

Abstract
Background
Miscarriage is the premature expulsion of an embryo or fetus from the uterus up to 23 weeks of pregnancy and weighing up to 500 grams. International studies using diagnostic tools have identified that some women suffer from anxiety, depression and grief after miscarriage. Psychological follow‐up might detect those women who are at risk of psychological complications following miscarriage. This review is necessary as the evidence is equivocal on the benefits of psychological follow‐up after miscarriage.
Objectives
Whether follow‐up affects the psychological well being of women following miscarriage.
Search methods
We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (31 December 2011), reference lists of all retrieved papers and contacted professional and lay organisations to obtain any ongoing trials or unpublished data.
Selection criteria
Randomised controlled trials only.
Data collection and analysis
All potential trials for eligibility according to the criteria specified in the protocol by screening the titles and abstracts, retrieving full reports of potentially relevant trials for assessment. All review authors extracted data and checked for accuracy. No studies were published in duplicate. When data were missing and only the abstract was available, we attempted to contact the trial authors. We resolved any disagreement through discussion.
Main results
Six studies involving 1001 women were included. Three trials compared one counselling session with no counselling. There was no significant difference in psychological well being including anxiety, grief, depression avoidance and self‐blame. One trial compared three one‐hour counselling sessions with no counselling at four and 12 months. Some subscales showed statistical significance in favour of counselling and some in favour of no counselling. The results for two trials were given in narrative form as data were unavailable for meta‐analyses. One trial compared multiple interventions. The other trial compared two counselling sessions with no counselling. Neither study favoured counselling.
Authors' conclusions
Evidence is insufficient to demonstrate that psychological support such as counselling is effective post‐miscarriage. Further trials should be good quality, adequately‐powered using standardised interventions and outcome measures at specific time points. The economic implications and women's satisfaction with psychological follow‐up should also be explored in any future study.
Keywords: Female; Humans; Pregnancy; Abortion, Spontaneous; Abortion, Spontaneous/psychology; Anxiety; Anxiety/therapy; Counseling; Counseling/methods; Depression; Depression/therapy; Follow‐Up Studies; Psychotherapy; Psychotherapy/methods; Randomized Controlled Trials as Topic; Stress, Psychological; Stress, Psychological/therapy
Plain language summary
Follow‐up for improving psychological well being for women after a miscarriage
Miscarriage is the premature, or loss of a fetus, up to 23 weeks of pregnancy. Some women suffer from anxiety and depression after miscarriage which may be part of their grief following the loss. Psychological follow‐up might detect those women who are at risk of psychological complications following miscarriage. This review of six studies, involving 1001 women, found that there is insufficient evidence from randomised controlled trials to recommend any method of psychological follow‐up. Timing of the counselling interventions varied from one week following miscarriage up to 11 weeks. In all studies the interventions were delivered by different professional groups including a midwife, psychologists and nurses. Measurements of the outcomes were made from one month to 12 months after miscarriage in the different studies, which highlights the uncertainty surrounding the rate of psychological recovery following miscarriage. The two larger studies included a complex combination of interventions and outcome measures so that any potentially significant effects may have been diluted.
Further robust research is needed to determine if any recognised psychological follow‐up is effective is hastening psychological recovery following miscarriage.
Background
Description of the condition
Although definitions of miscarriage vary internationally, it is defined by the World Health Organization (WHO) as the premature expulsion of an embryo or fetus from the uterus up to 23 weeks of pregnancy and weighing up to 500 grams (WHO 2001). Early pregnancy loss is defined as a confirmed empty sac or sac with fetus but with no fetal heart activity at less than 12 weeks' gestation (Farquharson 2005; RCOG 2006). It is difficult to quantify precisely how many women will have a miscarriage but in a longitudinal Swedish study, Blohm 2008 found that clinical miscarriage constituted 12% of all pregnancies, and 25% of women who had been pregnant by 39 years of age had experienced at least one miscarriage.
This review will focus on spontaneous miscarriage and will not include elective termination of pregnancy, ectopic pregnancy, stillbirth and neonatal death.
There are various categorisations of miscarriage, in that a miscarriage may be complete with all the products of conception passed or incomplete in which some of the products are retained within the uterus. There is an additional category of ‘silent’ miscarriage or early fetal demise in which the fetus may have been dead for some weeks but has not yet been expelled from the uterus (Trinder 2006). The characteristic symptoms of miscarriage are vaginal blood loss which may be accompanied by pain.
Physical management of women with miscarriage in the UK optimally involves rapid referral to an early pregnancy unit with ultrasound confirmation that the pregnancy is not viable. Management will depend on the category of miscarriage and the woman’s clinical condition; women may be offered the option of expectant management where there is no active medical intervention with the miscarriage proceeding of its own accord. Other options are surgical management, in which the retained products of conception are evacuated usually under general anaesthetic; and medical intervention, in which medications are given to induce uterine contractions and evacuation of retained products usually without the need for surgical intervention (RCOG 2006). Systematic reviews by Nanda 2006 and Neilson 2010 suggest that all of these treatments are acceptable and women should be supported to make the choice of treatment which is most suitable for them.
Unlike physical management of women following miscarriage, the evidence on psychological management is less well developed and is the focus of this review. There has been increased awareness of the psychological consequences of miscarriage for women and their partners. International studies using diagnostic tools identified that some women suffer from anxiety and depression after miscarriage (Neugebauer 1997; Nikcevic 1999; Stirtzinger 1999). These and other feelings that women describe have been conceptualised by many as being part of a pattern of grief in response to the loss of a baby (Frost 2007; Malacrida 1998; Mander 1997). Accounts from women about their hospital experiences in one study were critical of how health professionals cared for them with little awareness of their feelings of distress and no effective interventions to support them (Stratton 2008).
Description of the intervention
Strategies to provide some kind of psychological follow‐up after miscarriage have been proposed. However, these are characterised by their diversity both in terms of the type of follow‐up and who provides it. They range from telephone counselling provided by women who have already had a miscarriage to more formal counselling programmes. The mode of intervention could be passive, such as written or electronic information, or active, via telephone, clinic appointment or one‐to‐one or group support.
How the intervention might work
Follow‐up might detect those women who are at risk of developing or who actually have psychological complications following miscarriage such as anxiety, distress and depression. The United Kingdom RCOG guidelines (RCOG 2006) on the management of women after early pregnancy loss state that support and counselling for women after miscarriage can have significant positive effects on psychological well being. However, a Cochrane review of support after perinatal death, concluded that there is insufficient evidence that such interventions are beneficial (Flenady 2008). Similarly, Stratton 2008 in a review of hospital‐based interventions, found little evidence to suggest that follow‐up after miscarriage has positive outcomes. It is possible that psychological follow‐up could reduce any adverse effects on women such as on their employment, relationships with their partners and other close family members.
Why it is important to do this review
Currently once any complications are detected via follow‐up, women can be referred to specific agencies which will provide interventions to manage these complications and reduce any adverse psychological outcomes following miscarriage. There is a need to systematically review the evidence on follow‐up after miscarriage as it is not known which interventions are effective.
Objectives
Primary
To identify whether follow‐up by healthcare professionals or lay organisations at any time affects the psychological well being of women following miscarriage.
Secondary
To compare the effects of different types of interventions on the psychological well being of women following miscarriage.
Methods
Criteria for considering studies for this review
Types of studies
All published and unpublished randomised controlled trials including cluster trials that compare different methods of follow‐up after miscarriage. We did not include quasi‐randomised trials (e.g. trials that allocate treatment by sequential record number, sequential admitting number, by day of the week).
Types of participants
Females of child‐bearing age experiencing miscarriage defined as premature expulsion of an embryo or fetus from the uterus up to 23 weeks of pregnancy and weighing up to 500 grams (WHO 2001).
Types of interventions
We considered trials if they compared interventions following miscarriage.
Psychological intervention versus no intervention.
Psychological intervention versus usual care.
Psychological intervention versus another psychological intervention.
Types of outcome measures
Primary outcomes
Psychological well being as defined by the trial authors.
Patient satisfaction as defined by the trial authors.
Secondary outcomes
Adverse reaction to follow‐up.
Referral to primary healthcare services.
Admission to hospital.
Costs associated with follow‐up.
Search methods for identification of studies
Electronic searches
We contacted the Trials Search Co‐ordinator to search the Cochrane Pregnancy and Childbirth Group’s Trials Register (31 December 2011).
The Cochrane Pregnancy and Childbirth Group’s Trials Register is maintained by the Trials Search Co‐ordinator and contains trials identified from:
quarterly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
weekly searches of MEDLINE;
weekly searches of EMBASE;
handsearches of 30 journals and the proceedings of major conferences;
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Details of the search strategies for CENTRAL, MEDLINE and EMBASE, the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service can be found in the ‘Specialized Register’ section within the editorial information about the Cochrane Pregnancy and Childbirth Group.
Trials identified through the searching activities described above are each assigned to a review topic (or topics). The Trials Search Co‐ordinator searches the register for each review using the topic list rather than keywords.
Searching other resources
We searched reference lists of all retrieved papers for additional studies and contacted professional and lay organisations in order to obtain any ongoing trials or unpublished data.
We did not apply any language restrictions.
Data collection and analysis
We assessed all potential trials for eligibility according to the criteria specified in the protocol by screening the titles and abstracts. We retrieved full reports of potentially relevant trials for assessment of eligibility based on the inclusion criteria. All review authors extracted the data and checked for accuracy, and we resolved discrepancies by discussion. No studies were published in duplicate. When data were missing, or if only the abstract was available, we attempted to contact the trial authors to obtain the missing information. We resolved any disagreement through discussion or we consulted the Pregnancy and Childbirth Review Group.
Selection of studies
All review authors independently assessed for inclusion all the potential studies we identified as a result of the search strategy.
Data extraction and management
We designed a form to extract data. For eligible studies, all review authors extracted the data using the agreed form. We entered data into Review Manager software (RevMan 2011) and checked for accuracy.
When information regarding any of the above was unclear, we attempted to contact authors of the original reports to provide further details.
Assessment of risk of bias in included studies
All review authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
(1) Random sequence generation (checking for possible selection bias)
We described for each included study the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
We assessed the method as:
low risk of bias (any truly random process, e.g. random number table; computer random number generator);
high risk of bias (any non‐random process, e.g. odd or even date of birth; hospital or clinic record number);
unclear risk of bias.
(2) Allocation concealment (checking for possible selection bias)
We described for each included study the method used to conceal allocation to interventions prior to assignment and assessed whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as:
low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
unclear risk of bias.
(3.1) Blinding of participants and personnel (checking for possible performance bias)
We described for each included study the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. We consider that studies are at low risk of bias if they were blinded, or if we judge that the lack of blinding would be unlikely to affect results. We assess blinding separately for different outcomes or classes of outcomes.
We assessed the methods as:
low, high or unclear risk of bias for participants;
low, high or unclear risk of bias for personnel.
(3.2) Blinding of outcome assessment (checking for possible detection bias)
We described for each included study the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed methods used to blind outcome assessment as:
low, high or unclear risk of bias.
(4) Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data)
We described for each included study, and for each outcome or class of outcomes, the completeness of data including attrition and exclusions from the analysis. We stated whether attrition and exclusions were reported and the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported, or could be supplied by the trial authors, we re‐included missing data in the analyses which we undertook.
We assessed methods as:
low risk of bias (e.g. no missing outcome data; missing outcome data balanced across groups);
high risk of bias (e.g. numbers or reasons for missing data imbalanced across groups; ‘as treated’ analysis done with substantial departure of intervention received from that assigned at randomisation);
unclear risk of bias.
(5) Selective reporting (checking for reporting bias)
We described for each included study how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
low risk of bias (where it is clear that all of the study’s pre‐specified outcomes and all expected outcomes of interest to the review have been reported);
high risk of bias (where not all the study’s pre‐specified outcomes have been reported; one or more reported primary outcomes were not prespecified; outcomes of interest are reported incompletely and so cannot be used; study fails to include results of a key outcome that would have been expected to have been reported);
unclear risk of bias.
(6) Other bias (checking for bias due to problems not covered by (1) to (5) above)
We described for each included study any important concerns we may have had about other possible sources of bias. Was the trial stopped early due to some data‐dependent process? Was there extreme baseline imbalance?
We assessed whether each study was free of other problems that could put it at risk of bias:
low risk of other bias;
high risk of other bias;
unclear whether there is risk of other bias.
(7) Overall risk of bias
We made explicit judgements about whether studies were at high risk of bias, according to the criteria given in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). With reference to (1) to (6) above, we assessed the likely magnitude and direction of the bias and whether we considered it was likely to impact on the findings. We explored the impact of the level of bias through undertaking sensitivity analyses ‐ seeSensitivity analysis.
Measures of treatment effect
Dichotomous data
For dichotomous data, we planned to present results as summary risk ratio with 95% confidence intervals.
Continuous data
For continuous data, we intended to use the mean difference if outcomes were measured in the same way between trials. We used the standardised mean difference to combine trials that measured the same outcome, but used different methods.
Unit of analysis issues
Cluster‐randomised trials
If identified, we would have included cluster‐randomised trials in the analyses along with individually randomised trials. We would have adjusted their sample sizes using the methods described in the Cochrane Handbook for Systematic Reviews of Interventions using an estimate of the intracluster correlation co‐efficient (ICC) derived from the trial (if possible), or from another source. If ICCs from other sources had been used, we would have reported this and conducted sensitivity analyses to investigate the effect of variation in the ICC. If we had identified both cluster‐randomised trials and individually‐randomised trials, we planned to synthesise the relevant information. We considered it reasonable to combine the results from both if there was little heterogeneity between the study designs and the interaction between the effect of intervention and the choice of randomisation unit was considered to be unlikely.
We also acknowledged heterogeneity in the randomisation unit and would have performed a separate sensitivity analysis to investigate the effects of the randomisation unit.
Dealing with missing data
For included studies, we noted levels of attrition. We explored the impact of including studies with high levels of missing data in the overall assessment of treatment effect by using Sensitivity analysis.
For all outcomes we carried out analyses, as far as possible, on an intention‐to‐treat basis, i.e. we attempted to include all participants randomised to each group in the analyses and all participants would have been analysed in the group to which they were allocated, regardless of whether or not they received the allocated intervention.The denominator for each outcome in each trial was the number randomised minus any participants whose outcomes were known to be missing.
Assessment of heterogeneity
We assessed statistical heterogeneity in each meta‐analysis using the T², I² and Chi² statistics. We regarded heterogeneity as substantial if T² is greater than zero and either I² is greater than 30% or there is a low P value (less than 0.10) in the Chi² test for heterogeneity.
Assessment of reporting biases
If there were 10 or more studies in the meta‐analysis, we planned to investigate reporting biases (such as publication bias) using funnel plots. We would have assessed funnel plot asymmetry visually, and used formal tests for funnel plot asymmetry. For continuous outcomes, we would have used the test proposed by Egger 1997, and for dichotomous outcomes, we planned to use the test proposed by Harbord 2006. If we had detected asymmetry in any of these tests or by a visual assessment, we would have performed exploratory analyses to investigate it.
Data synthesis
We carried out statistical analysis using the Review Manager software (RevMan 2011). We planned to use fixed‐effect meta‐analysis for combining data where it was reasonable to assume that studies were estimating the same underlying treatment effect: i.e. where trials are examining the same intervention, and the trials’ populations and methods were judged sufficiently similar. Where there was clinical heterogeneity sufficient to expect that the underlying treatment effects differed between trials, or if substantial statistical heterogeneity was detected, we used random‐effects meta‐analysis to produce an overall summary if an average treatment effect across trials was considered clinically meaningful. The random‐effects summary was treated as the average range of possible treatment effects and we discussed the clinical implications of treatment effects differing between trials. If the average treatment effect was not clinically meaningful, we did not combine trials.
Using random‐effects analyses, the results were presented as the average treatment effect with 95% confidence intervals, and the estimates of T² and I².
Subgroup analysis and investigation of heterogeneity
If we had identified substantial heterogeneity, we would have investigated it using subgroup analyses and sensitivity analyses. We would have considered whether an overall summary was meaningful, and if it was, we would have used random‐effects analysis to produce it.
We planned to carry out the following subgroup analyses.
Recurrent miscarriage versus sporadic miscarriage.
Early versus late miscarriage.
Pre‐existing psychological condition versus no psychological condition.
We planned to use the following outcome in subgroup analysis.
Psychological well being.
For fixed‐effect meta‐analyses, we planned to conduct subgroup analyses classifying whole trials by interaction tests as described by Deeks 2001. For random‐effects and fixed‐effect meta‐analyses using methods other than inverse variance, we intended to assess differences between subgroups by inspection of the subgroups’ confidence intervals; non‐overlapping confidence intervals indicate a statistically significant difference in treatment effect between the subgroups.
Sensitivity analysis
We planned to carried out sensitivity analyses to explore the effect of trial quality separating using the 'Risk of bias' table to distinguish high‐quality from low‐quality trials, for example, in allocation concealment and blinding of outcome assessors.
Results
Description of studies
See Characteristics of included studies; Characteristics of excluded studies.
Results of the search
Nineteen papers were identified in the search which covered psychological support for women who have had a miscarriage up to 23 weeks' gestation. We included six studies involving 1001 women (Adolfsson 2006; Lee 1996; Lok Hung 2006; Nikčević 2007; Swanson 1999; Swanson 2009). We excluded the remaining 13 papers as they were either not randomised controlled trials or were not within gestation limits. Some excluded trials did not provide interventions (seeCharacteristics of excluded studies).
Risk of bias in included studies
Overall, the quality of the studies was moderate to good. Some studies were unclear regarding blinding. SeeFigure 1; 'Risk of bias' summary and Figure 2 'Risk of bias' graph and Characteristics of included studies.
1.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Sequence generation
Randomisation was adequate in all studies. We contacted one author to confirm that randomisation was by an independent person pulling one of four cards blindly from a box (Swanson 1999).
Allocation concealment
This was low risk in the majority of studies and clear in only one study where allocation concealment was described in personal correspondence from the author (Swanson 1999).
Blinding
Following personal communication, blinding was considered adequate in one study (Adolfsson 2006) and for the remainder it was not clear that the participants, clinicians or outcome assessors were blinded. Because of the nature of the interventions, blinding was not considered crucial for the participants or clinicians.
Incomplete outcome data
Loss to follow‐up, withdrawals and exclusions after randomisation were not excessive and explained in all studies. An intention‐to‐treat analysis was performed in one study (Lok Hung 2006).
Selective outcome reporting
We were only able to access one study protocol to be assured that there was no selective outcome reporting (Lok Hung 2006). One study reported that two subscales measured were dropped from the analysis because they were confounded by alterations due to the women's pregnancy loss (Swanson 1999).
Other potential sources of bias
The participants in all studies were similar at baseline except for percentage of women with children (Lee 1996) and history of infertility (Lok Hung 2006) and were judged by the review authors to be at low risk of bias for this issue. As far as could be ascertained, no studies were stopped early for any reason.
Effects of interventions
1. One counselling session versus no counselling (three studies 236 women) (Analysis 1.1)
Primary outcomes
Psychological well being
This analysis included three studies with 236 women and compared one counselling session with no counselling (Adolfsson 2006; Lee 1996; Nikčević 2007). The counselling sessions were based on recognised counselling techniques and lasted 50 minutes (Nikčević 2007) or one hour (Adolfsson 2006; Lee 1996). All three studies used a number of measures to assess psychological well being at four months after miscarriage (Analysis 1.1).
1.1. Analysis.

Comparison 1 One counselling session versus no counselling (at four months), Outcome 1 Psychological well being.
For the purpose of analysis, components of the tools used to measure psychological well being are displayed separately. Two studies used the Hospital Anxiety and Depression (HADs) scale (Lee 1996; Nikčević 2007). Both studies recognised greater than 11 as the threshold for 'caseness' with HADs. When compared with no counselling, one counselling session did not result in a statistically significant reduction in anxiety with the standardised mean difference (SMD) ‐0.24 (95% confidence interval (CI) ‐0.62 to 0.15) (Analysis 1.1.1) or depression SMD ‐0.25 (95% CI ‐0.63 to 0.14) (Analysis 1.1.2).
When combined, grief as measured on the modified Texas Grief Inventory (Nikčević 2007) and the Perinatal Grief Scale (Swedish version) (Adolfsson 2006) showed no statistically significant reduction in grief in the counselling group (SMD ‐0.12; 95% CI ‐0.43 to 0.20) (Analysis 1.1.3).
In addition to HADs, Lee 1996 employed the Impact of Events scale and neither of the two components measured were statistically significantly reduced in the counselling group for avoidance (SMD 0.18; 95% CI ‐0.45 to 0.81) (Analysis 1.1.4) and intrusion (SMD ‐0.42; 95% CI ‐1.06 to 0.22) (Analysis 1.1.5). The Perinatal grief Scale (Adolfsson 2006) measured difficulty in coping (SMD ‐0.08; 95% CI ‐0.50 to 0.34) (Analysis 1.1.6) as well as grief (see above) and despair (SMD 0.01; 95% CI ‐0.41 to 0.43) (Analysis 1.1.7). Neither component was statistically significantly reduced by one‐hour counselling. In addition to HADs, Nikčević 2007 used the Texas Grief Inventory which measured grief (see above), self‐blame (SMD 0.03; 95% CI ‐0.45 to 0.51) (Analysis 1.1.8) and worry (SMD ‐0.42; 95%CI ‐0.91 to 0.06) (Analysis 1.1.9). Neither analysis showed statistically significant reduction in self‐blame or worry as a result of one 50‐minute counselling session.
The other primary outcome of patient satisfaction was not assessed in any of the studies.
Secondary outcomes
The other prespecified secondary outcomes were not assessed.
2. Three one‐hour counselling sessions versus no counselling (at four months) (one study 242 women) (Analysis 2.1)
Primary outcomes
Psychological well being
One study compared three one‐hour counselling sessions with no counselling based on a technique devised by the main author of the study (Swanson 1999). The sessions were conducted at one, five and 11 weeks. A Solomon four group randomised design was used in this study. Instead of omitting the pretest in two of the four groups, as recommended by Solomon, the study authors delayed it. This modification was justified by the study author to reduce the risk of early focused attention on loss serving as a form of treatment.
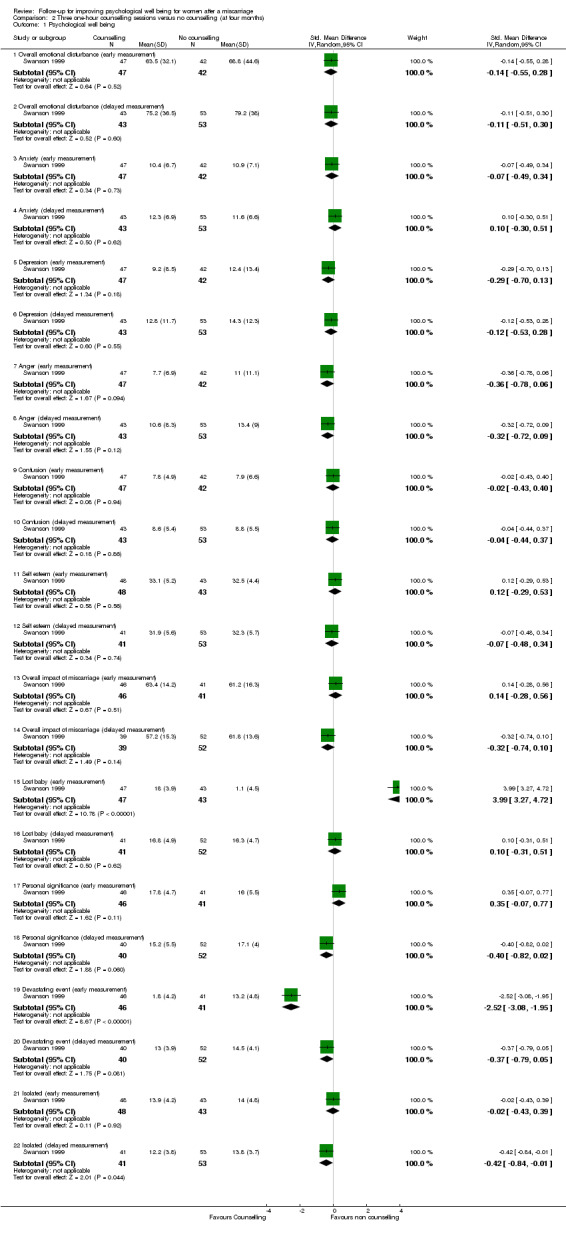
Outcome measures comprised self‐esteem measured on the 10‐item Rosenberg scale. Mood states were measured by the Profile of Mood States (POMS) as 'overall mood disturbance' and six subscales of anxiety‐tension, depression‐dejection, anger‐hostility, vigour‐fatigue, confusion‐bewilderment. The outcome measures of vigour‐fatigue were omitted by the author. In addition, the Impact of Miscarriage Scale (IMS) was developed by the author to measure 'overall impact of miscarriage' and four subscales of 'devastating event', 'lost baby' (this refers to whether the woman views the loss as a fetus or a baby), 'personal significance' and 'feeling isolated'.
Of the scores on any of the three scales and eight subscales of all outcome measures (early and delayed measure) (22 in total), only three showed statistical significance for any intervention, either early or delayed at four months. The subscales which identified a significant result were in the measurement tool developed by Swanson 1999. These were Lost baby (early measure) which showed that those women who did not have counselling had improved psychological well being than those who had counselling (SMD 3.99; 95% CI 3.27 to 4.72) (Analysis 2.1.15) (P = 0.00001). However, those women who undertook counselling (early measure) were statistically significantly less likely to view the miscarriage as a Devastating event (SMD ‐2.52; 95% CI ‐3.08 to ‐1.95) (Analysis 2.1.19) (P = 0.00001). Women who undertook counselling (delayed measure) stated that they felt less isolated than women who did not (SMD ‐0.42; 95%CI ‐0.84 to ‐0.01) (Analysis 2.1.22) (P = 0.04). Only two of the three statistically significant results favour counselling. All three significant results were from subscales of the instrument developed by the author (IMS).
2.1. Analysis.
Comparison 2 Three one‐hour counselling sessions versus no counselling (at four months), Outcome 1 Psychological well being.
Although another study used three counselling sessions as one of the interventions measured at three and five months, data were not available for this analysis despite contact with the author (Swanson 2009).
Patient satisfaction was not assessed in this study.
Secondary outcomes
The other prespecified secondary outcomes were not assessed.
3. Three one‐hour counselling sessions versus no counselling (at 12 months) (one study 242 women) (Analysis 3.1)
One study compared three one‐hour counselling sessions with no counselling based on a technique devised by the main author of the study (Swanson 1999). The sessions were conducted at one, five and 11 weeks. To counter the potential effect of data gathering unwittingly producing a beneficial effect Solomon four group randomised design was implemented where measurements were delayed on half of the treated and half of the control group. Outcome measures comprised self‐esteem measured on the 10‐item Rosenberg scale. Mood states were measured by the POMS as 'overall mood disturbance' and six subscales of anxiety‐tension, depression‐dejection, anger‐hostility, vigour‐fatigue, confusion‐bewilderment. The outcome measures of vigour‐fatigue were omitted by the author. In addition, the IMS was developed by the author to measure 'overall impact of miscarriage' and four subscales of 'devastating event', 'lost baby', 'personal significance' and 'feeling isolated'.
Of the scores on any of the three scales and eight subscales of all outcome measures (early and delayed measure) (22 in total), only three showed statistical significance for any intervention, either early or delayed at four months. The subscales which measured a significant result were in the measurement tool (IMS) developed by Swanson 1999. At 12 months, the overall impact of miscarriage (delayed measurement) (SMD ‐0.43; 95% CI ‐0.85 to ‐0.01) showed a statistically significant effect (P = 0.05) (Analysis 3.1.14) towards three one‐hour counselling sessions compared with no counselling, Lost baby (delayed measurement) showed a statistically significant effect (SMD 2.15; 95% CI 1.48 to 2.82) (Analysis 3.1.16) for no counselling compared with three one‐hour counselling sessions. Personal significance (delayed measurement) (SMD ‐0.66; 95% CI ‐1.09 to ‐0.24) (Analysis 3.1.18) and devastating event (delayed measurement) showed a statistically significant effect (SMD ‐0.45; 95% CI ‐0.87 to ‐0.04) (Analysis 3.1.20) towards three one‐hour counselling sessions compared with no counselling. Three of the four significant results favoured counselling over no counselling. All the significant results were from a subscale of an instrument developed by the author (IMS). Significant findings at 12 months differed in that the subscale of isolation at four months was replaced by that of personal significance at 12 months.
3.1. Analysis.

Comparison 3 Three one‐hour counselling sessions versus no counselling (at 12 months), Outcome 1 Psychological well being.
Although another study used three counselling sessions as one of the interventions measured at 12 months, data were not available for this analysis despite contact with the author (Swanson 2009).
Secondary outcomes
The other prespecified secondary outcomes were not assessed.
4. Two counselling sessions versus no counselling (one study 280 women) (Analysis 4.1)
Primary outcomes
Psychological well being
One study compared two nurse‐led counselling sessions with no counselling (Lok Hung 2006). The first session was 60 minutes face‐to‐face counselling by a nurse counsellor before discharge. The second session was 30 minutes telephone counselling two weeks after discharge. Outcome measures were the 12‐item General Health Questionnaire (GHQ‐12) (caseness greater than four), the Beck Depression Inventory (BDI) (caseness greater than12) and the Dyadic Adjustment Scale (DAS) completed at six weeks, three months and six months after miscarriage.
Medians were used to express data in this study and we were unable to extract the means or obtain them despite attempts to contact the author, therefore, the results are in narrative form.
At six weeks post‐miscarriage 56/132 (33.3%) women scored at least four on GHQ (median three, interquartile range (IQR) zero to six) in the counselling group compared with 60/136 (44.1%) (median three, IQR zero to seven) in the no‐counselling group. Thirty‐three women/132 (25%) scored at least 12 on BDI (median four, IQR two to 12) in the counselling group compared with 41/136 (30.1%) (median seven, IQR two to 13) in the no‐counselling group. No significant differences were found between the counselling and control groups using an intention‐to‐treat analysis.
At three months post‐miscarriage 32/132 (24.2%) women scored at least four on GHQ (median one, IQR 0 to three) in the counselling group compared with 42/136 (30.9%) (median one, IQR 0 to 4.75) in the no‐counselling group. Twenty‐four/132 (18.2%) scored at least 12 on BDI (median three, IQR 0 to seven) in the counselling group compared with 27/136 (19.9%) (median four, IQR one to 10) in the no‐counselling group. No significant differences were found between the counselling and control groups using an intention‐to‐treat analysis.
At six months post‐miscarriage, 30/132 (22.7%) women scored at least four on GHQ (median 0, IQR zero to three) in the counselling group compared with 27/136 (19.9%) (median one, IQR zero to three) in the no‐counselling group. Twenty women/132 (15.2%) scored at least 12 on BDI (median two, IQR zero to seven) in the counselling group compared with 23/136 (16.9%) (median seven, IQR zero to 8.75) in the no‐counselling group. No significant differences were found between the counselling and control groups using an intention‐to‐treat analysis.
Patient satisfaction was not assessed in this study.
Secondary outcomes
The other prespecified secondary outcomes were not assessed.
5. Combined caring (CC) Nurse caring (NC), self caring (SC) and no treatment (NT) (one study 341 women)
One study compared four interventions based on a counselling technique, videos and a workbook devised by the author (Swanson 2009). The comparisons were combined care (CC) comprising one counselling session by nurse counsellors based on the author's post‐miscarriage counselling model, three 18‐minute videos of the author coaching couples on ways to practice self and partner caring, plus one workbook; nurse caring (NC) comprising three one‐hour counselling sessions; self‐care (SC) comprising three videos plus workbook; and no treatment (NT) (Swanson 2009).
Primary outcomes were measured as depression (CES‐D). Women scoring 16 were associated with a higher risk of clinical depression. The secondary outcome of grief was measured by two subscales of the Miscarriage Grief Inventory; (MGI) pure grief (PG) and grief‐related emotions (GRE) which is adapted from the Texas Grief Inventory (TGI).
Women in all three treatment groups showed a faster rate of recovery from depression (CES‐D) compared with women receiving no treatment. However, only three one‐hour counselling sessions (NC) met the author's criterion for substantial evidence favouring NC over SC, CC and no treatment for accelerating resolution of depression (Bayesian Odds Ratio 7.9 median ‐0.7 P = 0.89).
Relative to no treatment there was, according to the author, substantial evidence that all three interventions (NC, SC, CC) hastened women's resolution of pure grief (PG) (Bayesian odds ratio 3.1 median ‐0.2 P = 0.76). The evidence favoured the impact of SC in hastening women's resolution of GRE (Bayesian odds ratio 3.2 median ‐0.2 P = 0.76).
According to Swanson 2009, there was no substantial evidence that no treatment was preferable to NC, SC or CC in accelerating women's resolution of pure grief, grief‐related emotion or depression.
Patient satisfaction was not assessed in this study.
Secondary outcomes
The other prespecified secondary outcomes were not assessed.
Discussion
Summary of main results
There is an assumption that miscarriage is an adverse event distressing all affected women to a greater or lesser degree. Until now the extent to which psychological follow‐up is necessary to reverse this state has not been examined in a Cochrane systematic review.
Given the international nature of systematic reviews, the WHO definition of miscarriage was used with the limit of 23 weeks' gestation in contrast to the UK definition of 24 weeks' gestation (RCOG 2006). It is possible that a very small number of women were between 23 and 24 weeks' gestation in one study (Lok Hung 2006) although this was calculated as unlikely by the review authors, although two other studies (Neugebauer 2006; Rajan 1993) were sufficiently at risk of including women up to 28 weeks that they were excluded. Planned sensitivity analyses were not possible as no studies examined recurrent miscarriages as a specific event, differentiated between early and late miscarriages or between women with a pre‐existing psychological condition and those without.
The interventions following miscarriage mainly consisted of one or a number of counselling sessions using recognised counselling techniques. Timing of the interventions varied from one week following miscarriage (Swanson 1999; Swanson 2009), up to 11 weeks (Swanson 1999; Swanson 2009). It was not possible to compare different types of psychological follow‐up via a meta‐analysis given the heterogeneity between studies.
In all studies the interventions were delivered by different professional groups including a midwife (Adolfsson 2006), psychologists (Lee 1996; Nikčević 2007) and nurses (Lok Hung 2006; Swanson 1999; Swanson 2009), which may have had an impact on the way in which the intervention was delivered. No study compared professionals delivering the intervention.
The time span of the studies covered more than a decade and so it is possible that psychological interventions may have changed during that period.
The major primary outcome was psychological well being. We were unable to report the majority of the studies as meta‐analyses but were able to report them as forest plots with narrative.
Under the primary outcome of psychological well being, a wide range of outcomes were measured from those more commonly anticipated such as grief, anxiety and depression to emotional disturbance, self‐esteem and isolation. Outcome measures used included validated tools, some of which had been modified, for example, a Swedish version of the Perinatal grief Scale (Adolfsson 2006) and others which had been developed by the study authors (Impact of Miscarriage Scale Swanson 1999) (Miscarriage Grief Inventory Swanson 2009). The tools also varied in that some were generic such as the Hospital Anxiety and Depression Scale (Lee 1996; Nikčević 2007) and others were miscarriage specific (Swanson 1999; Swanson 2009). Caseness, or the level at which women were judged to benefit from psychological follow‐up using a specific tool, was not made clear in all studies. Some studies did not state whether a high score indicated psychological ill health or well being (Nikčević 2007; Swanson 2009). All of these issues made it challenging to pool the results and compare findings.
Timing of outcome measurements differed markedly between studies from one month (Lok Hung 2006) to 12 months (Swanson 1999) highlighting the uncertainty surrounding the rate of psychological recovery following miscarriage. One study noted that anxiety, depression and grief reduced significantly in all three groups with time (Nikčević 2007). Psychological well being was measured and improved with time which may or may not have been influenced by the intervention in four other studies (Lee 1996; Lok Hung 2006; Swanson 1999; Swanson 2009).
The possibility that the measurement of grief, depression and other associated symptoms act as part of the healing process by allowing the woman to talk about her feelings was explored in one study. The author attempted to manage this possibility by organising early or delayed measurement, but this did not make a difference to the overall results (Swanson 1999).
Generally the studies have shown that women's reactions to miscarriage vary and the extent of depression, grief and anxiety differ. Only one study showed some significant outcomes. However, they were unlikely to be of significance overall as they represented differences between delayed and early measures as well as individual subscales on a complex tool developed by the study author (Swanson 2009). No significant results were found in this study on the widely used, standardised scales.
Three studies, two of which were combined in a forest plot, measured the generic outcomes of anxiety, depression and grief. although the results favoured counselling none were significant. The other primary outcome of patient satisfaction was not measured in any of the trials. We maintain that this is an important outcome as evidence of satisfaction alone is not a reason to provide a service. In addition, none of the secondary outcomes identified by the review authors as important were reported. They included adverse reaction to follow‐up, referral to primary healthcare services, admission to hospital and costs associated with follow‐up. It is possible that an adverse reaction, referral or admission to hospital following psychological follow‐up is unlikely and therefore these outcomes may not be a priority outcome measure for primary studies.
Overall completeness and applicability of evidence
Our published protocol described our plan to analyse a series of major and minor outcomes. We were able to analyse one of the primary outcomes but none of the secondary outcomes were included in any studies. All eligible randomised controlled trials were included up to April 2011. The majority of studies lacked power. The two larger studies (Swanson 1999; Swanson 2009) included such a complex combination of interventions and outcome measures that any potentially significant effects may have been diluted.
Quality of the evidence
This review examined psychological follow‐up for 1001 women after miscarriage in six randomised controlled trials. The studies were single centre, from a range of countries, over a decade and a half. Overall, the risk of bias was judged to be low, although allocation concealment and blinding was unclear as it was not stated in the majority of studies. It was recognised that given the nature of the trials, blinding of the participants and clinicians would not be possible.
Potential biases in the review process
There are a number of limitations to this review. Suprisingly, most of the studies published in the last decade did not have a published protocol and to our knowledge, had not registered their study in one of the many trial registries, indicating that a broad search strategy was still necessary. Lay organisations providing psychological follow‐up were included in the search strategy, but none were found.
Strengths of this review include the methodological rigour applied, including a published protocol, data analysis and narrative, which allowed us to make the findings explicit.
Agreements and disagreements with other studies or reviews
A Cochrane review on perinatal death (Flenady 2008), has indicated that there is insufficient evidence to show that psychological follow‐up improves the well being of women following perinatal death. Similarly, this review has found a lack of evidence to show that psychological follow‐up is beneficial for women following miscarriage. However, some women may benefit from psychological follow‐up and the review authors recommend that any service already in place should continue taking into account women's preference pending further evidence.
Authors' conclusions
Implications for practice.
Evidence is insufficient to demonstrate the superiority of either psychological support such as counselling or no intervention post‐miscarriage. Given the equivocal evidence, women's preference should play a large role in the decision‐making process.
Implications for research.
Further evaluation of the effectiveness of psychological follow‐up for women following miscarriage should be based on good quality, adequately‐powered randomised trials. Future trials should use standardised interventions, standardised outcome measures at specified time points.
Women's satisfaction with psychological follow‐up should be explored in future studies. Given the costs of these interventions, the economic implications for this service should also be integrated into any future study.
Acknowledgements
All authors would like to acknowledge Swansea University and the University of Glamorgan for allowing them the time to undertake the protocol and the full review.
As part of the pre‐publication editorial process, this review has been commented on by three peers (an editor and two referees who are external to the editorial team) and the Group's Statistical Adviser.
Data and analyses
Comparison 1. One counselling session versus no counselling (at four months).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Psychological well being | 3 | Std. Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 1.1 Anxiety | 2 | 105 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.24 [‐0.62, 0.15] |
| 1.2 Depression | 2 | 105 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.25 [‐0.63, 0.14] |
| 1.3 Grief | 2 | 154 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.12 [‐0.43, 0.20] |
| 1.4 Avoidance | 1 | 39 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.18 [‐0.45, 0.81] |
| 1.5 Intrusion | 1 | 39 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.42 [‐1.06, 0.22] |
| 1.6 Difficulty in coping | 1 | 88 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.08 [‐0.50, 0.34] |
| 1.7 Despair | 1 | 88 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.01 [‐0.41, 0.43] |
| 1.8 Self blame | 1 | 66 | Std. Mean Difference (IV, Fixed, 95% CI) | 0.03 [‐0.45, 0.51] |
| 1.9 Worry | 1 | 66 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.42 [‐0.91, 0.06] |
Comparison 2. Three one‐hour counselling sessions versus no counselling (at four months).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Psychological well being | 1 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Overall emotional disturbance (early measurement) | 1 | 89 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.14 [‐0.55, 0.28] |
| 1.2 Overall emotional disturbance (delayed measurement) | 1 | 96 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.11 [‐0.51, 0.30] |
| 1.3 Anxiety (early measurement) | 1 | 89 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.49, 0.34] |
| 1.4 Anxiety (delayed measurement) | 1 | 96 | Std. Mean Difference (IV, Random, 95% CI) | 0.10 [‐0.30, 0.51] |
| 1.5 Depression (early measurement) | 1 | 89 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.29 [‐0.70, 0.13] |
| 1.6 Depression (delayed measurement) | 1 | 96 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.12 [‐0.53, 0.28] |
| 1.7 Anger (early measurement) | 1 | 89 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.36 [‐0.78, 0.06] |
| 1.8 Anger (delayed measurement) | 1 | 96 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.32 [‐0.72, 0.09] |
| 1.9 Confusion (early measurement) | 1 | 89 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.43, 0.40] |
| 1.10 Confusion (delayed measurement) | 1 | 96 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.04 [‐0.44, 0.37] |
| 1.11 Self esteem (early measurement) | 1 | 91 | Std. Mean Difference (IV, Random, 95% CI) | 0.12 [‐0.29, 0.53] |
| 1.12 Self esteem (delayed measurement) | 1 | 94 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.07 [‐0.48, 0.34] |
| 1.13 Overall impact of miscarriage (early measurement) | 1 | 87 | Std. Mean Difference (IV, Random, 95% CI) | 0.14 [‐0.28, 0.56] |
| 1.14 Overall impact of miscarriage (delayed measurement) | 1 | 91 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.32 [‐0.74, 0.10] |
| 1.15 Lost baby (early measurement) | 1 | 90 | Std. Mean Difference (IV, Random, 95% CI) | 3.99 [3.27, 4.72] |
| 1.16 Lost baby (delayed measurement) | 1 | 93 | Std. Mean Difference (IV, Random, 95% CI) | 0.10 [‐0.31, 0.51] |
| 1.17 Personal significance (early measurement) | 1 | 87 | Std. Mean Difference (IV, Random, 95% CI) | 0.35 [‐0.07, 0.77] |
| 1.18 Personal significance (delayed measurement) | 1 | 92 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.40 [‐0.82, 0.02] |
| 1.19 Devastating event (early measurement) | 1 | 87 | Std. Mean Difference (IV, Random, 95% CI) | ‐2.52 [‐3.08, ‐1.95] |
| 1.20 Devastating event (delayed measurement) | 1 | 92 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.37 [‐0.79, 0.05] |
| 1.21 Isolated (early measurement) | 1 | 91 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.43, 0.39] |
| 1.22 Isolated (delayed measurement) | 1 | 94 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.42 [‐0.84, ‐0.01] |
Comparison 3. Three one‐hour counselling sessions versus no counselling (at 12 months).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Psychological well being | 1 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Emotional disturbance (early measurement) | 1 | 89 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐0.51, 0.32] |
| 1.2 Emotional disturbance (delayed measurement) | 1 | 96 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.14 [‐0.54, 0.27] |
| 1.3 Anxiety (early measurement) | 1 | 89 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.03 [‐0.45, 0.39] |
| 1.4 Anxiety (delayed measurement) | 1 | 96 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.15 [‐0.56, 0.25] |
| 1.5 Depression (early measurement) | 1 | 89 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.26 [‐0.68, 0.16] |
| 1.6 Depression (delayed measurement) | 1 | 96 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.57, 0.23] |
| 1.7 Anger (early measurement) | 1 | 89 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.17 [‐0.59, 0.25] |
| 1.8 Anger (delayed measurement) | 1 | 96 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.15 [‐0.56, 0.25] |
| 1.9 Confusion (early treatment) | 1 | 89 | Std. Mean Difference (IV, Random, 95% CI) | 0.04 [‐0.38, 0.46] |
| 1.10 Confusion (delayed measurement) | 1 | 96 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.08 [‐0.48, 0.32] |
| 1.11 Self esteem (early measurement) | 1 | 91 | Std. Mean Difference (IV, Random, 95% CI) | 0.13 [‐0.29, 0.54] |
| 1.12 Self esteem (delayed measurement) | 1 | 94 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.54, 0.28] |
| 1.13 Impact of miscarriage (early measurement) | 1 | 87 | Std. Mean Difference (IV, Random, 95% CI) | 0.12 [‐0.30, 0.54] |
| 1.14 Impact of miscarriage (delayed measurement) | 1 | 91 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.43 [‐0.85, ‐0.01] |
| 1.15 Lost baby (early measurement) | 1 | 90 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [‐0.41, 0.41] |
| 1.16 Lost baby (delayed measurement) | 1 | 68 | Std. Mean Difference (IV, Random, 95% CI) | 2.15 [1.48, 2.82] |
| 1.17 Personal significance (early measurement) | 1 | 87 | Std. Mean Difference (IV, Random, 95% CI) | 0.18 [‐0.24, 0.60] |
| 1.18 Personal significance (delayed measurement) | 1 | 92 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.66 [‐1.09, ‐0.24] |
| 1.19 Devastating event (early measurement) | 1 | 87 | Std. Mean Difference (IV, Random, 95% CI) | 0.20 [‐0.22, 0.63] |
| 1.20 Devastating event (delayed measurement) | 1 | 92 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.45 [‐0.87, ‐0.04] |
| 1.21 Isolated (early measurement) | 1 | 91 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.50, 0.33] |
| 1.22 Isolated (delayed measurement) | 1 | 94 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.36 [‐0.77, 0.06] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Adolfsson 2006.
| Methods | Randomised controlled trial. | |
| Participants | Women who had experienced complete, incomplete or missed early miscarriage before 13 weeks' gestation. Inclusion criteria Visit to gynaecologic outpatient clinic to diagnose miscarriage before 13 weeks' gestation. Over 18 years of age. Swedish speaking. N = 116 commenced the study, 88 completed. Excluson criteria Pregnancy kept secret from next of kin. Extrauterine or suspicion of extrauterine pregnancy. |
|
| Interventions |
Intervention group 1: a structured conversation with 1 midwife for 60 minutes focusing on the woman's experience of miscarriage and taking her through the process of Swanson's caring science theory.
N = 43. Comparison group 2: met 1 of 5 midwives during a 30‐minute visit who asked about their general health and any complications. At this visit the midwife did not ask about the woman's feelings and emotions. N = 45. |
|
| Outcomes | Reduction of women's grief as measured at 1 and 4 months post‐miscarriage by:
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was performed in blocks of 10. |
| Allocation concealment (selection bias) | Unclear risk | Sealed envelopes, not stated as opaque. |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Clinicians and outcomes assessors blinded. Participants not blinded but asked not to discuss their care during the study with other participants (personal communication with the author). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Of the 116 included in the study, 28 did not complete either the first questionnaire or the second questionnaire. |
| Selective reporting (reporting bias) | Low risk | Reports all pre‐specified outcomes but we have not accessed the trial protocol. |
| Groups similar at baseline? | Low risk | For age, gestational length, children, haemorrhage. |
| Free from early stopping? | Low risk | There was no statement indicating that the study was stopped early. |
Lee 1996.
| Methods | Randomised controlled trial. | |
| Participants | Women who had experienced a miscarriage up to 19 weeks' gestation. Inclusion criteria Pregnancy of 6 to 19 weeks at the time of miscarriage. No previous miscarriage. Aged 18 years or over. Able to speak and read English fluently. Had wanted pregnancy to continue. Were not under psychological or psychiatric care or taking psychoactive drugs at the time of miscarriage. N = 40. Exclusion criteria Those who had intended to terminate the pregnancy. |
|
| Interventions |
Intervention group 1: 1‐hour long psychological debriefing by a female psychologist in their own home 2 weeks post‐miscarriage.
N = 21 Comparison group 2: no intervention. N = 18 |
|
| Outcomes | Emotional adaptation measured at 4 months post‐miscarriage by:
Questionnaires sent by post 2 days and 4 months post‐miscarriage to all participants. |
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | 'Women were randomly allocated to Group 1 or Group 2.' |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Participants, clinicians and outcomes assessors not stated as blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 7 women did not return questionnaire and were excluded from the study. 14 indicated that they did not wish to have a follow‐up appointment and were excluded from the data analysis. |
| Selective reporting (reporting bias) | Low risk | Reports all pre‐specified outcomes but we were not able to access the trial protocol. |
| Groups similar at baseline? | Low risk | 'There were no significant differences between groups on any measures taken at phase 1, except that the percentage of women with children in group 1 (38%) was significantly lower than that of women in group 2 (77.8%).' |
| Free from early stopping? | Low risk | There was no statement indicating that the study was stopped early. |
Lok Hung 2006.
| Methods | Randomised controlled trial. | |
| Participants | Women who had experienced a miscarriage up to 24 weeks' gestation (see notes). Inclusion criteria Miscarriage before 24 weeks. N = 280 (12 withdrew after randomisation). Exclusion criteria Patients who were unwilling to participate, with actively treated psychiatric disease, non‐Chinese, visitors to Hong Kong. |
|
| Interventions |
Intervention group 1
A 1‐hour counselling session by a nurse following baseline questionnaire while in hospital and a second 30‐minute telephone counselling session 2 weeks later.
N = 132. Control group 2 'Routine clinical practice and attended by the clinical staff as usual. No specific counselling or follow‐up care was arranged.' N = 136. |
|
| Outcomes | Assessment of the proportion of women with psychological morbidity after miscarriage at baseline, 6 weeks, 3 and 6 months measured by:
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | 'Randomised using a set of sealed, opaque, sequentially numbered envelopes, each containing a computer‐generated random number denoting the randomisation result.' |
| Allocation concealment (selection bias) | Low risk | 'sealed, opaque, sequentially numbered envelopes, each containing a computer‐generated random number denoting the randomisation result.' |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Participants, clinicians and outcomes assessors not stated as blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | At 6 weeks there were 96 in the intervention group and 99 in the control group, at 3 months 105 and 115 and at 6 months 104 and 110 respectively. An intention‐to‐treat analysis was performed. |
| Selective reporting (reporting bias) | Low risk | Reports all pre‐specified outcomes as we were able to access the trial protocol. |
| Groups similar at baseline? | Low risk | Similar for education, employment status, previous miscarriage, planned, wanted pregnancy, miscarriage symptoms, management of miscarriage. 314 women in the control group had a history of infertility compared to 187 in the counselling group. |
| Free from early stopping? | Low risk | There was no statement indicating that the study was stopped early. |
Nikčević 2007.
| Methods | Randomised controlled trial. | |
| Participants | Women found to have a missed miscarriage at 10 to 14 weeks' gestation.
Inclusion criteria
As above. N = 80 commenced the study, 66 completed. Exclusion criteria Women with a history of perinatal death. Elective termination for foetal abnormality. Recurrent miscarriage. Inability to speak and read English fluently. Those under psychological or psychiatric care. |
|
| Interventions |
Intervention group 1: 1 session of psychological counselling with a psychologist for 50 minutes 5 weeks after the miscarriage.
N = 39. Comparison group 2: no psychological counselling. N = 41. |
|
| Outcomes | Women's distress post‐miscarriage measured at 4, 7 and 16 weeks post‐miscarriage by:
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | 'randomly allocated'... 'on the basis of computer generated random number tables'. |
| Allocation concealment (selection bias) | Low risk | 'At the end of the medical consultation, the doctor opened a sealed envelope and accordingly invited the women allocated to the intervention group to stay for psychological counselling.' |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Participants, clinicians and outcomes assessors not stated as blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 14 women did not complete the second and third questionnaires; 2 women from the intervention group were excluded (1 had a second miscarriage during the study and 1 had psychological counselling arranged elsewhere). |
| Selective reporting (reporting bias) | Low risk | Reports all pre‐specified outcomes but we were not able to access the trial protocol. |
| Groups similar at baseline? | Low risk | For age, Caucasian, married, children, miscarriage history, planned pregnancy, cause. There was a difference in those with a university education between group 1 (16) and group 2 (10). |
| Free from early stopping? | Low risk | There was no statement indicating that the study was stopped early. |
Swanson 1999.
| Methods | Solomon 4 group randomised experimental design with repeated measures. | |
| Participants | Women who had experienced a miscarriage. Inclusion criteria At least 18 years of age. Miscarried at 20 weeks or less. Within 5 weeks of loss. Could speak and write English. N = 242. Exclusion criteria Not stated. |
|
| Interventions |
Intervention group 1: 1‐hour long counselling sessions following Swanson's middle‐range caring theory conducted by the principal investigator or a research associate at 1, 5 and 11 weeks after study entry with early measures.
N = 56.
Intervention group 2: 1‐hour long counselling sessions following Swanson's middle‐range caring theory conducted by the principal investigator or a research associate at 1, 5 and 11 weeks after study entry with delayed measures.
N = 60. Comparison group 3: no counselling with early measures. N = 64. Comparison group 4: no counselling with delayed measures. N = 62. |
|
| Outcomes | Women's integration of loss and emotional well‐being measured at enrolment, 6 weeks, 4 months and 1 year or 4 months and 1 year post‐miscarriage using the following questionnaires:
Intervention 1 and 2 were measured 'early' immediately after enrolling, at 6 weeks, 4 months and 1 year. Comparison 3 and 4 had 'delayed' measurement at 4 months and 1 year after enrolling. |
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The author was contacted and confirmed that randomisation was by an independent person pulling 1 of 4 cards blindly from a box. |
| Allocation concealment (selection bias) | Low risk | Women were randomly assigned via telephone by an independent person (correspondence with author). |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Participants, clinicians and outcomes assessors not stated as blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Intervention group 1 lost 10, intervention group 2 lost 16, comparison group 3 lost 21 and comparison group 4 lost 9 to follow‐up, 57 or 24% in total. |
| Selective reporting (reporting bias) | Unclear risk | We were not able to access the trial protocol, but vigour and fatigue subscales were dropped 'because they were confounded by alterations in women's physical health status due to the pregnancy‐related changes experienced by many women in the first year after loss'. |
| Groups similar at baseline? | Low risk | There were no significant differences between groups on any recruitment criteria or demographic variables. |
| Free from early stopping? | Low risk | There was no statement indicating that the study was stopped early. |
Swanson 2009.
| Methods | Randomised controlled clinical trial. | |
| Participants | Couples of which the woman had sustained a miscarriage before 20 weeks' gestation. Inclusion criteria Both agreed to participate. Reported unplanned, unexpected loss of pregnancy prior to 20 weeks' gestation. Could speak and write English. In a self‐proclaimed committed relationship. Geographically accessible. Within 3 months of loss. N = 341 women (682 in total). Exclusion criteria Unmarried people aged less than 18 years. |
|
| Interventions | Intervention 1: nurse caring (NC) (3 1‐hour counselling sessions in own home).
N = 77.
Intervention 2: self‐caring (SC) (3 videos of Swanson coaching couples and couples speaking of their miscarriage experiences and his and hers workbooks which stimulated reflection by asking 7 daily questions, data from which were not analysed).
N = 64.
Intervention 3: combined caring (CC) (1‐hour long counselling session plus 1 workbook given and 2 workbooks mailed).
N = 63.
Intervention 4: control (no treatment).
N = 79 (at 13 months). All 3 interventions were based on Swanson's caring theory and comprised: week 1 ‐ 'coming to know', week 5 ‐ 'sharing the loss', week 11 ‐ 'getting through it'. |
|
| Outcomes | Depression and grief measured at baseline, 3 months, 5 months and 13 months by:
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Cards shuffled and box shaken vigorously. |
| Allocation concealment (selection bias) | Low risk | Upon consent random allocation via 'a strict card pulling protocol' ... 'always involved two members of staff; 1 shuffled cards, vigorously shook the box and lifted the box above the card puller's eye level and the other who reached up and blindly pulled the card out of the box'. |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Participants, clinicians and outcomes assessors not stated as blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 341 couples randomised, 17 couples plus 3 women and 9 men subsequently returned no data. The final analysis comprised 318 couples. 1 woman in Intervention 1 attended no NC sessions, 8 women never used their SC materials and 2 women did not participate in the CC intervention 3. |
| Selective reporting (reporting bias) | Low risk | All pre‐specified outcomes appear to have been addressed, but we were not able to access the trial protocol. |
| Groups similar at baseline? | Low risk | 'There were no significant differences in baseline scores attributable to randomisation'. Measured for employment, history of depression, anxiety or grief, ethnicity/race, income, age and days since loss at baseline. |
| Free from early stopping? | Low risk | There was no statement indicating that the study was stopped early. |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Broen 2004 | Not RCT, follow‐up study with no intervention. |
| Broen 2005 | Not RCT, follow‐up study with no intervention. |
| Cordle 1994 | Not RCT, follow‐up study with no intervention. |
| Jacobs 2000 | Not RCT, qualitative evaluation of a follow‐up service. |
| Lefkof 2002 | Not RCT, a review article |
| Luise 2002 | Not RCT, observational study with no intervention. |
| Neugebauer 2006 | RCT, women up to 28 weeks' gestation. |
| Neugebauer 2007 | Not RCT, a preliminary open trial. |
| Nikčević 1998 | Not RCT, cross‐sectional study. |
| Nikčević 2003 | Not RCT, controlled intervention study. |
| Rajan 1993 | RCT, but no follow‐up on pregnancy loss. |
| Sejourne 2011 | Quasi‐RCT using alternation as means of randomisation. |
| Thaper 1992 | Not RCT, no intervention. |
RCT: randomised controlled trial
Differences between protocol and review
There are no differences between what was stated in the protocol and the content of the review.
Contributions of authors
All three authors chose the topic for the review. Fiona Murphy (FM) provided subject expertise and Allyson Lipp (AL) provided systematic review expertise. FM, AL and Diane L Powles (DP) jointly wrote the protocol.
All three authors separately assessed trials for inclusion and trial methodological quality. AL produced a first draft of the review and FM and DP contributed to data collection and analysis, as well as drafting the results and discussion.
Sources of support
Internal sources
-
Swansea University, UK.
Time to undertake the protocol
-
University of Glamorgan, UK.
Time to undertake the protocol
External sources
No sources of support supplied
Declarations of interest
None known.
New
References
References to studies included in this review
Adolfsson 2006 {published data only}
- Adolfsson A. The effect of structured second visit to midwifes in women with early miscarriages, a randomized study. 10th International Conference of Maternity Care Researchers; 2004 June 13‐16; Lund, Sweden. 2004:22. [CN‐00487510]
- Adolfsson A, Bertero C, Larsson PG. Effect of a structured follow‐up visit to a midwife on women with early miscarriage: a randomized study. Acta Obstetricia et Gynecologica Scandinavica 2006;85:330‐5. [DOI] [PubMed] [Google Scholar]
Lee 1996 {published data only}
- Lee C, Slade P, Lygo V. The influence of psychological debriefing on emotional adaptation in women following early miscarriage: a preliminary study. British Journal of Medical Psychology 1996;69(Pt 1):47‐58. [DOI] [PubMed] [Google Scholar]
Lok Hung 2006 {published and unpublished data}
- Lok IH. Psychological morbidity after miscarriage [thesis]. University of Hong Kong, 2006. [Google Scholar]
Nikčević 2007 {published data only}
- Nikčević AV, Kuczmierczyk AR, Nicolaides KH. The influence of medical and psychological interventions on women's distress after miscarriage. Journal of Psychosomatic Research 2007;63(3):283‐90. [DOI] [PubMed] [Google Scholar]
Swanson 1999 {published data only}
- Swanson KM. Effects of caring, measurement, and time on miscarriage impact and women's well‐being. Nursing Research 1999;48(6):288‐98. [DOI] [PubMed] [Google Scholar]
Swanson 2009 {published data only}
- Swanson KM, Chen HT, Graham CJ, Wojnar DM, Petras A. Resolution of depression and grief during the first year after miscarriage: a randomized controlled clinical trial of couples‐focused interventions. Journal of Women's Health 2009;18(8):1245‐57. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Broen 2004 {published data only}
- Broen AN, Moum TR, Bødtker AS, Ekeberg O. Psychological impact on women of miscarriage versus induced abortion: a 2‐year follow‐up study. Psychosomatic Medicine 2004;66(2):265‐71. [DOI] [PubMed] [Google Scholar]
Broen 2005 {published data only}
- Broen AN, Moum TR, Bødtker AS, Ekeberg O. The course of mental health after miscarriage and induced abortion: a longitudinal, five‐year follow‐up study. BMC Medicine 2005;3:265‐71. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cordle 1994 {published data only}
- Cordle CJ, Prettyman RJ. A 2‐year follow‐up of women who have experienced early miscarriage. Journal of Reproductive and Infant Psychology 1994;12:37‐43. [Google Scholar]
Jacobs 2000 {published data only}
- Jacobs J, Harvey J. Evaluation of an Australian miscarriage support programme. British Journal of Nursing 2000;9(1):22‐6. [DOI] [PubMed] [Google Scholar]
Lefkof 2002 {published data only}
- Lefkof J, Glazer G. Grief after miscarriage. Practical interventions can assist with far‐reaching loss. Advance for Nurse Practitioners 2002;10(10):79‐82. [PubMed] [Google Scholar]
Luise 2002 {published data only}
- Luise C, Jermy K, Collons WP, Bourne TH. Expectant management of incomplete, spontaneous first‐trimester miscarriage: outcome according to initial ultrasound criteria and value of follow‐up visits. Ultrasound In Obstetrics & Gynecology 2002;19(6):580‐2. [DOI] [PubMed] [Google Scholar]
Neugebauer 2006 {published data only}
- Neugebauer R, Kline J, Markowitz JC, Bleiberg KL, Baxi L, Rosing MA, et al. Pilot randomized controlled trial of interpersonal counselling for subsyndromal depression following miscarriage. Journal of Clinical Psychiatry 2006;67(8):1299‐304. [DOI] [PubMed] [Google Scholar]
Neugebauer 2007 {published data only}
- Neugebauer R, Kline J, Bleiberg K, Baxi L, Markowitz JC, Rosing M, et al. Preliminary open trial of interpersonal counselling for subsyndromal depression following miscarriage. Depression and Anxiety 2007;24(3):219‐22. [DOI] [PubMed] [Google Scholar]
Nikčević 1998 {published data only}
- Nikcevic AV, Tunkel SA, Nicolaides KH. Psychological outcomes following missed abortions and provision of follow‐up care. Ultrasound in Obstetrics and Gynecology 1998;11(2):123‐8. [DOI] [PubMed] [Google Scholar]
Nikčević 2003 {published data only}
- Nikcevic AV. Development and evaluation of a miscarriage follow up clinic. Journal of Reproductive & Infant Psychology 2003;21(3):207‐17. [Google Scholar]
Rajan 1993 {published data only}
- L Rajan A Oakley. No pills for heartache: The importance of social support for women who suffer pregnancy loss. Journal of Reproductive and Infant Psychology 1993;11:75‐87. [Google Scholar]
Sejourne 2011 {published data only}
- Sejourne N, Callahan S, Chabrol H. [The efficiency of a brief support intervention for anxiety, depression and stress after miscarriage]. [French]. Journal de Gynecologie, Obstetrique et Biologie de la Reproduction 2011;40(5):437‐43. [DOI] [PubMed] [Google Scholar]
Thaper 1992 {published data only}
- Thapar AK, Thapar A. Psychological sequelae of miscarriage: a controlled study using the General Health Questionnaire and the Hospital Anxiety and Depression scale. British Journal of General Practice 1992;42(356):94‐6. [PMC free article] [PubMed] [Google Scholar]
Additional references
Blohm 2008
- Blohm F, Friden B, Milsom I. A prospective longitudinal population‐based study of clinical miscarriage in an urban Swedish population. BJOG: An International Journal of Obstetrics & Gynaecology 2008;115(2):176‐83. [DOI] [PubMed] [Google Scholar]
Deeks 2001
- Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta‐analysis. In: Egger M, Davey Smith G, Altman DG editor(s). Systematic reviews in health care: meta‐analysis in context. London: BMJ Books, 2001. [Google Scholar]
Egger 1997
- Egger M, Smith GD, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;315:629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Farquharson 2005
- Farquharson RG, Jauniaux E, Exalto N. Updated and revised nomenclature for description of early pregnancy events. Human Reproduction 2005;20:3008‐11. [DOI] [PubMed] [Google Scholar]
Flenady 2008
- Flenady V, Wilson T. Support for mothers, fathers and families after perinatal death. Cochrane Database of Systematic Reviews 2008, Issue 1. [DOI: 10.1002/14651858.CD000452.pub2] [DOI] [PubMed] [Google Scholar]
Frost 2007
- Frost J, Bradley H, Levitas R, Smith L, Garcia J. The loss of possibility: scientisation of death and the special case of early miscarriage. Sociology of Health and Illness 2007;29(7):1003‐22. [DOI] [PubMed] [Google Scholar]
Harbord 2006
- Harbord RM, Egger M, Sterne JA. A modified test for small‐study effects in meta‐analyses of controlled trials with binary endpoints. Statistics in Medicine 2006;25:3443‐57. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Malacrida 1998
- Malacrida C. Mourning the dreams. Alberta Canada: Qual Institute Press, 1998. [Google Scholar]
Mander 1997
- Mander R. Perinatal grief: understanding the bereaved and their carers. In: Alexander J, Roth C, Levy V editor(s). Midwifery Practice. Basingstoke: Macmillan, 1997:29‐50. [Google Scholar]
Nanda 2006
- Nanda K, Peloggia A, Grimes DA, Lopez LM, Nanda G. Expectant care versus surgical treatment for miscarriage. Cochrane Database of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD003518.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Neilson 2010
- Neilson JP, Gyte GML, Hickey M, Vazquez JC, Dou L. Medical treatments for incomplete miscarriage (less than 24 weeks). Cochrane Database of Systematic Reviews 2010, Issue 1. [DOI: 10.1002/14651858.CD007223.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Neugebauer 1997
- Neugebauer R, Kline J, Shrout P, Skodol A, O’Connor P, Geller P, et al. Major depressive disorder in the 6 months after miscarriage. JAMA 1997;277(5):383‐8. [PubMed] [Google Scholar]
Nikcevic 1999
- Nikcevic A, Tunkel S, Kuczmierczyk A. Investigation of the cause of miscarriage and its influence on women’s psychological distress. British Journal of Obstetrics and Gynaecology 1999;106(8):808‐13. [DOI] [PubMed] [Google Scholar]
RCOG 2006
- RCOG. Management of Early Pregnancy Loss. London: Royal College of Obstetricians and Gynaecologists, 2006. [Google Scholar]
RevMan 2011 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011.
Stirtzinger 1999
- Stirtzinger RM, Robinson DE, Stewart DE, Ralevski E. Parameters of grieving in spontaneous abortion. International Journal of Psychiatry in Medicine 1999;29:235‐49. [DOI] [PubMed] [Google Scholar]
Stratton 2008
- Stratton K, Lloyd L. Hospital‐based interventions at and following miscarriage: literature to inform a research‐practice initiative. Australian and New Zealand Journal of Obstetrics and Gynaecology 2008;48:5‐11. [DOI] [PubMed] [Google Scholar]
Trinder 2006
- Trinder J, Brocklehurst P, Porter R, Read M, Vyas S, Smith L. Management of miscarriage: expectant, medical, or surgical? Results of randomised controlled trial (miscarriage treatment (MIST) trial). BMJ 2006;332:1235‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
WHO 2001
- WHO. Definitions and indicators in family planning, maternal & child health and reproductive health. WHO Regional Strategy on Sexual and Reproductive Health. Geneva: World Health Organization, 2001. [Google Scholar]