

Abstract
Background:
Stress is a common hazard in the work environment and is associated with multiple adverse health effects. The association between work-related stress (WRS) and cardiovascular disease has been established in a number of epidemiological studies.
Methods:
A systematic review was conducted according to the PRISMA statement of the English literature involving WRS and carotid artery intima media thickness (CIMT).
Results:
Four cohorts and six cross-sectional studies of occupational stress and CIMT were identified. All cohorts and five of the cross-sectional studies reported a significant positive association, while one reported an inverse association of WRS and CIMT.
Discussion:
The weight of the evidence that we were able to identify suggests that occupational stress results in an increased risk of atherosclerosis, assessed via CIMT. Studies that include longitudinal measures of stress and intermediate cardiac endpoints, with adequate accounting for confounders, are needed. Interventional studies should also be conducted to determine whether CIMT progression can be prevented with workplace stress reduction.
Keywords: Carotid artery intima media thickness, Cardiovascular disease, Atherosclerosis, Work-related stress, Systematic review, Occupational health
Introduction
Rationale
Work-related stress (WRS) differs from other occupational injuries and illnesses in several ways. Although stress-related disorders comprised only a small fraction of occupational injuries and illnesses reported to the United States Bureau of Labor Statistics in 1997 (the most recent surveillance data available), the median time away from work is more than four times greater for stress-related conditions than for injuries and illnesses overall.1 Work-related stress is thought to contribute to a range of occupational illnesses including cardiovascular disease.
Unlike physical, chemical, or biological occupational hazards, job stress cannot be readily and objectively measured. Two commonly used metrics for measuring WRS are the job strain and effort–reward imbalance models. The job strain model was developed by Karasek and is based on questions from the U.S. Department of Labor/University of Michigan Quality of Employment Survey.2 The instrument measures two work environment characteristics: job demand and the degree of the worker's decision latitude. Job demand includes factors that quantify the burden of work, such as too much work, insufficient time to complete tasks, and working extremely hard. Decision latitude includes the freedom a person feels in the job, the ability to participate in work decisions, and having input on the job. High job demand coupled with low decision latitude results in a high level of job strain.3 Johnson later added social support as a third dimension of the model.4 Jobs with high job strain combined with low social support are proposed to have the greatest health risk.
The effort–reward imbalance model approaches WRS from a different perspective. The effort construct is composed of demands and responsibilities of the job (extrinsic), a worker's need for control (intrinsic), and coping patterns utilized to deal with job demand. Reward is determined by esteem, money, and status control.5,6 The latter term accounts for lack of promotion, holding a job that does not match one's educational background, and moving down (instead of up) in the organizational structure.5
High levels of WRS have been associated with increased risk of cardiovascular mortality and mortality. A 28-year study of 812 employees in a Finnish manufacturing company found that individuals with high job strain or effort–reward imbalance had more than twice the risk of cardiovascular mortality compared to individuals with low job strain or effort–reward imbalance.7 Systematic reviews and meta-analyses consistently find at least moderate evidence of an association between WRS and cardiovascular disease.8–11 Evidence of a dose response relationship between job strain and angina was found in a large cohort of males in England.12 Among workers who suffered a myocardial infarction, those who experienced effort–reward imbalance at their jobs were found to be at increased risk of a recurrent coronary event.13
Identifying workers with early evidence of work-related cardiovascular disease may be useful in workplace prevention initiatives. Three intermediate cardiovascular disease endpoints have been investigated in relation to WRS: hypertension, heart rate variability (HRV), and carotid artery intima media thickness (CIMT). A review by Rosenthal and Alter found an association between WRS and hypertension.14 However, the findings from studies have been inconsistent in showing an association between WRS and HRV.15 While there have been reviews assessing the association between WRS and both hypertension and HRV, the relationship between CIMT and WRS has not been systematically evaluated.
Carotid artery intima media thickness is obtained by ultrasound examination of the carotid arteries, which quantifies the distance from the luminal–intima to the media–adventitia interface of the vessel.16–18 Guidelines for obtaining CIMT measurements are provided in the Mannheim Carotid Intima-Media Thickness consensus document.19 Standard ultrasound equipment includes B-mode ultrasound with a frequency >7 MHz.19 Specific measurement techniques include assessing the artery in a longitudinal orientation and preferentially measuring the carotid artery far wall.19
Numerous studies report higher relative risk for cardiovascular disease with increased CIMT.20 This has been found to linearly increase the Framingham risk score for cardiovascular disease.21 Carotid artery intima media thickness is high among people who have symptomatic coronary artery disease compared to asymptomatic controls. A thickening of the CIMT of more than 1 mm has been associated with a 5.07 (95% CI 3.08–8.36) relative risk (compared to those with ≤1 mm) for coronary artery disease in women and 1.85 (95% CI 1.28–2.69) in men, based on data from the Atherosclerosis Risk in Communities study.20 Carotid artery intima media thickness values are predictive of the extent of coronary artery atherosclerosis determined by coronary angiography.22,23 Carotid artery intima media thickness has been reported to be a stronger predictor of coronary artery disease than total cholesterol.23
The objective of this systematic review was to determine whether WRS is associated with increased CIMT, an intermediate endpoint of cardiovascular disease that can be measured objectively and non-invasively.
Methods
This review is organized based on the PRISMA guidelines for systematic reviews. This study protocol was not registered.24
Eligibility criteria
All the studies included in this review met specific criteria, as determined by the lead author. Studies had to include only employed individuals, be original research, and have measured CIMT via carotid ultrasound. There also had to be an exposure assessment of WRS.
Information sources
Pubmed, Ovid, and PsycINFO databases were searched for this review. The following search terms were used in PubMed: (Occupational OR work-related) AND (mental OR psychological AND stress) AND (carotid artery intima media thickness). Ovid was searched with the terms WRS and carotid artery intima media thickness. A string search in PsycINFO included (carotid artery intima media thickness) AND (work related OR occupational) AND (mental stress OR psychological stress).
The databases were searched on 4 October 2013, with no date restrictions. A second search was performed on 30 January 2014 and no new information was revealed. The lead author screened articles for eligibility.
Data items
Data were extracted from each study into a spreadsheet and organized by funding source, stress measurement instrument, ultrasound instrumentation, CIMT assessment technique, quality control measures, study population, study design, gender consideration, and confounding factors controlled for in the study. Funding sources and conflicts of interest were noted to assess the risk of bias. Studies were scored against a list of criteria similar to a method used in another systematic review (Table 1).
Table 1. Article ranking criteria.
| Category | Item | Scoring |
| A | Stress measurement | 0 – Use of an unvalidated assessment method |
| 1 – Use of a validated assessment method | ||
| B | Ultrasound Instrumentation | 0 – Unknown ultrasound mode AND <7 MHz or unknown frequency |
| 1 – B-mode or unknown ultrasound OR <7 MHz or unknown frequency | ||
| 2 – B-mode ultrasound >7 MHz | ||
| C | Carotid assessment | 0 – Image obtained from carotid near wall OR not specified |
| 1 – Image obtained as composite of carotid near and far wall | ||
| 2 – Image obtained from carotid far wall only | ||
| D | Quality control | 0 – No ultrasound measurement quality control information |
| 1 – Information regarding equipment (phantom scans) OR readers (interclass correlation) | ||
| 2 – Information regarding BOTH equipment and readers | ||
| E | Population | 0 – Population restricted to single organization or profession |
| 1 – Population derived from multiple organizations or professions | ||
| F | Study design | 0 – Cross-sectional or retrospective |
| 1 – Prospective | ||
| G | Gender | 0 – Gender not considered as a confounding factor |
| 1 – Gender taken into account as a confounding factor | ||
| 2 – Gender analyzed separately or single gender study | ||
| H | Confounding factors | 0 – Adjustment for only demographic and/or socioeconomic factors |
| 1 – Adjustment for demographic, socioeconomic, and bio-clinical factors such as blood lipids | ||
| 2 – Adjustment for demographic, socioeconomic, bio-clinical factors, and adiposity |
Results
Study selection
Twenty-nine articles were identified. Twenty articles did not meet the eligibility criteria or were duplicates. One additional article was identified by reviewing the citations of eligible studies (Figure 1).
Figure 1.
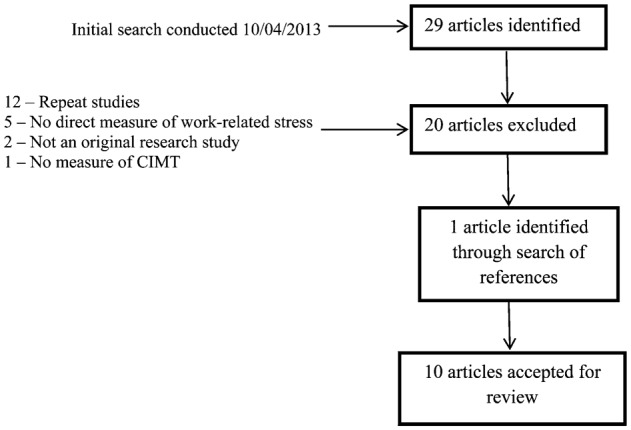
Article search strategy.
Study characteristics
Six studies were cross-sectional in design and four were prospective cohort studies. Eight studies found positive associations with WRS.25–32 Jedryka-Góral et al. reported a statistically significant inverse association between WRS and CIMT.33 Fujishiro et al. reported an association between CIMT and job control, but not with job strain (Table 3).34 The average sample size across studies was 928 subjects, with a range of 94–24801. Individual study characteristics, along with quality scoring, are listed in Table 2.
Table 3. Confounding factors, key results, and limitations for job stress and carotid artery intima media thickness (CIMT) studies.
| Author (year) | Confounders accounted for | Key results | Limitations |
| Prospective studies | |||
| Eller and Netterstrom (2007) | BP, WHR, BMI, fibrinogen, cholesterol, HDL, tobacco use, alcohol intake, and PA | Effort, reward, demands, and overcommitment correlated with IMT progression in women; ERI and reward correlated with IMT progression in men | Small population, small variation in psychosocial exposure, specific ultrasound technique not specified, and psychosocial exposure averaged over course of study |
| Everson et al. (1997) | Age, SBP, HDL, blood glucose, apolipoprotein B, BMI, alcohol consumption, cigarette smoking, education, diabetes, IHD, and medications | Carotid atherosclerosis was greater in subjects with high job demands and high blood pressure reactivity than subjects who were either less reactive or experienced less demanding jobs | Sample population was highly homogenous, sources of stress outside of work not considered, and did not use commonly accepted stress instrument |
| Hintsa et al. (2008) | Age, family history of CHD, family income, parental education, parental life satisfaction, and participant's education. | High job strain associated with higher CIMT in 27–39 year-old males. This was not significantly weakened after accounting for pre-employment factors | Possibility of selection bias based on analysis of non-participants, assessment made early in life and may not be applicable to older individuals, and self-reported job strain measures |
| Kamarck et al. (2012) | Baseline disease, age, sex, clinic SBP, fasting glucose, insulin, current smoking status, HDL, LDL, and waist circumference | A significant interaction between task demand and employment status on IMT progression. Mean demand ratings significantly associated with IMT progression for being at work and not at work. Both the demand and control subscales from the JCQ were not associated with IMT or plaque progression | Momentary demand and control scales not stated to be a validated stress measurement instrument, small sample size, analysis based on initial employment status with only 36% of respondents with initial employment data available reported working full or part-time at follow-up |
| Cross-sectional studies | |||
| Fujishiro et al. (2011) | BMI, smoking status, blood pressure, hypertension, diabetes, total and HDL cholesterol, age, household income, educational level, and place of birth | Job control correlation with common CIMT. Job strain not strongly associated with IMT | All information obtained via self-report; current job available only, therefore previous stress exposure not considered |
| Hintsanen et al. (2008) | Age, Socioeconomic status, Social support, Smoking status, Alcohol consumption, PA, BMI, HDL, and LDL cholesterol | Strain and correlated with increased IMT in men with the VAL/VAL COMT genotype only, not seen in women | Cross-sectional study cannot determine causation, previous employment not assessed, non-occupational stress not assessed, and young population with relatively short work history |
| Jedryka-Góral et al. (2006) | Age, DBP, LDL, anti-HSP antibodies, and anti-cardiolipin antibodies | Negative correlation between global job strain and IMT (R2 = 0.06). Increased IMT found with being a manager rather than a clerk | Small sample size, not a commonly used stress instrument |
| Nordstrom et al. (2001) | Age and body height | Increased likelihood of wall thickening of the common carotid artery in males, not females | Utilized stress assessment instrument similar to job strain, not stated as a validated stress measure, did not account for many confounding factors of cardiovascular disease, and cross-sectional design unable to determine causality |
| Rosvall et al. (2002) | Smoking, alcohol consumption, PA, LDL and HDL cholesterol, SBP, treatment for HTN, DM, BMI, social participation, emotional support, cohabiting status, # working hours, overtime, household duties/week, children at home, and education level of neighborhood | Women w/job strain showed high plaque prevalence odds and thicker IMT at carotid bifurcation compared to relaxed jobs (mean difference of 0.15 mm, 95% CI 0.07, 0.23). Women in active jobs also showed thicker IMT than relaxed jobs (mean difference of 0.10 mm, 95% CI 0.01, 0.19). This association was not seen in men | Cross-sectional design unable to determine causality, slightly more male subjects excluded |
| Xu et al. (2010) | Age, HTN, DM, Hyperlipidemia, and BMI | Effort, overcommitment, ERI positively correlated, and reward inversely correlated w/CIMT, even after adjustment in women. Similar association seen in men, but disappeared after adjustment (r = 0.120 in men, 0.307 in women for ERI and CIMT) | Population consisted of subject undergoing physical exam at one particular hospital, job stress assessed with a Chinese version of ERI questionnaire, and age was only demographic confounder assessed. Cross-sectional design unable to determine causality |
BMI, body mass index; BP, blood pressure; DBP, diastolic blood pressure; SBP, systolic blood pressure; PA, physical activity; WHR, waist-to-hip ratio.
Table 2. Quality ranking of work-related stress (WRS) and Carotid artery intima media thickness (CIMT) studies.
| Stress measurement | Ultrasound instrumentation | Carotid assessment | Quality control | Population | Study design | Gender | Confounding factors | Total Score |
| Category A | Category B | Category C | Category D | Category E | Category F | Category G | Category H | |
| Eller and Netterstrom25 | ||||||||
| Used effort–reward imbalance and demand-control models | Information not provided | No information provided regarding whether near or fall wall measurements were taken | The same individual performed all examinations and readings | 97% healthcare sector for females, 41% healthcare sector for males | Prosp. | Analyzed by gender | BP, WHR, BMI, fibrinogen, cholesterol, HDL, tobacco use, alcohol intake, and PA | |
| Score: 1 | 0 | 0 | 1 | 1 | 1 | 2 | 2 | 8 |
| Everson et al.26 | ||||||||
| Used questions from another study, not stated as validated | Used B mode ultrasound, 10 MHz | Images obtained from posterior wall of left carotid | Calibrated via phantom studies and IMT measurements made with edge detection software | Employed participants from the Kuopio ischemic heart disease risk factor study | Prosp. | Males only | age, SBP, HDL, blood glucose, apolipoprotein B, BMI, alcohol, smoking, education, diabetes, IHD, and medications | |
| Score: 0 | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 12 |
| Fujishiro et al.34 | ||||||||
| Job content questionnaire | B-mode ultrasound, frequency not specified | IMT reported as maximum IMT of near and far walls of right and left carotid. | Inter-reader reproducibility for CCA was 0.87, ICA 0.94. | Employed participants of the Multi-Ethnic Study of Atherosclerosis | X-S | Analyses adjusted for gender | BMI, smoking, blood pressure, HTN, diabetes, total and HDL cholesterol, age, income, education, and place of birth | |
| Score: 1 | 1 | 1 | 1 | 1 | 0 | 1 | 2 | 8 |
| Hintsa et al.27 | ||||||||
| Job demands measured with occupational stress questionnaire, job control measure with job content questionnaire | Ultrasound mode not specified, 13 MHz | LCA scanned according to an unspecified standardized protocol | Between observer coefficient of variation of 5.2% | Employed participants of The Cardiovascular Risk in Young Finns Study | Prosp. | Males only | Age, family history of CHD, income, education, parental education, and parental life satisfaction | |
| Score: 0 | 1 | 0 | 1 | 1 | 1 | 2 | 0 | 6 |
| Hintsanen et al.29 | ||||||||
| Job demands measured with occupational stress questionnaire, job control measure with job content questionnaire | Ultrasound mode not specified, 13 MHz | LCA scanned according to an unspecified standardized protocol | Between observer coefficient of variation of 5.2% | Employed participants of The Cardiovascular Risk in Young Finns Study | X-S | Analyzed by gender | Age, socioeconomic status, social support, smoking status, alcohol consumption, PA, BMI, HDL, and LDL cholesterol | |
| Score: 0 | 1 | 0 | 1 | 1 | 0 | 2 | 2 | 7 |
| Jedryka-Góral et al.33 | ||||||||
| Occupational stress/coping risk factors from: stress at work questionnaire | B-mode Ultrasound, 7.5 MHz | No information provided regarding ultrasound technique | No quality control information provided | 100 managers and 50 office workers | X-S | Analyses not gender-specific | Age, DBP, LDL, anti-HSP antibodies, and anti-cardiolipin antibodies | |
| Score: 0 | 2 | 0 | 0 | 0 | 0 | 0 | 1 | 3 |
| Kamarck et al.28 | ||||||||
| Job content questionnaire | B-mode ultrasound, unknown frequency | Far wall of left and right common carotid, carotid bulb, and proximal 1 cm of internal carotid | Ultrasound read with automated edge detection software | Currently employed participants | Prosp. | Analyses adjusted for gender | Baseline disease, age, sex, clinic SBP, fasting glucose, insulin, current smoking status, HDL, LDL, and waist circumference | |
| Score: 1 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 10 |
| Nordstrom et al.30 | ||||||||
| Six item questionnaire regarding work demands and work intrusion at home | B-mode ultrasound, unknown frequency | IMT estimated over 1 cm segment of carotid far wall | IMT measured with automated edge tracking system | Employees of a utility company | X-S | Analyzed by gender | Height, age, PA, fat intake, alcohol intake, BMI, SBP, total cholesterol, HDL, ethnicity, job category, education, smoking, BP meds, cholesterol meds, and DM | |
| Score: 0 | 1 | 2 | 1 | 0 | 0 | 2 | 2 | 8 |
| Rosvall et al.31 | ||||||||
| Job demands and decision latitude instrument by Karasek and Theorell | B-mode ultrasound, unknown frequency | Far wall IMT of CCA, bifurcation, and 1 cm of internal and external carotids | No quality control information provided | Employed participants from a sub cohort of Malmo Diet and Cancer Study | X-S | Analyzed by gender | Smoking, Alcohol, PA, LDL and HDL SBP, treatment for HTN, DM, BMI, social participation, emotional support, cohabiting status, hours worked, overtime, household duties, children at home, and educ. level of neighborhood | |
| Score: 1 | 1 | 2 | 0 | 1 | 0 | 2 | 2 | 9 |
| Xu et al.32 | ||||||||
| Effort–reward imbalance questionnaire | Ultrasound mode not specified, frequency of 8–13 MHz | Minimum of five carotid far wall measurements | No quality control information provided | Occupations including civil servants, managers, teachers, policemen, other white collar workers | X-S | Analyzed by gender | Age, HTN, DM, hyperlipidemia, and BMI | |
| Score: 1 | 0 | 2 | 0 | 1 | 0 | 2 | 2 | 8 |
Prosp., prospective; X-S, Cross-sectional; DM, diabetes mellitus; PA, physical activity; HTN, hypertension; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; HDL, high density lipoproteins; LDL, low density lipoproteins.
Risk of bias within studies
The funding source was not listed for one study.25 One investigator involved with the Kamarck study had an interest in a company providing a survey instrument used in the study. The most common funding sources were governmental agencies and private foundations. The risk of bias within studies was determined to be limited.
Prospective cohort study results
The four cohort studies had quality scores that ranged from 6 to 12 out of a possible 13. All four reported increased CIMT with higher levels of WRS. Study follow-up ranged from four to six years. Job strain or components of the demand/control model were utilized in three studies and one study used the effort–reward imbalance model.25 Two studies controlled for blood pressure, smoking, lipids, and diabetes.26,28 Eller and Netterstrom did not account for diabetes.25 Hintsa et al. did not account for any biomedical factors.27 Two studies enrolled both males and females and one reported gender specific results. Work-related stress was associated with CIMT thickening for both males and females, but the specific subscales exhibiting this relationship differed.25
Cross-sectional study results
Quality scores of the cross-sectional studies ranged from 3 to 9 (Table 2). Five out of six studies reported a positive relationship between CIMT progression and WRS. Jedryka-Góral et al. reported an inverse association between CIMT and WRS, but they did find greater CIMT among managers than among clerks, even though clerks tended to be older and had a higher prevalence of hypertension.33
Studies that investigated gender as a modifier of the WRS–CIMT association generated conflicting results. Two studies reported an association in males and not females.29,30 Two other studies found the opposite to be true.31,32 Differences in the WRS–CIMT association in males were found to be modified by a genetic factor. Men with the VAL/VAL catechol-O-methyl transferase allele had increased CIMT in relation to WRS, while those with either the MET/MET or MET/VAL allele did not.29
Bias
It is probable that studies reporting an association between stress and CIMT are more likely to be published than those reporting no association. This is a potential source of bias across the studies evaluated.
Discussion
Summary of evidence
The studies described above found modifiable and non-modifiable risk factors to be associated with increased CIMT. These include age, hypertension, gender, cigarette smoking, LDL and HDL cholesterol, and obesity.35 Increased intima-media thickness was also exhibited in sedentary individuals compared with people engaging in regular physical activity.36 All the cohort studies and the majority of the cross-sectional studies (Table 3) found greater CIMT with higher levels of WRS. The study by Jedryka-Góral et al., which had the lowest quality score, found an inverse association between WRS and IMT.33 The study population was composed of exclusively of white-collar workers and had considerably fewer study participants than other WRS–CIMT studies.33 Jedryka-Góral also used a stress assessment method that differed from studies reporting a positive relationship between WRS and CIMT. In a follow-up article by the same group, Bugajska et al. proposed that perhaps somatization of stress occurred in subjects reporting lower WRS, resulting in IMT changes.37
A possible effect modification by gender of the WRS–CIMT association was suggested. However, findings among individual studies are inconsistent about the direction of the effect modification. Gender differences in the WRS–HRV association are a challenge to interpret because of the variation in smoking status, cholesterol levels, degrees of WRS, and baseline CIMT by gender. Hintsanen et al. and Nordstrom et al. found a relationship between work related stress and increased CIMT in males, but observed no association among females.29,30 Conversely, two studies found a relationship between WRS and CIMT in females, but not males.31,32 Differences in smoking, BMI, and hypertension across studies may explain these conflicting results. Genetic characteristics also appear to modify the association between WRS and CIMT. Hintsanen et al. noted that WRS was associated with CIMT progression among those with the VAL/VAL allele of the catechol-O-methyl transferase gene.29
Critique
Defining a measure of risk, such as relative risk or an odds ratio, for the WRS–CIMT association based on the available literature was not possible due to inconsistencies in the stress assessment methods. The two main measures of WRS utilized were job strain and effort–reward imbalance. Although these scales were used in many of the studies, the specific questions included in the instruments varied (Table 4). In those that used the job strain model, the number of questions assessing demands ranged from two to five.25,28,31,32 The calculation of stress scores also differed by study. Job strain was evaluated as a combination of decision latitude and job demands based on the median score of each characteristic in two studies, with the other studies either calculating job strain using a different formula or analyzing the subscales independently (Table 4).25,27–29,31,34 The two studies which utilized effort–reward imbalance assessments also differed from one another in the number of questions asked, and in the formula for calculating imbalance.25,32 Other methods of assessing WRS included measuring only job demands and sources of pressure on the job scale.26,33
Table 4. Job strain and effort–reward imbalance scales.
| Author (year) | Scale items | Measurement technique |
| Job strain | ||
| Eller and Netterstrom (2007) | 2 items for demand, 12 items for control, 4 items for support | Each dimension analyzed independently |
| Fujishiro et al. (2011) | 5 items for demand, 9 items for job control | Categorized into high strain, low strain, and active and passive groups following trichotomization of the demands and control scales |
| Hintsa et al. (2008) | 3 items for work demand from the Occupational Stress Questionnaire, 9 items for control from the Job Content Questionnaire | A continuous indicated calculated by subtracting the demands from control |
| Hintsanen et al. (2008) | 3 items for work demand from the Occupational Stress Questionnaire, 9 items for control from the Job Content Questionnaire | Job strain obtained by division of the mean score of the job demands and control sub scales |
| Kamarck et al. (2012) | 5 items for job demand, job latitude composed of 6 item skill discretion and three item decision authority | Task demand and control analyzed separately |
| Rosvall et al. (2002) | 5 items for demand, 6 items for decision latitude | Scores dichotamized at the median to form job strain, active, passive, and relaxed jobs |
| Effort–reward imbalance | ||
| Eller and Netterstrom (2007) | 5 items for effort, 10 items for reward, 6 items for overcommitment | ERI calculated as effort/reward × (5/10) |
| Xu et al. (2010) | 6 items for effort, 11 items for reward, 6 items for overcommitment | ERI calculated as 11× effort/(6 × reward) |
Adjustment for cardiac risk factor confounders in the WRS–CIMT association also varied. The bio-clinical factors, particularly blood lipids, were accounted for to a greater degree than demographic factors. An indicator of adiposity was accounted for in half of the studies either as BMI or waist circumference. Workplace exposures other than stress were not considered in any studies. Although the relationship between these factors and CIMT is limited, there is evidence that some of these exposures may have an effect on CIMT and should be accounted for in future research. For example, exposure to ambient fine particulate matter is associated with an increased CIMT.38 An increased CIMT also has been shown in a population of barbecue workers exposed to carbon monoxide, as assessed by carboxyhemoglobin levels.39 Further studies need to be conducted in order to better characterize the effects of various workplace exposures on CIMT.
One general challenge in interpreting occupational epidemiology studies is that of selection. Workers with known cardiac disease may self-select into jobs with lesser degrees of WRS or leave the work force entirely. Workers in high strain jobs who subsequently develop cardiac disease may shift out of those positions, and potentially into new ones with lower degrees of WRS. Finally, people who work in high strain occupations may engage in poor health behaviors, which may not be adequately adjusted for in statistical models (i.e., residual confounding).40
The cross-sectional design also limits the ability to account for changing levels of WRS. Many of the studies examined the effect of WRS on cardiovascular outcomes in different age groups, but the length of employment in the particular job strain categories was not quantified. The frequency and direction of changes in WRS over time were not adequately addressed in any studies and should be a focus in the future. Although Eller and Netterstrom conducted a prospective study, the psychosocial stress levels were averaged between the initial and follow-up period.25 This presents a challenge in assessing the CIMT progress in relation to a changing psychosocial work environment.
Research needs
Carotid artery intima media thickness was associated with WRS in 9 out of 10 studies. Nevertheless, several critical research needs are apparent. First, a consistent measurement of stress should be established and followed for future WRS research. Although job strain and effort–reward imbalance are the most common measures, questionnaires vary widely between studies. Second, cumulative and recent WRS should be described and differentiated. Differentiating stress that has operated over a period of months or years in current or past jobs should be supplemented with current stress. Third, workplace environmental measurements should be collected to help quantify the contribution of environmental stressors, such as noise and chemical exposures on cardiovascular outcomes. Fourth, future studies must account for known cardiovascular disease risk factors. This is particularly critical, as some of these variables have been associated with WRS. Finally, the longitudinal evaluation of WRS in large cohort studies is critical, particularly for investigating gender differences. As the only prospective study, reporting gender differences noted a significant effect of CIMT and WRS for both sexes and the cross-sectional studies were divided into their associations, more prospective studies should be conducted to determine the differences in the CIMT and stress relationship between males and females. A prospective design would also account for those who leave the workforce, as those individuals may leave work because of stress or cardiovascular disease. This would help reduce the “healthy worker survivor effect” that can distort results of cross-sectional studies.
As the evidence of the association between CIMT and WRS is fairly consistent, interventional studies should be conducted to determine if changes in the rate of CIMT progression result from programs and/or policies aimed at reducing WRS. Various types of intervention studies examining smoking cessation and obesity have already been conducted.41,42 A similar approach may be used with WRS, in which efforts to decrease WRS will be evaluated as predictors in slowing the progression of CIMT.
Limitations
This review was limited to publications cataloged in the Pubmed, Ovid, PsycINFO databases, and snowballing the references of identified studies. An additional limitation involved restricting the articles identified by using the keywords provided in the methods. Publication bias may have resulted in an absence of negative studies.
Conclusions
Occupational health professionals, particularly those involved in workplace wellness, may wish to consider the use of non-invasive measures of subclinical cardiovascular disease as a means of evaluating health impacts of WRS. Carotid artery intima media thickness is a non-invasive method of assessing pre-clinical cardiovascular disease, which may be incorporated into routine medical monitoring. Given the limitations noted, the body of published studies of WRS suggests that higher degrees of occupational stress are associated with greater CIMT, a consistent finding even considering the variability across studies in the stress assessment measurement techniques and the number and types of confounding factors taken into account. Greater CIMT may translate into an increased risk of coronary artery disease. The literature suggests differences in cardiovascular responses to WRS by gender, being more consistent among males. Large cohort studies as well as intervention studies should be conducted in order to better characterize the relationship of stress and CIMT and to reduce the burden of cardiovascular disease attributable to workplace stress.
Disclaimer Statements
Contributors Mark Wilson is the lead author of the paper. Lorraine Conroy and Sam Dorevitch substantially contributed to the format, content, and revisions of the manuscript. Approval was received from each author prior to submission.
Funding This research was supported in part by National Institute for Occupational Safety and Health Grant T42/OH008672. The contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC/NIOSH.
Conflicts of interest The authors have no conflicts of interest to declare.
Ethics approval Ethics approval was not required as this manuscript is a review of previously published research.
Acknowledgments
We would like to thank Lee Friedman for his valuable contribution to the final preparation of this manuscript.
References
- 1.Webster T, Bergman B. Occupational stress: counts and rates. Compens Work Cond. 1999;Fall:38–41. [Google Scholar]
- 2.Schnall PL, Pieper C, Schwartz JE, Karasek RA, Schlussel Y, Devereux RB, et al. The relationship between ‘job strain,’ workplace diastolic blood pressure, and left ventricular mass index. Results of a case-control study. JAMA. 1990;263(14):1929–35. [PubMed] [Google Scholar]
- 3.Karasek RA., Jr Job demands, job decision latitude, and mental strain: implications for job redesign. Adm Sci Q. 1979;24(2):285–308. [Google Scholar]
- 4.Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B. The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol. 1998;3(4):322–55. doi: 10.1037//1076-8998.3.4.322. [DOI] [PubMed] [Google Scholar]
- 5.Siegrist J. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol. 1996;1(1):27–41. doi: 10.1037//1076-8998.1.1.27. [DOI] [PubMed] [Google Scholar]
- 6.van Vegchel N, de Jonge J, Bosma H, Schaufeli W. Reviewing the effort-reward imbalance model: drawing up the balance of 45 empirical studies. Soc Sci Med. 2005;60(5):1117–31. doi: 10.1016/j.socscimed.2004.06.043. [DOI] [PubMed] [Google Scholar]
- 7.Kivimaki M, Leino-Arjas P, Luukkonen R, Riihimaki H, Vahtera J, Kirjonen J. Work stress and risk of cardiovascular mortality: prospective cohort study of industrial employees. BMJ. 2002;325(7369):857. doi: 10.1136/bmj.325.7369.857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Eller NH, Netterstrom B, Gyntelberg F, Kristensen TS, Nielsen F, Steptoe A, et al. Work-related psychosocial factors and the development of ischemic heart disease: a systematic review. Cardiol Rev. 2009;17(2):83–97. doi: 10.1097/CRD.0b013e318198c8e9. [DOI] [PubMed] [Google Scholar]
- 9.Backe EM, Seidler A, Latza U, Rossnagel K, Schumann B. The role of psychosocial stress at work for the development of cardiovascular diseases: a systematic review. Int Arch Occup Environ Health. 2012;85(1):67–79. doi: 10.1007/s00420-011-0643-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Belkic KL, Landsbergis PA, Schnall PL, Baker D. Is job strain a major source of cardiovascular disease risk? Scand J Work Environ Health. 2004;30(2):85–128. doi: 10.5271/sjweh.769. [DOI] [PubMed] [Google Scholar]
- 11.Kivimaki M, Virtanen M, Elovainio M, Kouvonen A, Vaananen A, Vahtera J. Work stress in the etiology of coronary heart disease–a meta-analysis. Scand J Work Environ Health. 2006;32(6):431–42. doi: 10.5271/sjweh.1049. [DOI] [PubMed] [Google Scholar]
- 12.Sacker A, Bartley MJ, Frith D, Fitzpatrick RM, Marmot MG. The relationship between job strain and coronary heart disease: evidence from an English sample of the working male population. Psychol Med. 2001;31(2):279–90. doi: 10.1017/s0033291701003270. [DOI] [PubMed] [Google Scholar]
- 13.Aboa-Eboule C, Brisson C, Maunsell E, Bourbonnais R, Vezina M, Milot A, et al. Effort-reward imbalance at work and recurrent coronary heart disease events: a 4-year prospective study of post-myocardial infarction patients. Psychosom Med. 2011;73(6):436–47. doi: 10.1097/PSY.0b013e318222b2d8. [DOI] [PubMed] [Google Scholar]
- 14.Rosenthal T, Alter A. Occupational stress and hypertension. J Am Soc Hypertens. 2012;6(1):2–22. doi: 10.1016/j.jash.2011.09.002. [DOI] [PubMed] [Google Scholar]
- 15.Jarczok MN, Jarczok M, Mauss D, Koenig J, Li J, Herr RM, et al. Autonomic nervous system activity and workplace stressors – a systematic review. Neurosci Biobehav Rev. 2013;37(8):1810–23. doi: 10.1016/j.neubiorev.2013.07.004. [DOI] [PubMed] [Google Scholar]
- 16.Adolphe A, Cook LS, Huang X. A cross-sectional study of intima-media thickness, ethnicity, metabolic syndrome, and cardiovascular risk in 2268 study participants. Mayo Clin Proc. 2009;84(3):221–8. doi: 10.4065/84.3.221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Touboul PJ, Grobbee DE, Ruijter H. Assessment of subclinical atherosclerosis by carotid intima media thickness: technical issues. Eur J Prev Cardiol. 2012;19(2 Suppl):18–24. doi: 10.1177/2047487312448990. [DOI] [PubMed] [Google Scholar]
- 18.Baldassarre D, Amato M, Bondioli A, Sirtori CR, Tremoli E. Carotid artery intima-media thickness measured by ultrasonography in normal clinical practice correlates well with atherosclerosis risk factors. Stroke. 2000;31(10):2426–30. doi: 10.1161/01.str.31.10.2426. [DOI] [PubMed] [Google Scholar]
- 19.Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P, Bornstein N, et al. Mannheim carotid intima-media thickness consensus (2004–2006). An update on behalf of the Advisory Board of the 3rd and 4th Watching the Risk Symposium, 13th and 15th European Stroke Conferences, Mannheim, Germany, 2004, and Brussels, Belgium, 2006. Cerebrovasc Dis. 2007;23(1):75–80. doi: 10.1159/000097034. [DOI] [PubMed] [Google Scholar]
- 20.Linhart A, Gariépy J, Massonneau M, Dauzat M. Carotid intima-media thickness: the ultimate surrogate end-point of cardiovascular involvement in atherosclerosis. Appl Radiol. 2000;29(3):25–39. [Google Scholar]
- 21.Campuzano R, Moya JL, Garcia-Lledo A, Tomas JP, Ruiz S, Megias A, et al. Endothelial dysfunction, intima-media thickness and coronary reserve in relation to risk factors and Framingham score in patients without clinical atherosclerosis. J Hypertens. 2006;24(8):1581–8. doi: 10.1097/01.hjh.0000239294.17636.27. [DOI] [PubMed] [Google Scholar]
- 22.Graner M, Varpula M, Kahri J, Salonen RM, Nyyssonen K, Nieminen MS, et al. Association of carotid intima-media thickness with angiographic severity and extent of coronary artery disease. Am J Cardiol. 2006;97(5):624–9. doi: 10.1016/j.amjcard.2005.09.098. [DOI] [PubMed] [Google Scholar]
- 23.Holaj R, Spacil J, Petrasek J, Malik J, Haas T, Aschermann M. Intima-media thickness of the common carotid artery is the significant predictor of angiographically proven coronary artery disease. Can J Cardiol. 2003;19(6):670–6. [PubMed] [Google Scholar]
- 24.Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 20091514264–9. W64 [DOI] [PubMed] [Google Scholar]
- 25.Eller NH, Netterstrom B. Psychosocial factors at home and at work and four-year progression in intima media thickness. Int J Behav Med. 2007;14(1):21–9. doi: 10.1007/BF02999224. [DOI] [PubMed] [Google Scholar]
- 26.Everson SA, Lynch JW, Chesney MA, Kaplan GA, Goldberg DE, Shade SB, et al. Interaction of workplace demands and cardiovascular reactivity in progression of carotid atherosclerosis: population based study. BMJ. 1997;314(7080):553–8. doi: 10.1136/bmj.314.7080.553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hintsa T, Kivimaki M, Elovainio M, Vahtera J, Hintsanen M, Viikari JS, et al. Is the association between job strain and carotid intima-media thickness attributable to pre-employment environmental and dispositional factors? The Cardiovascular Risk in Young Finns Study. Occup Environ Med. 2008;65(10):676–82. doi: 10.1136/oem.2007.037622. [DOI] [PubMed] [Google Scholar]
- 28.Kamarck TW, Shiffman S, Sutton-Tyrrell K, Muldoon MF, Tepper P. Daily psychological demands are associated with 6-year progression of carotid artery atherosclerosis: the Pittsburgh Healthy Heart Project. Psychosom Med. 2012;74(4):432–9. doi: 10.1097/PSY.0b013e3182572599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hintsanen M, Elovainio M, Puttonen S, Kivimaki M, Lehtimaki T, Kahonen M, et al. Val/Met polymorphism of the COMT gene moderates the association between job strain and early atherosclerosis in young men. J Occup Environ Med. 2008;50(6):649–57. doi: 10.1097/JOM.0b013e318165c7ec. [DOI] [PubMed] [Google Scholar]
- 30.Nordstrom CK, Dwyer KM, Merz CN, Shircore A, Dwyer JH. Work-related stress and early atherosclerosis. Epidemiology. 2001;12(2):180–5. doi: 10.1097/00001648-200103000-00009. [DOI] [PubMed] [Google Scholar]
- 31.Rosvall M, Ostergren PO, Hedblad B, Isacsson SO, Janzon L, Berglund G. Work-related psychosocial factors and carotid atherosclerosis. Int J Epidemiol. 2002;31(6):1169–78. doi: 10.1093/ije/31.6.1169. [DOI] [PubMed] [Google Scholar]
- 32.Xu W, Hang J, Cao T, Shi R, Zeng W, Deng Y, et al. Job stress and carotid intima-media thickness in Chinese workers. J Occup Health. 2010;52(5):257–62. doi: 10.1539/joh.l9157. [DOI] [PubMed] [Google Scholar]
- 33.Jedryka-Goral A, Pasierski T, Zabek J, Widerszal-Bazyl M, Radkiewicz P, Szulczyk GA, et al. Risk factors for atherosclerosis in healthy employees-a multidisciplinary approach. Eur J Intern Med. 2006;17(4):247–53. doi: 10.1016/j.ejim.2005.12.005. [DOI] [PubMed] [Google Scholar]
- 34.Fujishiro K, Diez Roux AV, Landsbergis P, Baron S, Barr RG, Kaufman JD, et al. Associations of occupation, job control and job demands with intima-media thickness: the Multi-Ethnic Study of Atherosclerosis (MESA). Occup Environ Med. 2011;68(5):319–26. doi: 10.1136/oem.2010.055582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Krishnan P, Balamurugan A, Urbina E, Srinivasan SR, Bond G, Tang R, et al. Cardiovascular risk profile of asymptomatic healthy young adults with increased carotid artery intima-media thickness: the Bogalusa Heart Study. J La State Med Soc. 2003;155(3):165–9. [PubMed] [Google Scholar]
- 36.Galetta F, Franzoni F, Tocchini L, Camici M, Milanesi D, Belatti F, et al. Effect of physical activity on heart rate variability and carotid intima-media thickness in older people. Intern Emerg Med. 2013;8(Suppl 1):S27–9. doi: 10.1007/s11739-013-0919-9. [DOI] [PubMed] [Google Scholar]
- 37.Bugajska J, Widerszal-Bazyl M, Radkiewicz P, Pasierski T, Szulczyk GA, Zabek J, et al. Perceived work-related stress and early atherosclerotic changes in healthy employees. Int Arch Occup Environ Health. 2008;81(8):1037–43. doi: 10.1007/s00420-007-0297-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Adar SD, Sheppard L, Vedal S, Polak JF, Sampson PD, Diez Roux AV, et al. Fine particulate air pollution and the progression of carotid intima-medial thickness: a prospective cohort study from the multi-ethnic study of atherosclerosis and air pollution. PLoS Med. 2013;10(4):e1001430. doi: 10.1371/journal.pmed.1001430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Davutoglu V, Zengin S, Sari I, Yildirim C, Al B, Yuce M, et al. Chronic carbon monoxide exposure is associated with the increases in carotid intima-media thickness and C-reactive protein level. Tohoku J Exp Med. 2009;219(3):201–6. doi: 10.1620/tjem.219.201. [DOI] [PubMed] [Google Scholar]
- 40.Theorell T, Alfredsson L, Knox S, Perski A, Svensson J, Waller D. On the interplay between socioeconomic factors, personality and work environment in the pathogenesis of cardiovascular disease. Scand J Work Environ Health. 1984;10(6 Spec No):373–80. doi: 10.5271/sjweh.2305. [DOI] [PubMed] [Google Scholar]
- 41.Johnson HM, Piper ME, Baker TB, Fiore MC, Stein JH. Effects of smoking and cessation on subclinical arterial disease: a substudy of a randomized controlled trial. PLoS One. 2012;7(4):e35332. doi: 10.1371/journal.pone.0035332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Cooper JN, Columbus ML, Shields KJ, Asubonteng J, Meyer ML, Sutton-Tyrrell K, et al. Effects of an intensive behavioral weight loss intervention consisting of caloric restriction with or without physical activity on common carotid artery remodeling in severely obese adults. Metabolism. 2012;61(11):1589–97. doi: 10.1016/j.metabol.2012.04.012. [DOI] [PMC free article] [PubMed] [Google Scholar]