zuniga 2004) had fewer than 40 participants in each treatment arm. There were insufficient data to carry out this sensitivity analysis.
Summary of results B.
Sensitivity analyses using number of participants with ≥ 50% pain relief over 4 to 6 hours
| Criterion | Studies | Participants | Diclofenac (%) | Placebo (%) | NNT (95%CI) |
|---|---|---|---|---|---|
| Dental surgery 50 mg | 9 | 1119 | 56 | 19 | 2.7 (2.4 to 3.1) |
| Other surgery 50 mg | 2 | 206 | 62 | 19 | 2.4 (1.8 to 3.3) |
| Dental surgery 100 mg | 4 | 413 | 66 | 10 | 1.8 (1.6 to 2.1) |
| Other surgery 100 mg | 3 | 374 | 42 | 13 | 3.4 (2.7 to 4.9) |
| Na salt 50 mg dental surgery | 3 | 313 | 30 | 15 | 6.7 (4.2 to 17) |
| K salt 50 mg dental surgery | 5 | 622 | 65 | 16 | 2.1 (1.8 to 2.4) |
| Na salt 100 mg | 2 | 211 | 26 | 4 | 4.5 (3.2 to 7.7) |
| K salt 100 mg | 6 | 591 | 66 | 13 | 1.9 (1.7 to 2.2) |
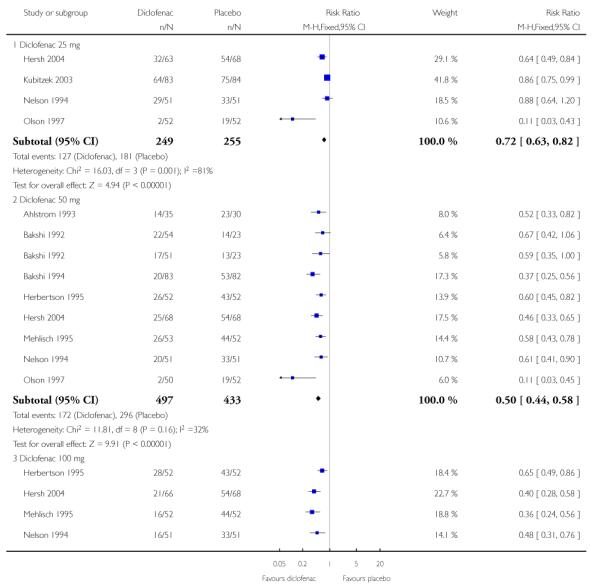
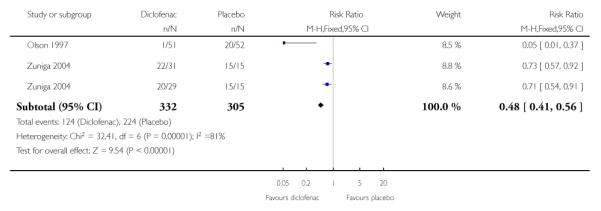
Use of rescue medication
Proportion of participants using rescue medication (see Summary of results C)
All but two studies (Cooper 1996; Desjardins 2004) reported the number or proportion of participants using rescue medication (please see Table 1 and Figure 8).
Four studies using diclofenac 25 mg reported the number or proportion of participants using rescue medication, all at 6 hours (Hersh 2004; Kubitzek 2003; Nelson 1994; Olson 1997). The weighted mean proportion was 51% (127/249) with diclofenac and 71% (181/255) with placebo, giving an NNTp of 5.0 (3.5 to 8.6).
Ten studies (12 treatment arms) using diclofenac 50 mg reported the number or proportion of participants using rescue medication, 8 to 6 hours (Ahlstrom 1993; Bakshi 1992; Bakshi 1994; Herbertson 1995; Hersh 2004; Mehlisch 1995; Nelson 1994; Olson 1997), and 2 to 8 hours (Chang 2002; Hofele 2006). The weighted mean proportion was 40% (305/763) with diclofenac and 70% (372/535) with placebo, giving an NNTp of 3.4 (2.9 to 4.1) for 6 to 8 hours. For 6 hours only the proportion was 35% (172/497) with diclofenac and 68% (296/433) with placebo, giving an NNTp of 3.0 (2.5 to 3.6) for 6 hours.
Six studies (seven treatment arms) using diclofenac 100 mg reported the number or proportion of participants using rescue medication, all at 6 hours (Herbertson 1995; Hersh 2004;Mehlisch 1995; Nelson 1994; Olson 1997; Zuniga 2004). The weighted mean proportion was 37%, and the NNTp was 2.8 (2.3 to 3.5).
Figure 8.

Forest plot of comparison: 4 Diclofenac versus placebo, outcome: 4.2 Participants using rescue medication at 6 hours.
Summary of results C.
Weighted mean proportion using rescue medication
| Dose and time of assessment | Studies | Participants | Diclofenac (%) | Placebo (%) | NNTp (95%CI) |
|---|---|---|---|---|---|
| 25 mg, 6 hours only | 4 | 504 | 51 | 71 | 5.0 (3.5 to 8.6) |
| 50 mg, 6 and 8 hours | 9 | 1298 | 40 | 70 | 3.4 (2.9 to 4.1) |
| 50 mg, 6 hours only | 5 | 930 | 35 | 68 | 3.0 (2.5 to 3.6) |
| 100 mg, 6 hours only | 6 | 637 | 37 | 73 | 2.8 (2.3 to 3.5) |
Time to use of rescue medication (see Summary of results D)
Eight studies reported the median time, and three the mean time to use of rescue medication (please see Table 1).
In four studies (502 participants) (Hersh 2004; Kubitzek 2003; Nelson 1994; Olson 1997) the weighted mean of the median time to use of rescue medication was 3.8 hours for diclofenac 25 mg and 1.5 hours for placebo.
In five studies (457 participants) (Chang 2002; Hersh 2004; Mehlisch 1995; Nelson 1994; Olson 1997) the weighted mean of the median time to use of rescue medication was 4.3 hours for diclofenac 50 mg and 2.0 hours for placebo.
In six studies (683 participants) (Desjardins 2004; Hersh 2004; Mehlisch 1995; Nelson 1994; Olson 1997; Zuniga 2004) the weighted mean of the median time to use of rescue medication was 4.9 hours for diclofenac 100 mg and 1.9 hours for placebo.
In three studies (378 participants) (Bakshi 1994; Cooper 1996; Hofele 2006) the weighted mean of the mean time to use of rescue medication was 7.4 hours for diclofenac 50 mg and 3.6 hours for placebo.
Summary of results D.
Weighted median and mean time to use of rescue medication
| Median time (hrs) | ||||
|---|---|---|---|---|
| Dose | Studies | Participants | Diclofenac | Placebo |
| 25 mg | 4 | 502 | 3.8 | 1.5 |
| 50 mg | 5 | 457 | 4.3 | 2.0 |
| 100 mg | 6 | 683 | 4.9 | 1.9 |
| Mean time (hrs) | ||||
| 50 mg | 3 | 378 | 7.4 | 3.6 |
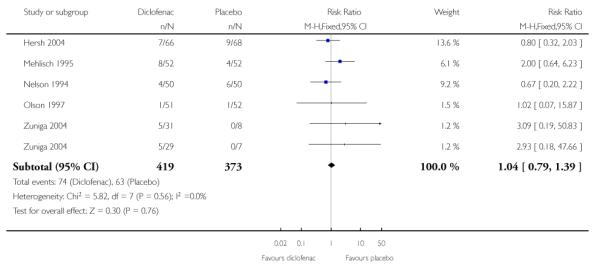
Adverse events (see Summary of results E)
(Please see Table 2 and Figure 9)
Table 2.
Summary of outcomes: adverse events and withdrawals
| Adverse events | Withdrawals | ||||
|---|---|---|---|---|---|
| Study ID | Treatment | Any | Serious | Adverse event | Other |
| Ahlstrom 1993 | (1)Diclofenac (soluble) 50 mg, n = 35 (2) Ibuprofen (tablets) 400 mg, n = 32 (3) Placebo, n = 30 |
(1) 6/35 (3) 2/30 considered treatment-related in 1 diclofenac and 1 ibuprofen patient |
None reported | None | 30 exclusions: various protocol violations |
| Bakshi 1992 | (1) Diclofenac K 50 mg, n = 51 (2) Diclofenac Na (enteric coated) 50 mg, n = 54 (3) Placebo, n = 46 |
Possibly or probably treatment-related (1) 3/51 (2) 1/54 (3) 3/46 |
None | None | 29 exclusions: 26 did not need medication, 3 lost to followup |
| Bakshi 1994 | (1)Diclofenac (soluble) 50 mg, n = 83 (2) Ibuprofen 400 mg, n = 80 (3) Placebo, n = 82 |
(1) 4/83 (3) 5/82 |
None reported | None | 12 exclusions: various protocol violations |
| Chang 2002 | (1) Diclofenac Na (enteric coated) 50 mg, n = 121 (2) Rofecoxib 50 mg, n = 121 (3) Placebo, n = 63 |
No single dose data | No single dose data | at 36 hours: (3) 1/63 (asthma flare) |
None |
| Cooper 1996 | (1) Diclofenac Na 50 mg, n = 18 (2) Misoprostol 200 μg, n = 21 (3) Diclofenac Na + misoprostol 50 mg/200 μg, n = 20 (4) Placebo, n = 11 |
No usable data. All AEs were transient and mild, and considered normal sequale of surgical procedure and probably unrelated to study drug | None | ||
| Desjardins 2004 | (1) Diclofenac Na 100 mg, n = 85 (2) Rofecoxib 50 mg, n = 85 (3) Placebo, n = 82 |
at 24 hours: (1) 38/85 (3) 41/82 |
None | (1) 1/85 (3) 3/82 |
None reported |
| Herbertson 1994 | (1) Diclofenac K 50 mg, n = 52 (2) Diclofenac K 100 mg, n = 52 (3) Aspirin 650 mg, n = 53 (4) Placebo, n = 52 |
(1) 6/54 (2) 6/55 (4) 2/54 |
None | 8 in total | In total, 8 participants did not contribute to any efficacy analysis, 23 did not contribute to reported TOTPAR 8 |
| Hersh 2004 | (1) Diclofenac K 25 mg, n = 63 (2) Diclofenac K 50 mg, n = 68 (3) Diclofenac K 100 mg, n = 66 (4) Placebo, n = 68 |
(1) 8/63 (2) 8/68 (3) 7/66 (4) 9/68 |
None reported | None | 1 placebo participant unwilling to continue |
| Hofele 2006 | (1) Diclofenac K sachet 50 mg, n = 74 (2) Diclofenac K tablet 50 mg, n = 71 (3) Placebo, n = 39 |
at 8 hours: (1) 2/74 (2) 2/71 (3) 2/39 |
None | None | 5 exclusions for protocol violations: 2 diclofenac sachet, 1 diclofenac tablet, 1 placebo |
| Kubitzek 2003 | (1) Diclofenac K 25 mg, n = 83 (2) Paracetamol 1000 mg, n = 78 (3) Placebo, n = 84 |
at 48 hrs: (1) 6/83 (3) 2/84 |
None | None | 1 placebo participant excluded for protocol violation |
| Mehlisch 1994 | 1) Diclofenac K 50 mg, n = 53 (2) Diclofenac K 100 mg, n = 52 (3) Aspirin 650 mg, n = 51 (4) Placebo, n = 52 |
at 7 days: (1) 5/53 (2) 8/52 (4) 4/52 |
None | None | None reported |
| Nelson 1994 | (1) Diclofenac K 25 mg, n = 50 (2) Diclofenac K 50 mg, n = 50 (3) Diclofenac K 100 mg, n = 50 (4) Aspirin 650 mg, n = 50 (5) Placebo, n = 50 |
at 8 hours: (1) 5/51 (2) 4/51 (3) 4/51 (5) 6/51 |
None reported | None | 1 participant excluded from safety analysis, 3 excluded from any efficacy analysis, 7 excluded from 8 hour efficacy analysis |
| Olson 1997 | (1) Diclofenac K 25 mg, n = 52 (2) Diclofenac K 50 mg, n = 50 (3) Diclofenac K 100 mg, n = 51 (4) Aspirin 650 mg, n = 50 (5) Placebo, n = 52 |
at 8 hours: (1) 1/52 (2) 0/50 (3) 1/51 (5) 1/52 |
None | None | None |
| Torres 2004 | (1)Diclofenac SR75 mg, n = 68 (2) Valdecoxib 20 mg, n = 68 (3) Valdecoxib 40 mg, n = 69 (4) Placebo, n = 67 |
at 12 hours: (1) 14/65 (4) 17/67 |
None reported | No usable data | No usable data |
| Zuniga 2004 | (1) Diclofenac K 100 mg, n = 31 (2) Diclofenac Na softgel 100 mg, n = 29 (3) Placebo, n = 15 |
at 24 hours: (1) 5/31 (2) 5/29 (3) 1/15 most occurred after rescue medication |
None | None | 1 participant excluded due to protocol violation |
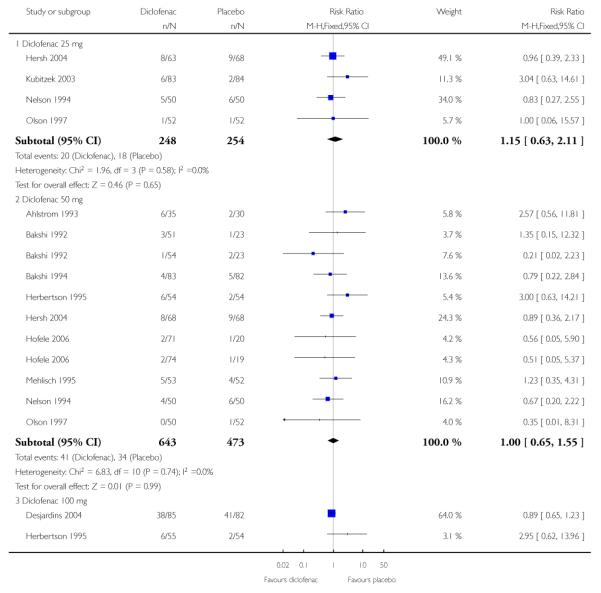
Figure 9.

Forest plot of comparison: 4 Diclofenac versus placebo, outcome: 4.1 Participants with at least one adverse event.
Any adverse event
Four studies using diclofenac 25 mg reported on the number of participants with at least one adverse event (Hersh 2004; Kubitzek 2003; Nelson 1994; Olson 1997): 8% (20/248) with diclofenac, and 7% (18/254) with placebo.
Nine studies using diclofenac 50 mg reported on the number of participants with at least one adverse event (Ahlstrom 1993; Bakshi 1992; Bakshi 1994; Herbertson 1995; Hersh 2004;Hofele 2006; Mehlisch 1995; Nelson 1994; Olson 1997): 6% (41/643) with diclofenac, and 7% (34/473) with placebo.
Seven studies using diclofenac 100 mg reported on the number of participants with at least one adverse event (Desjardins 2004; Herbertson 1995; Hersh 2004; Mehlisch 1995; Nelson 1994; Olson 1997; Zuniga 2004): 18% (18/419) with diclofenac, and 17% (64/373) with placebo.
At no dose was there any difference in the proportion of participants with diclofenac or placebo experiencing any adverse event.
Summary of results E.
Participants with at least one adverse event
| Dose | Studies | Participants | Naproxen (%) | Placebo (%) | NNH (95%CI) |
|---|---|---|---|---|---|
| 25 mg | 4 | 502 | 8 | 7 | not calculated |
| 50 mg | 9 | 1011 | 6 | 7 | not calculated |
| 100 mg | 7 | 792 | 18 | 17 | not calculated |
Serious adverse event
No study reported any serious adverse events with single dose treatment. One study (Chang 2002) reported a serious event (asthma flare) in a participant given placebo, but it is not clear whether this occurred during the single or multiple dose phase.
Withdrawals
(Please see Table 2)
Participants who took rescue medication were classified as withdrawals due to lack of efficacy, and details are reported under “Use of rescue medication” above.
Withdrawals and exclusions were not reported consistently, particularly in older studies. Exclusions may not be of any particular consequence in single dose acute pain studies, where most exclusions result from patients not having moderate or severe pain (McQuay 1982). Withdrawals were sometimes reported without stating which treatment groups these referred to, or when withdrawals occurred, i.e., before assessment of analgesia at 4 to 6 hours, or at some other point before the end of the trial. Where details were given, withdrawals or exclusions were usually due to protocol violations or adverse events related to the surgical procedure.
Three studies reported withdrawals due to adverse events. Chang et al (Chang 2002) reported withdrawal of one placebo-treated participant due to an asthma flare (see serious adverse events).Desjardins 2004 reported withdrawal of one participant treated with diclofenac 100 mg, and three with placebo, but did not provide specific details. Herbertson 1995 reported withdrawal of eight participants in total, one of whom was treated with diclofenac 100 mg, and experienced nausea and vomiting.
DISCUSSION
This updated review includes eight additional studies and more than doubles the amount of information available for each dose of diclofenac. All the studies were of adequate methodological quality to minimise bias. The additional information did not significantly change the NNTs for at least 50% pain relief over 4 to 6 hours at any dose, but should make the estimates more robust.
In the updated review, with all doses of diclofenac and both salts together, 50 to 60% of participants achieved at least 50% pain relief over 4 to 6 hours, compared to 10 to 20% with placebo, giving NNTs of about 2.5; there was no dose response for this outcome. For every five participants with moderate to severe postoperative pain treated with a single dose of diclofenac, two would experience at least 50% pain relief who would not have done so with placebo.
Indirect comparisons of NNTs for at least 50% pain relief over 4 to 6 hours in reviews of other analgesics using identical methods indicate that diclofenac 50 mg has equivalent efficacy to naproxen 500/550 mg (2.7 (2.3 to 3.2)) (Derry 2009) and lumiracoxib (2.7 (2.2 to 3.5)) (Roy 2007), and is better than paracetamol 1000 mg (3.6 (3.2 to 4.1)) (Toms 2008), but is worse than rofecoxib (2.2 (1.9 to 2.4) (Barden 2004b). A current listing of reviews of analgesics in the single dose postoperative pain model can be found at www.medicine.ox.ac.uk/bandolier/index.html.
Analysis of the primary outcome according to type of surgery demonstrated a statistically significant difference between dental surgery and other types of surgery for the 100 mg, but not the 50 mg dose. There may be a clinically significant difference between them, but the result could also be due to chance since the number of events in each set of studies was fewer than 220 (151 and 79 in the diclofenac arms of the dental and the other surgery studies respectively). Additionally, the “other surgery” group was clinically heterogeneous, with participants undergoing bunionectomy and various gynaecological procedures. Bunionectomy is a relatively new acute postoperative pain model and has rarely been included in single dose analgesic studies. Bunionectomy studies have not been included in comparisons of outcomes of different acute postoperative pain models (Barden 2004a), and it is not known whether bunionectomy studies produce similar results to other postoperative pain models. In the single bunionectomy study included here (Desjardins 2004), diclofenac (100 mg) had the lowest event rate of all included studies, at 15%, tentatively indicating that bunionectomy may be quantitatively different from other pain models.
Analysis of the primary outcome according to the diclofenac salt preparation used showed statistically significant differences between the sodium and potassium salts for both 50 and 100 mg. There was sufficient data for 50 mg to carry out the sensitivity analysis in dental studies only, and the statistical difference remained highly significant (P < 0.0001). This difference may be clinically important. In these studies the potassium salt performed better than the sodium salt, and the majority of studies in this review used the potassium salt. This is interesting because the sodium salt is the one normally dispensed, at least in England, where only 100,000 prescriptions out of almost eight million in 2007 were for the potassium salt. The bulk of the trial data is for the potassium salt, but the bulk of prescribing is for the sodium salt, which has measurably less effect. This is an important point for those producing guidelines and policy, especially as these effects in acute pain may have implications for chronic conditions.
There were insufficient data to investigate the effects on the primary outcome of tablet versus dispersible, or slow release versus immediate release formulations.
It has been suggested that data on use of rescue medication, whether as a proportion of participants requiring it, or the median time to use of it, might be helpful in assessing the usefulness of an analgesic, and possibly distinguishing between different doses (Moore 2005). This review demonstrated a non-significant trend for fewer participants to need rescue medication within 6 hours with higher doses of diclofenac, with just over 10% fewer using rescue medication with 100 mg than with 25 mg. Additionally, the median time to use of rescue medication increased with higher doses, from 4 hours with 25 mg to 5 hours with 100 mg. Both of these results indicate that the higher doses give more prolonged pain relief than lower doses. Longer duration of action may be advantageous in some circumstances. In a postoperative setting, where patients may feel nauseated, a longer time before remedication is needed and could be of benefit to the patient, and it may also reduce demands on time for nursing staff. Duration of action may also be a useful outcome with which to compare different analgesics. The full implications of the importance of remedication as an outcome awaits completion of other reviews, allowing examination of a substantial body of evidence.
Reporting of data for adverse events, withdrawals (other than lack of efficacy) or exclusions, and handling of missing data was not always complete, although it did appear to be better in the more recent studies. Adverse events were collected using various methods (questioning, patient diary) over different periods of time. This may have included periods after the use of rescue medication, which may cause its own adverse events. Poor reporting of adverse events in acute pain trials have been noted before (Edwards 1999). The usefulness of single dose studies for assessing adverse events is questionable, but it is non-the-less reassuring that there was no difference between naproxen (at any dose) and placebo for occurrence of any adverse event, and that serious adverse events and adverse event withdrawals were rare, and generally not thought to be related to the test drug. Long-term, multiple dose studies should be used for meaningful analysis of adverse events since, even in acute pain settings, analgesics are likely to be used in multiple doses.
Lack of information about withdrawals or exclusions may have led to an overestimate of efficacy, but the effect is probably not significant because it is as likely to be related to poor reporting as poor methods. In single dose studies most exclusions occur for protocol violations such as failing to meet baseline pain requirements, or failing to return for post treatment visits after the acute pain results are concluded. Where patients are treated with a single dose of medication and observed, often “on site” for the duration of the trial, it might be considered unnecessary to report on “withdrawals” if there were none. For missing data it has been shown that over the 4 to 6 hour period, there is no difference between baseline observation carried forward, which gives the more conservative estimate, and last observation carried forward (Moore 2005).
AUTHORS’ CONCLUSIONS
Implications for practice
A single dose of diclofenac 100 mg is an effective analgesic, providing at least 50% pain relief to about half of the treated patients with acute, moderate to severe, postoperative pain. The NNT of 2.3 for at least 50% pain relief compares favourably with other analgesics commonly used for postoperative pain. In single dose, it is associated with a low rate of adverse events, similar to that with placebo. Lower doses may provide equivalent levels of analgesia, with a slightly shorter duration of action. Since the last version of this review, additional evidence has strengthened differences between sodium and potassium salt preparations; it may be that potassium salts are more appropriate for acute pain conditions, and sodium salts for chronic pain conditions. However, care should be exercised over the choice of potassium salt or sodium salt formulations, and a wider examination of evidence of different sorts will be needed in making appropriate choices.
Implications for research
The most important implication for research is to clarify the apparent difference in efficacy between the potassium and sodium salts of diclofenac. Further studies at lower doses with the more effective potassium salt could clarify whether useful analgesia could be achieved with less diclofenac, probably improving safety. It should always be the goal to use the lowest dose of a drug that provides the desired clinical effect, and lower doses are likely to be associated with fewer adverse events in clinical practice. Additional studies investigating the relative efficacy of the sodium and potassium salts are needed to determine whether the difference demonstrated in this review is true. The major implication is for better reporting of clinical trials, in avoiding average information from highly skewed distributions, in providing information about how many patients achieve a clinically useful level of pain relief, and in reporting other outcomes of clinical relevance, such as time to remedication.
PLAIN LANGUAGE SUMMARY.
Single dose oral diclofenac for pain relief in adults experiencing moderate or severe pain following a surgical procedure
Diclofenac is a non-steroidal anti-inflammatory drug (NSAID) with pain relieving properties. It is used to treat many painful conditions, including acute postoperative pain. This review shows that single dose oral diclofenac provides effective pain relief for adults experiencing moderate or severe pain following a surgical procedure. For every five participants with moderate to severe postoperative pain treated with a single dose of diclofenac, two would experience at least 50% pain relief who would not have done so with placebo. One form of diclofenac, the potassium salt, is more effective at the same dose than the other form of diclofenac, the sodium salt. The incidence of adverse effects did not differ significantly from placebo in these single dose studies.
ACKNOWLEDGEMENTS
Jodie Barden and Jayne Rees were authors on the earlier review.
SOURCES OF SUPPORT
Internal sources
Pain Research funds, UK.
External sources
NHS Cochrane Collaboration Programme Grant Scheme, UK.
NIHR Biomedical Research Centre Programme, UK.
Support for RAM
CHARACTERISTICS OF STUDIES
Characteristics of included studies [ordered by study ID]
| Methods | RCT, DB, double dummy, single oral dose, 3 parallel groups Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 20, 40, 60 mins then hourly up to 6 hours |
| Participants | Third molar extraction N = 97 M = 46, F = 51 Mean age 25 yrs |
| Interventions | Diclofenac (soluble) 50 mg, n = 35 Ibuprofen (tablets) 400 mg, n = 32 Placebo, n = 30 |
| Outcomes | PI: std 100 mm VAS PR: std 100 mm VAS PGE: std 5 point scale |
| Notes | Oxford Quality Score: R1, DB2, W1 No details about rescue medication used or any restrictions on time before use was permitted |
| Methods | RCT, DB, single dose, 3 parallel groups Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 15, 30 and 60 mins then hourly up to 6 hours |
| Participants | Third molar extraction N = 151 M = 70, F = 81 Mean age 26 yrs |
| Interventions | Diclofenac K 50 mg, n = 51 Diclofenac Na (enteric coated) 50 mg, n = 54 Placebo, n = 46 |
| Outcomes | PI: std 4 point scale PR: 4 point scale (non std) PGE: 4 point scale (non std) |
| Notes | Oxford Quality Score: R1, DB1, W1 Rescue medication permitted after 1 hour. No details about drug used |
| Methods | RCT, DB, double dummy, single oral dose, 3 parallel groups Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 20, 40, 60, 90, 120 and 150 mins then hourly up to 6 hours |
| Participants | Third molar extraction N = 257 M = 151, F = 94 Mean age 27 yrs |
| Interventions | Diclofenac (soluble) 50 mg, n = 83 Ibuprofen 400 mg, n = 80 Placebo, n = 82 |
| Outcomes | PI: std 100 mm VAS PR: std 5 point scale PGE: 4 point (non std) |
| Notes | Oxford Quality Score: R1 DB2, W1 Rescue medication permitted after 1 hour. No details of drug used |
| Methods | RCT, DB, double dummy, 3 parallel groups, single and multiple oral dose phases Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 30, 60, 90, 120 mins, then hourly to 12 hours, then at 16, 20, 24 hours |
| Participants | Third molar extraction N = 305 M = 143, F = 162 Mean age 23 yrs |
| Interventions | Diclofenac Na (enteric coated) 50 mg, n = 121 Rofecoxib 50 mg, n = 121 Placebo, n = 63 |
| Outcomes | PR: std 5 point scale PGE: std 5 point scale Numbers of participants using rescue medication Time to use of rescue medication Numbers with any adverse event Withdrawals |
| Notes | Oxford Quality Score: R2, DB2, W1 Rescue medication permitted at any time (hydrocodone/paracetamol 5/500 mg) |
| Methods | RCT, DB, 4 parallel groups, single oral dose Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 15, 30, 60 mins, than hourly to 6 hours. |
| Participants | Third molar extraction N = 70 M = 27, F = 43 Mean age 24 yrs |
| Interventions | Diclofenac Na 50 mg, n = 18 Misoprostol 200 μg, n = 21 Diclofenac Na + misoprostol 50 mg/200 μg, n = 20 Placebo, n = 11 |
| Outcomes | PI: std 4 point scale PR: std 5 point scale Time to use of rescue medication Numbers with serious adverse events |
| Notes | Oxford Quality Score: R1, DB2, W0 Rescue medication permitted after 2 hours. No details of drug used |
| Methods | RCT, DB, 3 parallel groups, single and multiple oral dose phases Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 15, 30, 45, 60, 90, 120 mins, then hourly to 6 hours, and at 8, 10, 12, 14 and 24 hours |
| Participants | First metatarsal bunionectomy N = 252 M = 34, F = 218 Mean age 41 yrs |
| Interventions | Diclofenac Na 100 mg, n = 85 Rofecoxib 50 mg, n = 85 Placebo, n = 82 |
| Outcomes | PI: std 4 point scale and VAS PR: std 5 point scale PGE: std 5 point scale Numbers using rescue medication Time to use of rescue medication Numbers with any adverse event and serious adverse events Withdrawals |
| Notes | Oxford Quality Score: R2, DB2, W1 Rescue medication permitted after 90 mins (hydrocodone/paracetamol 7.5/500 mg) |
| Methods | RCT, DB, 4 parallel groups, single oral dose Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 30 and 60 mins, then hourly to 8 hours. |
| Participants | Gynaecological surgery N = 217 All F Mean age = 43 yrs |
| Interventions | Diclofenac K 50 mg, n = 52 Diclofenac K 100 mg, n = 52 Aspirin 650 mg, n = 53 Placebo, n =52 |
| Outcomes | PI: std 4 point scale PR: std 5 point scale PGE: std 5 point scale |
| Notes | Oxford Quality Score: R1, DB1, W1 Rescue medication permitted after 1 hour, but 2 hours recommended. No details of drug used |
| Methods | RCT, DB, double dummy, 4 parallel groups, single oral dose Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 15, 30, 45, 60, 90, 120 mins, then hourly to 6 hours |
| Participants | Third molar extraction N = 265 M = 111, F = 154 Mean age 21 yrs |
| Interventions | Diclofenac K 25 mg, n = 63 Diclofenac K 50 mg, n = 68 Diclofenac K 100 mg, n = 66 Placebo, n = 68 |
| Outcomes | PI: std 4 point scale PR: std 5 point scale PGE: std 5 point scale Numbers using rescue medication Time to use of rescue medication Numbers with any adverse event Withdrawals |
| Notes | Oxford Quality Score: R2, DB2, W1 Rescue medication permitted after 1 hour (hydrocodone/paracetamol 5/500 mg or oxycodone/paracetamol 5/325 mg) |
| Methods | RCT, DB, double dummy, 3 parallel groups, single oral dose Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 15, 30, 45, 60, 90, 120 mins, then hourly to 6 hours, and at 8 and 24 hours |
| Participants | Third molar extraction N = 184 M = 85, F = 99 Mean age = 27 yrs |
| Interventions | Diclofenac K sachet 50 mg, n = 74 Diclofenac K tablet 50 mg, n = 71 Placebo, n = 39 |
| Outcomes | PI: std 4 point scale PR: std 5 point scale PGE: std 5 point scale Numbers using rescue medication Time to use of rescue medication Numbers with any adverse event Withdrawals |
| Notes | Oxford Quality Score: R2, DB2, W1 Rescue medication permitted after 2 hours (paracetamol 1000 mg) |
| Methods | RCT, DB, 3 parallel groups, single oral dose Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 30, 60 mins, then hourly to 6 hours |
| Participants | Third molar extraction N = 245 M = ~40%, F = ~60% Age not given |
| Interventions | Diclofenac K 25 mg, n = 83 Paracetamol 1000 mg, n = 78 Placebo, n = 84 |
| Outcomes | PI: std 4 point scale PR: std 5 point scale PGE: std 5 point scale Numbers using rescue medication Time to use of rescue medication Numbers with any adverse event and serious adverse events Withdrawals |
| Notes | Oxford Quality Score: R1, DB2, W1 Rescue medication permitted after 1 hour (ibuprofen 200 mg) |
| Methods | RCT, DB, double dummy, 4 parallel groups, single oral dose Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 30, 60 mins then hourly to 8 hours. |
| Participants | Third molar extraction N = 208 M = 91, F = 117 Mean age = 26 yrs |
| Interventions | Diclofenac K 50 mg, n = 53 Diclofenac K 100 mg, n = 52 Aspirin 650 mg, n = 51 Placebo, n = 52 |
| Outcomes | PI: std 4 point scale PR: std 5 point scale PGE: std 5 point scale Numbers using rescue medication Time to use of rescue medication Numbers with any adverse event and serious adverse events Withdrawals |
| Notes | Oxford Quality Score: R1, DB2, W1 Rescue medication permitted after 2 hours. No details of drug used |
| Methods | RCT, DB, 5 parallel groups, single oral dose Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 15, 30, 45, 60, 90, 120 mins, then hourly to 6 hours |
| Participants | Third Molar Extraction N = 183 M = 126, F = 129 Mean age 25 yrs |
| Interventions | Diclofenac K 25 mg, n = 50 Diclofenac K 50 mg, n = 50 Diclofenac K 100 mg, n = 50 Aspirin 650 mg, n = 50 Placebo, n = 50 |
| Outcomes | PI: std 4 point scale PR: std 5 point scale PGE: std 5 point scale Numbers using rescue medication Time to use of rescue medication Numbers with any adverse event Withdrawals due to adverse events |
| Notes | Oxford Quality Score: R1, DB2, W1 Rescue medication permitted after 1 hour. No details of drug used |
| Methods | RCT, DB, 5 parallel groups, single oral dose. Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 30, 60 mins, then hourly to 8 hours. |
| Participants | Post-episiotomy N = 255 All F Mean age 24 yrs |
| Interventions | Diclofenac K 25 mg, n = 52 Diclofenac K 50 mg, n = 50 Diclofenac K 100 mg, n = 51 Aspirin 650 mg, n = 50 Placebo, n = 52 |
| Outcomes | PI: std 4 point scale PR: std 5 point scale PGE: non std 4 point scale Numbers using rescue medication Time to use of rescue medication Numbers with any adverse event and serious adverse events Withdrawals |
| Notes | Oxford Quality Score: R1, DB2, W1 Rescue medication permitted after 1 hour (non-study analgesic) |
| Methods | RCT, DB, 4 parallel groups, single and multiple dose phases Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 30, 45, 60 mins, then hourly to 6 hours, then at 10, 12, 18, 24, 36 hours |
| Participants | Inguinal hernia surgery N = 269 All M Mean age 53 yrs |
| Interventions | Diclofenac SR 75 mg, n = 68 Valdecoxib 20 mg, n = 68 Valdecoxib 40 mg, n = 69 Placebo, n = 67 |
| Outcomes | PI: std 4 point scale and VAS PGE: non std 4 point scale Numbers using rescue medication Time to use of rescue medication Numbers with any adverse event Withdrawals |
| Notes | Oxford Quality Score: R1, DB1, W1 Rescue medication permitted at any time (usual analgesic for hospital) |
| Methods | R, DB, 3 parallel groups, single oral dose Medication administered when baseline pain was of moderate to severe intensity Pain assessed at 0, 15, 30, 45, 60, 90, 120 mins, then hourly to 6 hours, then at 8 and 24 hours |
| Participants | Third molar extraction N = 75 M = 25, F = 50 Mea age 23 yrs |
| Interventions | Diclofenac K 100 mg, n = 31 Diclofenac Na softgel 100 mg, n = 29 Placebo, n = 15 |
| Outcomes | PI: std 4 point scale PR: std 5 point scale PGE: std 5 point scale Numbers using rescue medication Time to use of rescue medication Numbers with any adverse event and serious adverse events Withdrawals |
| Notes | Oxford Quality Score: R2, DB2, W1 Rescue medication permitted at any time. No details of drug used |
DB - double blind; F - female; M - male; N - total number in trial; n - number in treatment arm; PI - pain intensity; PR - pain relief; PGE - patient global evaluation; std - standard; R - randomised; W - withdrawals
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ahlstrom 1989 | No placebo control |
| Apaydin 1994 | No placebo control |
| Aranda 1989 | No placebo control |
| Carlos 1984 | Could not be obtained despite attempts to contact authors, ordering through British library and help from librarians at Novartis and Knoll pharmaceuticals |
| Dorfmann 1991 | Inadequate description of method. Did not say whether the allocation was randomised, did not say when interventions were administered, no mention of the level of baseline pain and did not define the pain measurement used |
| El-Tanany 1993 | No placebo control |
| Fineschi 1997 | No placebo control |
| Frezza 1985 | Unobtainable |
| Garcia 1997 | Intravenous route |
| Graf 2000 | Not obtainable |
| Henderson 1994 | No placebo control |
| Henrikson 1982 | Only presented data for the placebo arm for the first hour |
| Hultin 1978 | Cross-over study with the first dose administered exactly one hour after LA rather than when patients experienced moderate to severe pain |
| Iqbal 1986 | Unobtainable |
| Iwabuchi 1980 | No placebo control |
| Joubert 1977 | Unobtainable |
| Kittala 1972 | Routine intervention administration irrespective of baseline pain intensity |
| Li 1998 | No placebo control |
| Matthews 1984 | Intervention administered irrespective of baseline pain intensity |
| Mayer 1980 | Multiple dose study with no mention of baseline pain |
| Nakanishi 1990 | No placebo control |
| Rautela 1998 | Intramuscular route |
| Shimura 1981 | No placebo control |
| Tam 2001 | Intervention administered before procedure |
| Tani 1974 | No placebo control |
| Tesseroli 1986 | At baseline, the mean VAS minus 1.96 × SD was less than 30 mm, therefore some patients may have been included with a baseline pain of less than moderate intensity |
| Ujpal 1999 | No placebo control |
| Vigneron 1977 | Unobtainable |
| Walton 1993 | First dose administered IM during surgery, oral doses then given postoperatively at specified time points irrespective of baseline pain |
| Wuolijoki 1987 | Intervention administered pre-operatively or immediately post-operatively irrespective of baseline pain intensity |
| Zhang 2000 | Could not be obtained |
DATA AND ANALYSES
Comparison 1.
Diclofenac 25 mg v placebo
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Participants with at least 50% pain relief over 4 to 6 hours | 4 | 502 | Risk Ratio (M-H, Fixed, 95% CI) | 3.63 [2.64, 4.98] |
Comparison 2.
Diclofenac 50 mg v placebo
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Participants with at least 50% pain relief over 4 to 6 hours | 11 | 1325 | Risk Ratio (M-H, Fixed, 95% CI) | 3.02 [2.52, 3.62] |
| 2 Participants with at least 50% pain relief over 4 to 6 hours, dental or other surgery | 11 | Risk Ratio (M-H, Fixed, 95% CI) | Subtotals only | |
| 2.1 Dental surgery | 9 | 1119 | Risk Ratio (M-H, Fixed, 95% CI) | 2.98 [2.43, 3.65] |
| 2.2 Other surgery | 2 | 206 | Risk Ratio (M-H, Fixed, 95% CI) | 3.23 [2.12, 4.91] |
| 3 Participants with at least 50% pain relief over 4 to 6 hours, Na or K salt | 9 | Risk Ratio (M-H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Diclofenac Na | 3 | 313 | Risk Ratio (M-H, Fixed, 95% CI) | 2.04 [1.26, 3.31] |
| 3.2 Diclofenac K | 7 | 828 | Risk Ratio (M-H, Fixed, 95% CI) | 3.60 [2.84, 4.57] |
Comparison 3.
Diclofenac 100 mg v placebo
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Participants with at least 50% pain relief over 4 to 6 hours | 7 | 787 | Risk Ratio (M-H, Fixed, 95% CI) | 4.84 [3.63, 6.47] |
| 2 Participants with at least 50% pain relief over 4 to 6 hours, dental or other surgery | 7 | 787 | Risk Ratio (M-H, Fixed, 95% CI) | 4.85 [3.63, 6.47] |
| 2.1 Dental surgery | 4 | 413 | Risk Ratio (M-H, Fixed, 95% CI) | 6.65 [4.34, 10.21] |
| 2.2 Other surgery | 3 | 374 | Risk Ratio (M-H, Fixed, 95% CI) | 3.31 [2.24, 4.88] |
| 3 Participants with at least 50% pain relief over 4 to 6 hours, Na or K salt | 7 | Risk Ratio (M-H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Diclofenac Na | 2 | 211 | Risk Ratio (M-H, Fixed, 95% CI) | 5.28 [1.92, 14.50] |
| 3.2 Diclofenac K | 6 | 591 | Risk Ratio (M-H, Fixed, 95% CI) | 5.02 [3.71, 6.78] |
Comparison 4.
Diclofenac versus placebo
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Participants with at least one adverse event | 12 | Risk Ratio (M-H, Fixed, 95% CI) | Subtotals only | |
| 1.1 Diclofenac 25 mg | 4 | 502 | Risk Ratio (M-H, Fixed, 95% CI) | 1.15 [0.63, 2.11] |
| 1.2 Diclofenac 50 mg | 9 | 1116 | Risk Ratio (M-H, Fixed, 95% CI) | 1.00 [0.65, 1.55] |
| 1.3 Diclofenac 100 mg | 7 | 792 | Risk Ratio (M-H, Fixed, 95% CI) | 1.04 [0.79, 1.39] |
| 2 Participants using rescue medication at 6 hours | 10 | Risk Ratio (M-H, Fixed, 95% CI) | Subtotals only | |
| 2.1 Diclofenac 25 mg | 4 | 504 | Risk Ratio (M-H, Fixed, 95% CI) | 0.72 [0.63, 0.82] |
| 2.2 Diclofenac 50 mg | 8 | 930 | Risk Ratio (M-H, Fixed, 95% CI) | 0.50 [0.44, 0.58] |
| 2.3 Diclofenac 100 mg | 6 | 637 | Risk Ratio (M-H, Fixed, 95% CI) | 0.48 [0.41, 0.56] |
Analysis 1.1. Comparison 1 Diclofenac 25 mg v placebo, Outcome 1 Participants with at least 50% pain relief over 4 to 6 hours
Review: Single dose oral diclofenac for acute postoperative pain in adults
Comparison: 1 Diclofenac 25 mg v placebo
Outcome: 1 Participants with at least 50% pain relief over 4 to 6 hours
 |
Analysis 2.1. Comparison 2 Diclofenac 50 mg v placebo, Outcome 1 Participants with at least 50% pain relief over 4 to 6 hours
Review: Single dose oral diclofenac for acute postoperative pain in adults
Comparison: 2 Diclofenac 50 mg v placebo
Outcome: 1 Participants with at least 50% pain relief over 4 to 6 hours
 |
Analysis 2.2. Comparison 2 Diclofenac 50 mg v placebo, Outcome 2 Participants with at least 50% pain relief over 4 to 6 hours, dental or other surgery
Review: Single dose oral diclofenac for acute postoperative pain in adults
Comparison: 2 Diclofenac 50 mg v placebo
Outcome: 2 Participants with at least 50% pain relief over 4 to 6 hours, dental or other surgery
 |
Analysis 2.3. Comparison 2 Diclofenac 50 mg v placebo, Outcome 3 Participants with at least 50% pain relief over 4 to 6 hours, Na or K salt
Review: Single dose oral diclofenac for acute postoperative pain in adults
Comparison: 2 Diclofenac 50 mg v placebo
Outcome: 3 Participants with at least 50% pain relief over 4 to 6 hours, Na or K salt
 |
Analysis 3.1. Comparison 3 Diclofenac 100 mg v placebo, Outcome 1 Participants with at least 50% pain relief over 4 to 6 hours
Review: Single dose oral diclofenac for acute postoperative pain in adults
Comparison: 3 Diclofenac 100 mg v placebo
Outcome: 1 Participants with at least 50% pain relief over 4 to 6 hours
 |
Analysis 3.2. Comparison 3 Diclofenac 100 mg v placebo, Outcome 2 Participants with at least 50% pain relief over 4 to 6 hours, dental or other surgery
Review: Single dose oral diclofenac for acute postoperative pain in adults
Comparison: 3 Diclofenac 100 mg v placebo
Outcome: 2 Participants with at least 50% pain relief over 4 to 6 hours, dental or other surgery
 |
Analysis 3.3. Comparison 3 Diclofenac 100 mg v placebo, Outcome 3 Participants with at least 50% pain relief over 4 to 6 hours, Na or K salt
Review: Single dose oral diclofenac for acute postoperative pain in adults
Comparison: 3 Diclofenac 100 mg v placebo
Outcome: 3 Participants with at least 50% pain relief over 4 to 6 hours, Na or K salt
 |
Analysis 4.1. Comparison 4 Diclofenac versus placebo, Outcome 1 Participants with at least one adverse event
Review: Single dose oral diclofenac for acute postoperative pain in adults
Comparison: 4 Diclofenac versus placebo
Outcome: 1 Participants with at least one adverse event
 |
 |
Analysis 4.2. Comparison 4 Diclofenac versus placebo, Outcome 2 Participants using rescue medication at 6 hours
Review: Single dose oral diclofenac for acute postoperative pain in adults
Comparison: 4 Diclofenac versus placebo
Outcome: 2 Participants using rescue medication at 6 hours
 |
 |
Appendix 1. Search strategy for MEDLINE via Ovid
Diclofenac.sh
diclofenac.ti,ab,kw.
OR/1-2
Pain, postoperative.sh
((postoperative adj4 pain$) or (post-operative adj4 pain$) or post-operative-pain$ or (post$ NEAR pain$) or (postoperative adj4 analgesi$) or (post-operative adj4 analgesi$) or (“post-operative analgesi$”)).ti,ab,kw.
((post-surgical adj4 pain$) or (“post surgical” adj4 pain$) or (post-surgery adj4 pain$)).ti,ab,kw.
((“pain-relief after surg$”) or (“pain following surg$”) or (“pain control after”)).ti,ab,kw.
((“post surg$” or post-surg$) AND (pain$ or discomfort)).ti,ab,kw.
((pain$ adj4 “after surg$”) or (pain$ adj4 “after operat$”) or (pain$ adj4 “follow$ operat$”) or (pain$ adj4 “follow$ surg$”)).ti,ab,kw.
((analgesi$ adj4 “after surg$”) or (analgesi$ adj4 “after operat$”) or (analgesi$ adj4 “follow$ operat$”) or (analgesi$ adj4 “follow$ surg$”)).ti,ab,kw.
OR/4-10
randomized controlled trial.pt.
controlled clinical trial.pt.
randomized.ab.
placebo.ab.
drug therapy.fs.
randomly.ab.
trial.ab.
groups.ab.
OR/12-19
humans.sh.
20 AND 21
3 AND 11 AND 22
For the earlier review the following brand names were also searched:
allvoran; dolotren; nu-diclo; anfenax; ecofenac; olfen; apo-diclo; effekton; panamor; arcanafenac; fenac; pharmaflam; arthrotec; fenaren; polyflam; benfofen; flamrase; primofenac; brovaflamp; flector; rewodina; cataflam; flexagen; rheufenac; clinifam; flogofenac; rheumasan; dedolor; forgenac; rhumalgan; deflamat; fortfen; ribex; delphimix; grofenac; sigafenac; delphinac; inflamac; silino; diclac; isclofen; sodiclo; diclo; jenafenac; toryxil; diclobene; lexobene; tratul; dicloberl; liberalgium; valenac; diclofex; luase; veltex; diclomax; magluphen; voldal; diclomelan; monoflam; vologen; dicloreum; motifene; volraman; diclosyl; myogit; voltaren; diclozip; naclof; voltarene; dignofenac; novapirina; voltarol; dolobasan; novo-difenac; xenid.
Appendix 2. Search strategy for EMBASE via Ovid
Diclofenac.sh
diclofenac.ti,ab,kw.
OR/1-2
Postoperative pain.sh
((postoperative adj4 pain$) or (post-operative adj4 pain$) or post-operative-pain$ or (post$ NEAR pain$) or (postoperative adj4 analgesi$) or (post-operative adj4 analgesi$) or (“post-operative analgesi$”)).ti,ab,kw.
((post-surgical adj4 pain$) or (“post surgical” adj4 pain$) or (post-surgery adj4 pain$)).ti,ab,kw.
((“pain-relief after surg$”) or (“pain following surg$”) or (“pain control after”)).ti,ab,kw.
((“post surg$” or post-surg$) AND (pain$ or discomfort)).ti,ab,kw.
((pain$ adj4 “after surg$”) or (pain$ adj4 “after operat$”) or (pain$ adj4 “follow$ operat$”) or (pain$ adj4 “follow$ surg$”)).ti,ab,kw.
((analgesi$ adj4 “after surg$”) or (analgesi$ adj4 “after operat$”) or (analgesi$ adj4 “follow$ operat$”) or (analgesi$ adj4 “follow$ surg$”)).ti,ab,kw.
OR/4-10
clinical trials.sh
controlled clinical trials.sh
randomized controlled trial.sh
double-blind procedure.sh
(clin$ adj25 trial$).ab
((doubl$ or trebl$ or tripl$) adj25 (blind$ or mask$)).ab
placebo$.ab
random$.ab
OR/12-19
3 AND 11 AND 20
For the earlier review the following brand names were also searched:
allvoran; dolotren; nu-diclo; anfenax; ecofenac; olfen; apo-diclo; effekton; panamor; arcanafenac; fenac; pharmaflam; arthrotec; fenaren; polyflam; benfofen; flamrase; primofenac; brovaflamp; flector; rewodina; cataflam; flexagen; rheufenac; clinifam; flogofenac; rheumasan; dedolor; forgenac; rhumalgan; deflamat; fortfen; ribex; delphimix; grofenac; sigafenac; delphinac; inflamac; silino; diclac; isclofen; sodiclo; diclo; jenafenac; toryxil; diclobene; lexobene; tratul; dicloberl; liberalgium; valenac; diclofex; luase; veltex; diclomax; magluphen; voldal; diclomelan; monoflam; vologen; dicloreum; motifene; volraman; diclosyl; myogit; voltaren; diclozip; naclof; voltarene; dignofenac; novapirina; voltarol; dolobasan; novo-difenac; xenid.
Appendix 3. Search strategy for Cochrane CENTRAL
MESH descriptor Diclofenac
diclofenac:ti,ab,kw.
OR/1-2
MESH descriptor Pain, Postoperative
((postoperative adj4 pain$) or (post-operative adj4 pain$) or post-operative-pain$ or (post$ NEAR pain$) or (postoperative adj4 analgesi$) or (post-operative adj4 analgesi$) or (“post-operative analgesi$”)):ti,ab,kw.
((post-surgical adj4 pain$) or (“post surgical” adj4 pain$) or (post-surgery adj4 pain$)):ti,ab,kw.
((“pain-relief after surg$”) or (“pain following surg$”) or (“pain control after”)):ti,ab,kw.
((“post surg$” or post-surg$) AND (pain$ or discomfort)):ti,ab,kw.
((pain$ adj4 “after surg$”) or (pain$ adj4 “after operat$”) or (pain$ adj4 “follow$ operat$”) or (pain$ adj4 “follow$ surg$”)): ti,ab,kw.
((analgesi$ adj4 “after surg$”) or (analgesi$ adj4 “after operat$”) or (analgesi$ adj4 “follow$ operat$”) or (analgesi$ adj4 “follow$ surg$”)):ti,ab,kw.
OR/4-10
Clinical trials:pt.
Controlled Clinical Trial:pt.
Randomized Controlled Trial.pt.
MESH descriptor Double-Blind Method
(clin$ adj25 trial$):ti,ab,kw.
((doubl$ or trebl$ or tripl$) adj25 (blind$ or mask$)):ti,ab,kw.
placebo$:ti,ab,kw.
random$:ti,ab,kw.
OR/12-19
3 AND 11 AND 20
Appendix 4. Glossary
Categorical rating scale
The commonest is the five category scale (none, slight, moderate, good or lots, and complete). For analysis numbers are given to the verbal categories (for pain intensity, none=0, mild=1, moderate=2 and severe=3, and for relief none=0, slight=1, moderate=2, good or lots=3 and complete=4). Data from different subjects is then combined to produce means (rarely medians) and measures of dispersion (usually standard errors of means). The validity of converting categories into numerical scores was checked by comparison with concurrent visual analogue scale measurements. Good correlation was found, especially between pain relief scales using cross-modality matching techniques. Results are usually reported as continuous data, mean or median pain relief or intensity. Few studies present results as discrete data, giving the number of participants who report a certain level of pain intensity or relief at any given assessment point. The main advantages of the categorical scales are that they are quick and simple. The small number of descriptors may force the scorer to choose a particular category when none describes the pain satisfactorily.
VAS
Visual analogue scale: lines with left end labelled “no relief of pain” and right end labelled “complete relief of pain”, seem to overcome this limitation. Patients mark the line at the point which corresponds to their pain. The scores are obtained by measuring the distance between the no relief end and the patient’s mark, usually in millimetres. The main advantages of VAS are that they are simple and quick to score, avoid imprecise descriptive terms and provide many points from which to choose. More concentration and coordination are needed, which can be difficult post-operatively or with neurological disorders.
TOTPAR
Total pain relief (TOTPAR) is calculated as the sum of pain relief scores over a period of time. If a patient had complete pain relief immediately after taking an analgesic, and maintained that level of pain relief for 6 hours, they would have a 6-hour TOTPAR of the maximum of 24. Differences between pain relief values at the start and end of a measurement period are dealt with by the composite trapezoidal rule. This is a simple method that approximately calculates the definite integral of the area under the pain relief curve by calculating the sum of the areas of several trapezoids that together closely approximate to the area under the curve.
SPID
Summed pain intensity difference (SPID) is calculated as the sum of the differences between the pain scores over a period of time. Differences between pain intensity values at the start and end of a measurement period are dealt with by the trapezoidal rule.
VAS TOTPAR and VAS SPID are visual analogue versions of TOTPAR and SPID.
See “Measuring pain” in Bandolier’s Little Book of Pain, Oxford University Press, Oxford. 2003; pp 7-13 (Moore 2003).
HISTORY
Protocol first published: Issue 2, 2004
Review first published: Issue 2, 2004
| Date | Event | Description |
|---|---|---|
| 8 February 2011 | Amended | Contact details updated. |
| 24 September 2010 | Amended | Contact details updated. |
| 23 December 2008 | New citation required and conclusions have changed | Eight new studies (1206 participants in comparisons of diclofenac and placebo) were added in December 2008 (Chang 2002; Cooper 1996; Desjardins 2004; Hersh 2004; Hofele 2006; Kubitzek 2003; Torres 2004; Zuniga 2004). Overall the NNT for at least 50% pain relief over 4 to 6 hours was not changed, but the potassium salt was significantly better than the sodium salt |
| 26 September 2008 | New search has been performed | New studies added, analyses updated, additional data on use of rescue medication, and new authors |
| 22 May 2008 | Amended | Converted to new review format. |
WHAT’S NEW
Last assessed as up-to-date: 14 September 2011.
| Date | Event | Description |
|---|---|---|
| 15 September 2011 | Review declared as stable | The authors of this review scanned the literature in August 2011 and are confident that there should be no need to update this review until 2015 |
Footnotes
DECLARATIONS OF INTEREST RAM and HJM have consulted for various pharmaceutical companies. RAM and HJM have received lecture fees from pharmaceutical companies related to analgesics and other healthcare interventions. RAM, HJM and SD have received research support from charities, government and industry sources at various times. Support for this review came from Oxford Pain Research, the NHS Cochrane Collaboration Programme Grant Scheme, and NIHR Biomedical Research Centre Programme.
References to studies included in this review
- Ahlstrom 1993 {published data only} .Ahlstrom U, Bakshi R, Nilsson P, Wahlander L. The analgesic efficacy of diclofenac dispersible and ibuprofen in postoperative pain after dental extraction. European Journal of Clinical Pharmacology. 1993;44(6):587–8. doi: 10.1007/BF02440865. [DOI] [PubMed] [Google Scholar]
- Bakshi 1992 {published data only} .Bakshi R, Jacobs LD, Lehnert S, Picha B, Reuther J. A double-blind, placebo controlled trial comparing the analgesic efficacy of two formulations of diclofenac in postoperative dental pain. Current Therapeutic Research. 1992;52(3):435–42. [Google Scholar]
- Bakshi 1994 {published data only} .Bakshi R, Frenkel G, Dietlein G, Meurer Witt B, Schneider B, Sinterhauf U. A placebo-controlled comparative evaluation of diclofenac dispersible versus ibuprofen in postoperative pain after third molar surgery. Journal of Clinical Pharmacology. 1994;34(3):225–30. doi: 10.1002/j.1552-4604.1994.tb03990.x. [DOI] [PubMed] [Google Scholar]
- Chang 2002 {published data only} .Chang DJ, Desjardins PJ, Chen E, Polis AB, McAvoy M, Mockoviak SH, et al. Comparison of the analgesic efficacy of rofecoxib and enteric-coated diclofenac sodium in the treatment of postoperative dental pain: a randomized, placebo-controlled clinical trial. Clinical Therapeutics. 2002;24(4):490–503. doi: 10.1016/s0149-2918(02)85126-8. [DOI] [PubMed] [Google Scholar]
- Cooper 1996 {published data only} .Cooper SA, Cowan A, Tallarida RJ, Hargreaves K, Roszkowski M, Jamali F, et al. The analgesic interaction of misoprostol with nonsteroidal anti-inflammatory drugs. American Journal of Therapeutics. 1996;3(4):261–7. doi: 10.1097/00045391-199604000-00002. [DOI] [PubMed] [Google Scholar]
- Desjardins 2004 {published data only} .Desjardins PJ, Black PM, Daniels S, Bird SR, Fitzgerald BJ, Petruschke RA, et al. A randomized controlled study comparing rofecoxib, diclofenac sodium, and placebo in post-bunionectomy pain. Current Medical Research and Opinion. 2004;20(10):1523–37. doi: 10.1185/030079904X3069. [DOI] [PubMed] [Google Scholar]
- Herbertson 1995 {published data only} .Herbertson RM, Storey N. The comparative efficacy of diclofenac potassium, aspirin and placebo in the treatment of patients with pain following gynecologic surgery. Todays Therapeutic Trends. 1995;12(Suppl 1):33–45. [Google Scholar]
- Hersh 2004 {published data only} .Hersh EV, Levin LM, Adamson D, Christensen S, Kiersch TA, Noveck R, et al. Dose-ranging analgesic study of Prosorb diclofenac potassium in postsurgical dental pain. Clinical Therapeutics. 2004;26(8):1215–27. doi: 10.1016/s0149-2918(04)80033-x. [DOI: 10.1016/ S0149-2918(04)80033-X] [DOI] [PubMed] [Google Scholar]
- Hofele 2006 {published data only} .Hofele CM, Gyenes V, Daems LN, Stypula-Ciuba B, Wagener H, et al. Efficacy and tolerability of diclofenac potassium sachets in acute postoperative dental pain: a placebo-controlled, randomised, comparative study vs. diclofenac potassium tablets. International Journal of Clinical Practice. 2006;60(3):300–7. doi: 10.1111/j.1368-5031.2006.00828.x. [DOI: 10.1111/ j.1368-5031.2006.00828.x] [DOI] [PubMed] [Google Scholar]
- Kubitzek 2003 {published data only} .Kubitzek F, Ziegler G, Gold MS, Liu JM, Ionescu E. Analgesic efficacy of low-dose diclofenac versus paracetamol and placebo in postoperative dental pain. Journal of Orofacial Pain. 2003;17(3):237–44. [PubMed] [Google Scholar]
- Mehlisch 1995 {published data only} .Mehlisch DR, Brown P. Single-dose therapy with diclofenac potassium, aspirin or placebo following dental impaction surgery. Todays Therapeutic Trends. 1995;12(Suppl 1):15–31. [Google Scholar]
- Nelson 1994 {published data only} .Nelson SL, Brahim JS, Korn SH, Greene SS, Suchower LJ. Comparison of single-dose ibuprofen lysine, acetylsalicylic acid, and placebo for moderate-to-severe postoperative dental pain. Clinical Therapeutics. 1994;16(3):458–65. [PubMed] [Google Scholar]
- Olson 1997 {published data only} .Olson NZ, Sunshine A, Zighelboim I, DeCastro A. Onset and duration of analgesia of diclofenac potassium in the treatment of postepisiotomy pain. American Journal of Therapeutics. 1997;4:239–46. doi: 10.1097/00045391-199707000-00004. [DOI] [PubMed] [Google Scholar]
- Torres 2004 {published data only} .Torres LM, Cabrera J, MartÍnez J, Calderón E, Fernández S, Chaves J. The specific cox-2 inhibitor valdecoxib provides effective analgesia after inguinal hernia surgery. Revista Espanola Anestesiologia y Reanimacion. 2004;51(10):576–82. [PubMed] [Google Scholar]
- Zuniga 2004 {published data only} .Zuniga JR, Phillips CL, Shugars D, Lyon JA, Peroutka SJ, Swarbrick J, et al. Analgesic safety and efficacy of diclofenac sodium softgels on postoperative third molar extraction pain. Journal of Oral Maxillofacial Surgery. 2004;62(7):806–15. doi: 10.1016/j.joms.2003.12.019. [DOI: 10.1016/j.joms.2003.12.019] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
- Ahlstrom 1989 {published data only} .Ahlstrom U, Wahlander LA. Double-blind comparison of two different dosage recommendations for pain after surgical removal of a lower wisdom tooth. Current Therapeutic Research. 1989;45(3):495–501. [Google Scholar]
- Apaydin 1994 {published data only} .Apaydin A, Ozyuvaci H, Ordulu M, Disci R. Postoperative pain relief by single dose diclofenac kalium and etodolac. A comparative clinical study. The Journal of The Turkish Society of Algology. 1994;6(4):28–34. [Google Scholar]
- Aranda 1989 {published data only} .Aranda B, Bor YM. Comparative study between the efficacy of aluminum acetotartrate poultice and diclofenac in the postoperative treatment of degenerative knees [Etude du cataplasme d’acetotartrate d’alumine versus diclofenac dans le traitmente post–operatoire des genoux degeneratifs] Comptes Rendus de Thérapeutique et de Pharmacologie Clinique. 1989;7(80):11–7. [Google Scholar]
- Carlos 1984 {published data only} .Carlos DE. Comparative study of the efficacy of diclofenac NA, meperidine HCL and nalbuphine HCL in postoperative analgesia. Philippine Journal of Internal Medicine. 1984;22(1):51–5. [Google Scholar]
- Dorfmann 1991 {published data only} .Dorfmann H. Controlled therapeutic trial of diclofenac in meniscectomy under arthroscopy [Essai therapeutique controle du diclofenac dans les meniscectomies sous arthroscopie] Revue du Rhumatisme et des Maladies Osteo-Articulaires. 1991;58(1):59–61. [PubMed] [Google Scholar]
- El-Tanany 1993 {published data only} .El-Tanany H, Boghdady W. A double blind comparative study of Diclofenac-K and Glafenine in the management of acute dental pain. Cairo Dental Journal. 1993;9(2):117–20. [Google Scholar]
- Fineschi 1997 {published data only} .Fineschi G, Tamburrelli FC, Francucci BM, Pisati R. Oral diclofenac dispersible provides a faster onset of analgesia than intramuscular ketorolac in the treatment of postoperative pain. Clinical Drug Investigation. 1997;13:1–7. [Google Scholar]
- Frezza 1985 {published data only} .Frezza R, Bolognesi P, Bernardi F. Comparison of the action of 3 non-steroidal anti-inflammatory agents in the control of post-operative pain. Effectiveness of NSAID against pain [Confronto sull’azione di tre antinfiammatori non steroidei nel controllo de dolore odontoiatrico post–chirurgico. Efficaci i FANS contro il dolore] Attualita Dentale. 1985;1(30):40–2. [PubMed] [Google Scholar]
- Garcia 1997 {published data only} .Garcia DC, Espinosa JD, Marti ML. Analgesic efficacy of both lisine clonixinate and diclofenac for postsurgical pain during ambulatory surgery. Prensa Medica Argentina. 1997;84:1061–5. [Google Scholar]
- Graf 2000 {published data only} .Graf von Ingelheim FA. A homeopathic drug is equivalent to diclofenac? Der Orthopade. 2000;29:596. doi: 10.1007/s001320050498. [DOI] [PubMed] [Google Scholar]
- Henderson 1994 {published data only} .Henderson RC. A double-blind comparison of diclofenac potassium and naproxen sodium in the treatment of pain due to orthopedic skeletal surgery. Todays Therapeutic Trends. 1994;12(S1):81–95. [Google Scholar]
- Henrikson 1982 {published data only} .Henrikson PA, Thilander H, Wahlander LA. Absorption and effect of diclofenac-sodium after surgical removal of a lower wisdom tooth. Current Therapeutic Research. 1982;31(1):20–6. [Google Scholar]
- Hultin 1978 {published data only} .Hultin M, Olander KJ. A clinical trial of the analgesic properties of Voltaren (diclofenac sodium) Scandinavian Journal of Rheumatology. Supplement. 1978;22:42–5. doi: 10.3109/03009747809097215. [DOI] [PubMed] [Google Scholar]
- Iqbal 1986 {published data only} .Iqbal KM, Biswas GK, Mondo SK, Afzalunnessa B. Assessment of post operative analgesia: A comparative study of pethidine and diclofenac sodium. Journal of Bangladesh College of Physicians and Surgeons. 1986;4(1):1–7. [Google Scholar]
- Iwabuchi 1980 {published data only} .Iwabuchi T, Soma S. Use of Voltaren for relief of post-extraction pain. Shikai Tenbo [Dental Outlook] 1980;55(2):367–70. [PubMed] [Google Scholar]
- Joubert 1977 {published data only} .Joubert JJ. An assessment of the efficacy and tolerability of Voltaren in the treatment of inflammation after extractionof teeth. Journal of the Dental Association of South Africa. 1977;32:581–3. [PubMed] [Google Scholar]
- Kittala 1972 {published data only} .Kittala S, Aizawa M, Tokue I, Suge Y. Efficacy of GP-45840 on after-pains. Clinical trial with double blind method. Shinryo To Shinyaku [Medical Consultation and New Remedies] 1972;9(6):1123. [Google Scholar]
- Li 1998 {published data only} .Li X, Wu XC, Zhao LL. Randomised controlled study of the effect of diclofenac potassium and keflan. Chinese Journal of Pharmacoepidemiology. 1998;7:69–71. [Google Scholar]
- Matthews 1984 {published data only} .Matthews RW, Scully CM, Levers BG. The efficacy of diclofenac sodium (Voltarol) with and without paracetamol in the control of post surgical dental pain. British Dental Journal. 1984;157(10):357–9. doi: 10.1038/sj.bdj.4805486. [DOI] [PubMed] [Google Scholar]
- Mayer 1980 {published data only} .Mayer M, Weiss P. Antiphlogistic and analgesic effect of diclofenac sodium after maxillofacial interventions in a double-blind trial [Uber die antiphlogistische und analgetische Wirkung von Diclofenac–Na nach kieferchirurgischen Eingriffen im Doppelblindversuch] Deutsche Zahnarztliche Zeitschrift. 1980;35(5):559–63. [PubMed] [Google Scholar]
- Nakanishi 1990 {published data only} .Nakanishi M, Mizukawa N, Koyama S, Takagi S, Nishijima K. Clinical evaluation of Amfenac sodium compared with Diclofenac sodium. Journal of Oral Therapeutics and Pharmacology. 1990;9(2):85–92. [Google Scholar]
- Rautela 1998 {published data only} .Rautela RS, Kumar A, Gupta A, Bhattacharya A. A randomised double blind comparison of ketorolac and diclofenac for post-operative analgesia following major gynaecological surgery. Journal of Anesthesiology Clinical Pharmacology. 1998;14:79–81. [Google Scholar]
- Shimura 1981 {published data only} .Shimura T, Otaka Y, Ando N, Nagao H. Voltaren tablets for the pain following tooth extraction - studies of its analgesic effects. Shikai Tenbo [Dental Outlook] 1981;58(1):175–83. [PubMed] [Google Scholar]
- Tam 2001 {published data only} .Tam WH, Yuen PM. Use of diclofenac as an analgesic in outpatient hysteroscopy: a randomized, double-blind, placebo-controlled study. Fertility and Sterility. 2001;76(5):1070–2. doi: 10.1016/s0015-0282(01)02832-1. [DOI] [PubMed] [Google Scholar]
- Tani 1974 {published data only} .Tani I. Therapeutic results of Voltaren tablets an analgesic anti-inflammatory agent in pain following tonsillectomy. Shinryo To Shinyaku [Medical Consultation and New Remedies] 1974;11(8):274. [Google Scholar]
- Tesseroli 1986 {published data only} .Tesseroli de Siqueira JT, Potenza BJ, Basta D. Evaluation of the analgesic efficacy of potassium diclofenac and placebo in postoperative treatment of dental surgery. Multicentre, double blind study [Avaliacao do eficacia analgesicado diclofenaco potassico e placebo no pos–operatorio de cirurgias para extracoes dentarias. Estudo multicentrico, dupl–cego] Revista Paulista de Odontologia. 1986;6:2–7. [Google Scholar]
- Ujpal 1999 {published data only} .Ujpal M, Biczo A, Huszar L, Temesvari A, Tothfalusi L, Szabo G. Comparative study of the analgesic effect of apranax and cataflam after oral surgery procedures [Az apranax es a cataflam fajdalomesillapito hatasanak osszehasonlito vizsgalata szajsebeszeti beavatkozast kovetoen] Fogorvosi Szemle. 1999;92(12):374–8. [PubMed] [Google Scholar]
- Vigneron 1977 {published data only} .Vigneron JR, Thys R. Study of the anti-inflammatory and analgesic actions of diclofenac in traumatology and orthopedic surgery [Etude de l’action anti–inflammatoire et antalgique du diclofenac en traumatologie et chirurgie orthopedique] Revue Medicale de Liege. 1977;32(1):10–4. [PubMed] [Google Scholar]
- Walton 1993 {published data only} .Walton GM, Rood JP, Snowdon AT, Rickwood D. Ketorolac and diclofenac for postoperative pain relief following oral surgery. British Journal of Oral Maxillofacial Surgery. 1993;31(3):158–60. doi: 10.1016/0266-4356(93)90115-d. [DOI] [PubMed] [Google Scholar]
- Wuolijoki 1987 {published data only} .Wuolijoki E, Oikarinen VJ, Ylipaavalniemi P, Hampf G, Tolvanen M. Effective postoperative pain control by preoperative injection of diclofenac. European Journal of Clinical Pharmacology. 1987;32(3):249–52. doi: 10.1007/BF00607571. [DOI] [PubMed] [Google Scholar]
- Zhang 2000 {published data only} .Zhang SL, Meng ZY, Xu JH, Shou BQ. Analgesic efficacy of diclofenac potassium in dental pain trial. Journal of Medical Postgraduate. 2000;13:24–5. [Google Scholar]
Additional references
- Barden 2004b .Barden J, Edwards J, Moore RA, McQuay HJ. Single dose oral rofecoxib for postoperative pain. Cochrane Database of Systematic Reviews. 2004;(Issue 4) doi: 10.1002/14651858.CD004604. [DOI: 10.1002/ 14651858.CD004604.pub2] [DOI] [PubMed] [Google Scholar]
- BNF 2002 .Mehta DK, editor. British National Formulary. 43. Vol. British Medical Journal; London: Mar, 2002. Non-steroidal anti-inflammatory drugs; p. 482. [Google Scholar]
- Collins 1997 .Collins SL, Moore RA, McQuay HJ. The visual analogue pain intensity scale: what is moderate pain in millimetres? Pain. 1997;72:95–7. doi: 10.1016/s0304-3959(97)00005-5. [DOI] [PubMed] [Google Scholar]
- Collins 1999 .Collins SL, Moore RA, McQuay HJ, Wiffen PJ, Edwards JE. Single dose oral ibuprofen and diclofenac for postoperative pain. Cochrane Database of Systematic Reviews. 1999;(Issue 2) doi: 10.1002/14651858.CD001548. [DOI: 10.1002/14651858.CD001548] [DOI] [PubMed] [Google Scholar]
- Collins 2001 .Collins SL, Edwards JE, Moore RA, Smith LA, McQuay HJ. Seeking a simple measure of analgesia for mega-trials: is a single global assessment good enough? Pain. 2001;91(1-2):189–94. doi: 10.1016/s0304-3959(00)00435-8. [DOI] [PubMed] [Google Scholar]
- Cook 1995 .Cook RJ, Sackett DL. The number needed to treat: a clinically useful measure of treatment effect. British Medical Journal. 1995;310:452–4. doi: 10.1136/bmj.310.6977.452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper 1991 .Cooper SA. Single-dose analgesic studies: the upside and downside of assay sensitivity. In: Max MB, Portenoy RK, Laska EM, editors. The design of analgesic clinical trials. Advances in Pain Research and Therapy. Vol. 18. Raven Press; New York: 1991. pp. 117–24. [Google Scholar]
- Derry 2008 .Derry S, Moore RA, McQuay HJ. Single dose oral celecoxib for acute postoperative pain. Cochrane Database of Systematic Reviews. 2008;(Issue 4) doi: 10.1002/14651858.CD004233.pub2. [DOI: 10.1002/ 14651858.CD004233] [DOI] [PubMed] [Google Scholar]
- Derry 2009 .Derry C, Derry S, Moore RA, McQuay HJ. Single dose oral naproxen and naproxen sodium for acute postoperative pain in adults. Cochrane Database of Systematic Reviews. 2009;(Issue 1) doi: 10.1002/14651858.CD004234.pub3. [Art. No.: CD004234. DOI: 10.1002/ 14651858.CD004234.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Desjardins 2004 .Desjardins PJ, Black PM, Daniels S, Bird SR, Fitzgerald BJ, Petruschke RA, et al. A randomized controlled study comparing rofecoxib, diclofenac sodium, and placebo in post-bunionectomy pain. Current Medical Research and Opinion. 2004;20(10):1523–37. doi: 10.1185/030079904X3069. [DOI] [PubMed] [Google Scholar]
- Edwards 1999 .Edwards JE, McQuay HJ, Moore RA, Collins SL. Reporting of adverse effects in clinical trials should be improved. Lessons from acute postoperative pain. Journal of Pain and Symptom Management 1999. 1999;18:427–37. doi: 10.1016/s0885-3924(99)00093-7. [DOI] [PubMed] [Google Scholar]
- Fitzgerald 2001 .FitzGerald GA, Patrono C. The coxibs, selective inhibitors of cyclooxygenase-2. New England Journal of Medicine. 2001;345(6):433–42. doi: 10.1056/NEJM200108093450607. [DOI] [PubMed] [Google Scholar]
- Forrest 2002 .Forrest JB, Camu F, Greer IA, Kehlet H, Abdalla M, Bonnet F. Ketorolac, diclofenac, and ketoprofen are equally safe for pain relief after major surgery. British Journal of Anaesthesia. 2002;88(2):227–33. doi: 10.1093/bja/88.2.227. [DOI] [PubMed] [Google Scholar]
- Grahame-Smith 2002 .Grahame-Smith DG, Aronson JK. Oxford textbook of clinical pharmacology and drug therapy. 3rd Edition. Oxford University Press; Oxford: 2002. [ISBN: 13: 978–0–19–263234–0] [Google Scholar]
- Hawkey 1999 .Hawkey CJ. Cox-2 inhibitors. Lancet. 1999;353(9149):307–14. doi: 10.1016/s0140-6736(98)12154-2. [DOI] [PubMed] [Google Scholar]
- Hernández-Díaz 2001 .Hernández-Díaz S, García-Rodríguez LA. Epidemiologic assessment of the safety of conventional nonsteroidal anti-inflammatory drugs. American Journal of Medicine. 2001;110(Suppl 3A):20S–7S. doi: 10.1016/s0002-9343(00)00682-3. [DOI: 110.1016/S0002-9343 (00)00682-3] [DOI] [PubMed] [Google Scholar]
- Jadad 1996a .Jadad AR, Carroll D, Moore A, McQuay H. Developing a database of published reports of randomised clinical trials in pain research. Pain. 1996;66:239–46. doi: 10.1016/0304-3959(96)03033-3. [DOI] [PubMed] [Google Scholar]
- Jadad 1996b .Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJM, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Controlled Clinical Trials. 1996;17:1–12. doi: 10.1016/0197-2456(95)00134-4. [DOI] [PubMed] [Google Scholar]
- L’Abbé 1987 .L’Abbé KA, Detsky AS, O’Rourke K. Meta-analysis in clinical research. Annals of Internal Medicine. 1987;107:224–33. doi: 10.7326/0003-4819-107-2-224. [DOI] [PubMed] [Google Scholar]
- Martindale 1996 .Reynolds JEF, Parfitt K, Parsons AV, Sweetman SC, editors. Martindale: The extra pharmacopoeia. Vol. 31. Royal Pharmaceutical Society; London: 1996. Analgesics Anti-inflammatory Agents and Antipyretics; p. 36. [ISBN: 0–85369–342–0] [Google Scholar]
- McQuay 1982 .McQuay HJ, Bullingham RE, Moore RA, Evans PJ, Lloyd JW. Some patients don’t need analgesics after surgery. Journal of the Royal Society of Medicine. 1982;75(9):705–8. [PMC free article] [PubMed] [Google Scholar]
- McQuay 2005 .McQuay HJ, Moore RA. Placebo. Postgraduate Medical Journal. 2005;81:155–60. doi: 10.1136/pgmj.2004.024737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moher 1999 .Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of meta-analyses of randomised controlled trials: the QUOROM statement. The Lancet. 1999;354:1896–900. doi: 10.1016/s0140-6736(99)04149-5. [DOI] [PubMed] [Google Scholar]
- Moore 1996 .Moore A, McQuay H, Gavaghan D. Deriving dichotomous outcome measures from continuous data in randomised controlled trials of analgesics. Pain. 1996;66(2-3):229–37. doi: 10.1016/0304-3959(96)03032-1. [DOI] [PubMed] [Google Scholar]
- Moore 1997a .Moore A, McQuay H, Gavaghan D. Deriving dichotomous outcome measures from continuous data in randomised controlled trials of analgesics: verification from independent data. Pain. 1997;69(1-2):127–30. doi: 10.1016/s0304-3959(96)03251-4. [DOI] [PubMed] [Google Scholar]
- Moore 1997b .Moore A, Moore O, McQuay H, Gavaghan D. Deriving dichotomous outcome measures from continuous data in randomised controlled trials of analgesics: Use of pain intensity and visual analogue scales. Pain. 1997;69(3):311–5. doi: 10.1016/S0304-3959(96)03306-4. [DOI] [PubMed] [Google Scholar]
- Moore 1998 .Moore RA, Carroll D, Wiffen PJ, Tramer M, McQuay HJ. A systematic review of topically-applied non-steroidal anti-inflammatory drugs. BMJ. 1998;316:333–8. doi: 10.1136/bmj.316.7128.333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore 2003 .Moore RA, Edwards J, Barden J, McQuay HJ. Bandolier’s Little Book of Pain. Oxford University Press; Oxford: 2003. [Google Scholar]
- Moore 2005 .Moore RA, Edwards JE, McQuay HJ. Acute pain: individual patient meta-analysis shows the impact ofdifferent ways of analysing and presenting results. Pain. 2005;116(3):322–31. doi: 10.1016/j.pain.2005.05.001. [DOI: 10.1016/j.pain.2005.05.001] [DOI] [PubMed] [Google Scholar]
- Morris 1995 .Morris JA, Gardner MJ. Calculating confidence intervals for relative risk, odds ratio and standardised ratios and rates. In: Gardner MJ, Altman DG, editors. Statistics with confidence - confidence intervals and statistical guidelines. British Medical Journal; London: 1995. pp. 50–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oldman 2000 .Oldman A, Smith LA, Collins S, Carroll D, Wiffen PJ, McQuay HJ, et al. Single dose oral aspirin for acute pain. Cochrane Database of Systematic Reviews. 2000;(Issue 2) doi: 10.1002/14651858.CD002067. [DOI: 10.1002/14651858.CD002067] [DOI] [PubMed] [Google Scholar]
- PACT 2007 .Prescription Cost Analysis. England: 2007. [ISBN: 978–1–84636–210–1] [Google Scholar]
- Rapoport 1999 .Rapoport RJ. The Safety of NSAIDs and Related Drugs for the Management of Acute Pain: Maximizing Benefits and Minimizing Risks. Cancer Control. 1999;6(2 Suppl 1):18–21. doi: 10.1177/107327489900602S04. [DOI] [PubMed] [Google Scholar]
- Roy 2007 .Roy YM, Derry S, Moore RA. Single dose oral lumiracoxib for postoperative pain. Cochrane Database of Systematic Reviews. 2007;(Issue 4) doi: 10.1002/14651858.CD006865. [DOI: 10.1002/ 14651858.CD006865] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toms 2008 .Toms L, McQuay HJ, Derry S, Moore RA. Single dose oral paracetamol (acetaminophen) for postoperative pain in adults. Cochrane Database of Systematic Reviews. 2008;(Issue 4) doi: 10.1002/14651858.CD004602.pub2. [DOI: 10.1002/14651858.CD004602] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tramèr 1997 .Tramèr MR, Reynolds DJM, Moore RA, McQuay HJ. Impact of covert duplicate results on meta-analysis: a case study. BMJ. 1997;315:635–9. doi: 10.1136/bmj.315.7109.635. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
- Barden 2004a .Barden J, Edwards J, Moore RA, McQuay HJ. Single dose oral diclofenac for postoperative pain. Cochrane Database of Systematic Reviews. 2004;(Issue 2) doi: 10.1002/14651858.CD004768. [DOI: 10.1002/ 14651858.CD004768] [DOI] [PubMed] [Google Scholar]
- Collins 1998 .Collins SL, Moore RA, McQuay HJ, Wiffen PJ. Oral ibuprofen and diclofenac in postoperative pain: a quantitative systematic review. European Journal of Pain. 1998;2(4):285–91. doi: 10.1016/s1090-3801(98)90027-1. [DOI] [PubMed] [Google Scholar]
- * Indicates the major publication for the study