

Abstract
Background:
Breast cancer is one of the most common cancers in females. Methods of screening are the best among early detection methods. The goal of this study is effect of education on preventive behaviors of breast cancer in female teachers of guidance schools of Zahedan city based on health belief model
Materials and Methods:
This study was a semi-experimental, a kind of case-control research. This study was carried on 240 female teachers in guidance schools, Zahedan city, in 2011-2012 academic years with multi-stage sampling. Data collection tool was a questionnaire that was used after confirmation of validity and reliability. Data were collected with questionnaire after analysis, educational intervention with lecture, view video, group discussion, question and answer performed. Two month after intervention, secondary evaluation was performed. Collected data with SPSS software and appropriate statistical tests like: Paired t-test, independent t-test, regression analysis, Chi-square were analyzed.
Results:
Persons mean age in this study was 39.40(±7.4) years. In awareness item and health belief model constructs (awareness, perceived susceptibility, perceived seriousness, perceived benefits, perceived barriers, self-efficiency, behavior) and also practice, paired t-test showed significant difference among before and after education (P > 0.0001). In two groups based on Chi-square in level of education and married status, there were no significant differences. Also, regression analysis outcomes showed that perceived barriers had the most effect on behavior, and this construct could be predictor of preventive behaviors from breast cancer.
Conclusions:
The findings of this study could conclude that educational programs designed based on the health belief model have significant impact on improving preventive treatment of breast cancer. Given the fact that Iran has a very high incidence of breast cancer, since Iranian women's awareness level and performance specially research samples according to educational level (associate degree and higher) and employment conditions as model for today girls and future mothers in breast cancer screening before educational intervention was very low. So, due to need, increasing women's awareness in health belief model framework to promote preventive behaviors is recommended.
Keywords: Breast cancer, health belief model, preventive behaviors and female teachers’ education
INTRODUCTION
Each year, more than one million new cases of breast cancer have been diagnosed in the world, and for this reason, more than six hundred thousand cases death occurs.[1] In comparison with other countries, Iranian women are suffering with breast cancer a decade earlier, and 70% of patients are diagnosed at an advanced stage.[2] Several studies have shown that in Iran, the prevalence of this disease is among 35-44 years of age.[3] Early diagnosis is infrastructure for effort to reduce mortality due to breast cancer. Effort to breast cancer early detection led to the creation of programs for screening and discovery of the disease in its early stages.[4] Based on studies, the cancer prevention and it's early diagnosis is critical factor in controlling the disease and to increase survival rate.[5] Given the importance of early diagnosis in improved quality of life of patients, the best to achieve this goal is secondary prevention (screening).[6] Breast screening in women include: Mammography, clinical breast examination (CBE), breast self-examination (BSE).[7] If monthly breast self-examination and mammography is done at the appropriate time by clinician and by person, it could prevent 95% of breast cancer cases progress to advanced stages.[8] Many women, due to lack of information and awareness of breast cancer screening practices, are diagnosed in advanced stages of breast cancer. Due to these factors, raising awareness of breast cancer screening is essential in society.[9] Choosing a health education model, the first step in the process of planning an education program and effective health education, depends on dominance at the use of theory and strategies that are best suited to each event. Health belief model is a specific model for individual health behavior so that person knows. This model can be used in predicting health behaviors such as assertiveness and various contraceptive methods.[10] Use of this pattern in breast cancer screening education has been approved.[11] Structures of the model are perceived sensitivity and severity of illness, perceptual benefits of preventive behavior, perceptual barriers to preventive behavior, cause to action and self-efficacy than preventive behavior is.[12] When people know the risk for disease (perceived susceptibility), understand the disease has serious and potential consequences (perceived intensity), believe that preventive action has positive outcomes (perceived benefits), behavior obstacles is less than the earned benefits, belief that they have the ability to perform health behaviors (self-efficacy), There is a greater chance that behavior do.[13] Since the factors associated with health behavior in the framework of the health belief model can be used to design effective educational interventions, this study aim designed to determine the effect of education on preventive behaviors of breast cancer in female teachers of guidance schools of Zahedan city based on health belief model.
MATERIALS AND METHODS
This study has been done with a semi-experimental in form of case-control on 240 female teachers of guidance schools of Zahedan city that interred to study with multi-stage sampling and randomly divided into control and experimental groups.
Inclusion criteria was female teachers were being taught in girls’ guidance schools with degrees such as associate degree, bachelor, master, all those who had experienced breast cancer were not included in the study. The required sample size by confidence coefficient and test power of 80% was obtained using the following formula:
n = (Z1−α/2 + Z1−β)2(S12 + S22)/(x1 − x2)2
110 Persons in per group (n = 220 in each group) were determined. With taking to possible loss, 20 persons were considered as stored. Finally, 240 persons (120 persons in each group) were calculated. There were 56 governmental and non-governmental girls’ guidance schools in district 1 and 2 in Zahedan city. Schools in district 2 were selected as study group and schools in district 1 were selected as control group randomly. Twelve schools have been randomly selected, and teachers in these schools after obtaining informed consent enrolled into the study. Questionnaires based on the Health Belief Model constructs were distributed among them. The questionnaire consisted of two parts: The first part includes demographic questions such as age, education, marital status and the second part includes knowledge questions, the health belief model constructs. This collection includes questions related to perceived susceptibility (6 questions), perceived seriousness (5 questions), perceived benefits (5 questions), perceived barriers (5 questions), self-efficacy (5 questions), and cause to action (6 questions). Questions about consciousness: Three score for a correct answer of the question, 2 score for do not know answer and1 score was assumed for incorrect answers. Expressions of attitude, self-efficacy, and perceived benefits and barriers were developed based on the Likert scale. Given the spectrum of 5, the scores (score 5 for strongly agree, score 4for agree, score 3 for no comment, score 2 for opposed, and score 1 for those completely disagreed) were considered. The questions related to preventive behaviors: Five questions are in relation to fruit and vegetable consumption, physical activity, mammography, clinical breast examination, and breast self-examination. For grading standards: (always: Score 4, sometimes: Score 3, most: Score 2, never: Score 1) was considered. Thus, minimum of 5 and its maximum of 20 score. Minimum and maximum scores gained by perceived susceptibility structures were 6 and 30. Minimum and maximum score gained by perceived seriousness structures were 5 and 25, minimum and maximum score gained by perceived barriers and benefits and self-efficacy structures were5 and 25. In structure cause to action, the percentages were taken.
For determining the validity of questionnaire, the content validity method was used. The questionnaire was approved by 10 participants from relevant experts. For awareness section 0.87, in model's 0.91, in performance section 0.79 obtained. Its reliability was confirmed by Cranach's alpha. Cranach's alpha amount for reliability 76 percent was calculated. For collecting data first researchers explained the research objectives and also about obtained information from participants in the study will be confidential to teachers, If they had tendency to participate in the study, they were enrolled. Data after encryption using software SPSS (version 18) was analyzed.
RESULTS
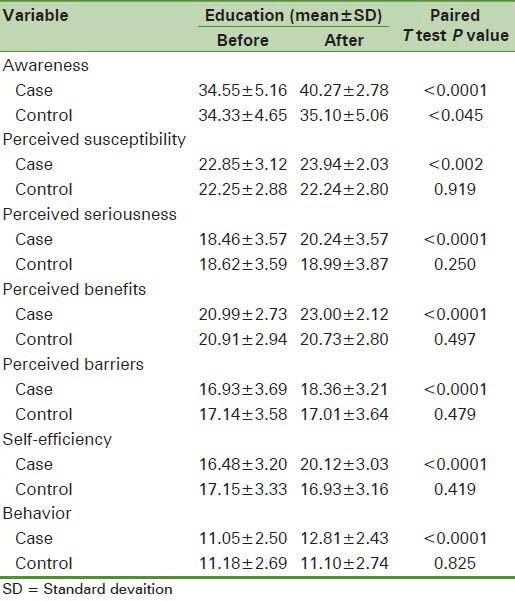
This study with the aim effect of educational intervention based on the Health Belief Model on modifying breast cancer preventive behaviors on 240 female teachers in guidance schools of Zahedan city. Mean age (SD) of the participants in this study was 39.4(±7.4) years. The youngest participant was 21-years-old, and the oldest participant was 65-years-old. Level of education: 98 people (40.8%) had Associate degree, 134 (55.8%) were bachelors and 8 (3.3%) were masters. Two hundred and sixteen (90%) of the subjects were married, 13 were single (5.4%), and 11 person (4.6 percent) were among other items (widow and divorced). Control and case group based on Chi-square test found no statistically significant difference in terms of overall marital and educational level [Table 1]. T-test showed that two groups had significant difference in age and interventional group was younger (P = 0.002). Paired t-test and independent t-test showed that the mean score awareness in case group before and after education intervention has significant difference (P < 0.0001): Susceptibility score (P < 0.002), self-efficacy, seriousness, perceived benefits, perceived barriers (P < 0.0001). Behavior scores before and after intervention in case group had a significant difference. But, in the control group there was no significant difference before and after intervention [Table 2].
Table 1.
Comparison frequency change in education level and marital status groups study

Table 2.
Comparison mean and standard deviation scores of awareness, behavior and structural health belief model before and after educational intervention
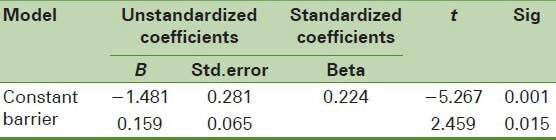
Regression analysis showed that the strongest variable predictor behavior after educational intervention was perceived barriers variable so that for every unit increase in perceived barriers variable, predicted that behavior change score increase to 0.224 [Table 3].
Table 3.
Prediction doing preventive behaviors from breast cancer in studied persons
DISCUSSION
In this study, educational program based on health belief model performed. This model is one of the patterns of behavioral science theories used to assess health-related problems and is widely used to describe the behavior of breast cancer controlling.[14] This model explains up to 47% of the variance in breast cancer control behavior.[15]
In this study, awareness score rather than before of educational intervention significantly increased; in direction with this study, Pavic and colleagues showed that education has increased women's awareness of breast cancer screening.[16] Also, in Hacihasanoglustudy, education increased awareness of BSE.[17]
This outcomes show that women needs education for increasing their awareness about breast cancer predictive behaviors. So, informing and increasing awareness of people before performance is a good method for helping them in direction doing performance.[18] Moudy and colleagues study showed that education with using health belief model on susceptibility, seriousness, perceived benefits, barriers structures and students’ awareness about breast self-examination had significantly affect except in self-efficiency structure were in agreement with this study outcomes.[19] Karimi and colleagues showed that among awareness mean scores, performance scores and HBM constructs except self-efficiency construct before and after education there were a significant difference.[20] Gammage et al., also indicated increase mean sores in model structures (perceived susceptibility, perceived seriousness, perceived benefits and perceived barriers) rather than before of educational intervention that The results were in agreement with this study.[21]
In this study, perceived seriousness scores, before and after intervention, had a significant difference the same Shidfar on patients with Angina pectoris.[22] This study showed that perceived barriers score in case group before and after educational intervention has significant difference. This outcomes are similar to study in Spanish women for research effects of educational program on their knowledge and beliefs about breast cancer.[23]
From factors associated with increasing perceived susceptibility scores it can be noted that if a person to be sensitive about health issues and belief that without symptoms of disease can become patient, this sensitivity can lead to the prevention of abuse and the risk of disease.[24] Perceived benefits from a behavior refer to understanding of person from benefits of one behavior.[25] One can with explain the efficiency and values of recommended behaviors for women encourage them to perform health behaviors. Perceived barriers indicated a perception of internal and external barriers to perform a behavior.[26] With better understanding barriers doing preventive behaviors and try to eliminate these barriers, way for health care procedures will be smoothing. Outcomes of this study showed that education had positive effect on awareness, beliefs, and breast cancer screening behavior. Results of regression analyzes indicated that perceived barriers has had the most influence on behavior. This construct can be a predictor of behavior in prevention of breast cancer. In this direction, Lance outcomes indicated that self-efficiency and perceived barriers were important variables in condom use and safe sex.[27] Also, In Karimi study, perceived barriers after self-confidence was the most predictive power in BSE.[28] In mentioned studies, outcomes except in self-efficiency construct were similar to this study.
In limitations of this study, low volume of the samples could be mentioned. It also included female teachers only and, therefore, may not have ability to generalize to the entire community of Iranian women.
CONCLUSIONS
The findings of this study could conclude that educational programs designed based on the health belief model have significant impact on improving preventive treatment of breast cancer. Given the fact that Iran has a very high incidence of breast cancer, since Iranian women awareness level and action specially research samples according to educational level (associate degree and higher) and employment conditions as model for today girls and future mothers in breast cancer screening before educational intervention was very low. So, due to need, increasing women's awareness in HBM frame work to promote preventive behaviors is recommended. On the other hand, due to the low cost of preventive activities, the necessary education in the field through lectures, question and answer, group discussions, film screenings, and providing education manuals for in-service training courses for teachers is given.
ACKNOWLEDGMENTS
This study is part of a master's thesis Article first author at the at the Zahedan university of medical sciences and also research project with number 2502Researchers must know itself thereby hearty thanks to deputy of Health School of Medical Sciences University and Education organizations in Zahedan and all participants in the research project.
Footnotes
Source of Support: Zahedan University of Medical Sciences
Conflict of Interest: None declared
REFERENCES
- 1.Stewart BW, Kleihues PE. Lyon, France: IARC Press; 2003. World cancer report. [Google Scholar]
- 2.Harirchi I, Karbakhsh M, Kashefi A, Momtahen AJ. Breast cancer in Iran: Results of multi-center study. Asian Pac J Cancer Prev. 2004;5:24–7. [PubMed] [Google Scholar]
- 3.Fasihi Harandy T, Anoosheh M, Ghofranipour F, Montazeri A, Ahmadi F, Mohammadi E, et al. Health-related quality of life in Iranian breast cancer survivors: A qualitative study. Payesh. 2012;11:73–81. [Google Scholar]
- 4.Rutledge DN, Barsevick A, Knobf MT, Book binder M. Breast cancer detection: Awareness attitudes and behaviors of women from Pennsylvania. Oncol Nurs Forum. 2001;28:1032–40. [PubMed] [Google Scholar]
- 5.McDonald S, Saslow D, Alciati MH. Behavior and reporting of clinical breast examination: Areview of literature cancer. J Clin. 2004;54:345–61. doi: 10.3322/canjclin.54.6.345. [DOI] [PubMed] [Google Scholar]
- 6.Franken F, Kirsten M. Health belief model of breast cancer screeningfor female college students. Masters Theses and Doctoral Dissertations. Eastern Michigan University. 2009;258:1–95. [Google Scholar]
- 7.Calderon-Margalit R, Paltiel O. Prevention of breast cancer in women who carry BRCA1 or BRCA2 mutations: A critical review of the literature. Int J Cancer. 2004;112:357–64. doi: 10.1002/ijc.20429. [DOI] [PubMed] [Google Scholar]
- 8.Yavari P, Mehrabi Y, Hoseingholi MA. Awareness and practice of women's regarding breast self-examination, A case control study. Persian J Ardabil Univ Med Sci. 2005;5:371–9. [Google Scholar]
- 9.Ceber E, Soyer MT, Ciceklioglu M, Cimat S. Breast cancer risk assessment and risk perception on nurses and midwives in Bornova Health District in Turkey. Cancer Nurs. 2006;29:244–9. doi: 10.1097/00002820-200605000-00013. [DOI] [PubMed] [Google Scholar]
- 10.Oyekale AS, Oyekale TO. Application of health belief model for promoting behavior change among Nigerian single youth. Afr J Repro’d Health. 2010;14:63–75. [PubMed] [Google Scholar]
- 11.Ceber E, Yücel U, Mermer G, Ozentürk G. Health beliefs and breast self-examination in a sample of Turkish women academicians in a university. Asian Pac J Cancer Prev. 2009;10:213–8. [PubMed] [Google Scholar]
- 12.Champion VL. Revised susceptibility, benefits, and barriers scale for mammography screening. Res Nurs Health. 1999;22:341–8. doi: 10.1002/(sici)1098-240x(199908)22:4<341::aid-nur8>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 13.Assari S. Theory based health education: Application of health belief model for Iranian patients with myocardial infarction. J Res Med Sci. 2011;16:580–2. [PMC free article] [PubMed] [Google Scholar]
- 14.Wu TY, Yu MY. Reliability and validity of the mammography screening beliefs questionnaire among Chinese American women. Cancer Nurs. 2003;26:131–42. doi: 10.1097/00002820-200304000-00007. [DOI] [PubMed] [Google Scholar]
- 15.Nahcivan NO, Secginli S. Health belief related to breast self-examination in a sample of Turkish women. Oncol Nurs Forum. 2007;34:425–32. doi: 10.1188/07.ONF.425-432. [DOI] [PubMed] [Google Scholar]
- 16.Pavic D, Schell MJ, Dancel RD, Sultana S, Lin L, Sejpal SV, et al. Comparison of three methods to increase awareness about Breast cancer and Breast cancer screening in screening mammography patients. Acad Radiol. 2007;14:553–60. doi: 10.1016/j.acra.2007.01.011. [DOI] [PubMed] [Google Scholar]
- 17.Hacihasanoglu R, Gozum S. The effect of education on the awareness levels and beliefs regarding breast self-examination on women attending a public education center. Eur J Oncol Nurs. 2008;12:58–64. doi: 10.1016/j.ejon.2007.06.005. [DOI] [PubMed] [Google Scholar]
- 18.Hatefnia E, Niknami SH, Mahmoudi M, Ghofranipour F, Lamyian M. The Effects of health belief model education on awareness attitude and behavior of Tehran pharmaceutical industry employees regarding breast cancer and mammography. Behbood J. 2010;14:42–53. [Google Scholar]
- 19.Moodi M, Mood MB, Sharifirad GR, Shahnazi H, Sharifzadeh G. Evaluation of breast self-examination program using Health Belief Model in female students. J Res Med Sci. 2011;16:316–22. [PMC free article] [PubMed] [Google Scholar]
- 20.Karimy M, Hasani M, Khorram R, Ghaffari M, Niknami SH. The Effect of Education, Based on Health Belief Model on Breast Self- Examination in Health Liaisons of ZarandiehCity. Tabib-e-Shargh 2006. 2007;10:283–91. [Google Scholar]
- 21.Gammage KL, Francoeur C, Mack DE, Klentrou P. Osteoporosis health beliefs and awareness in college students: Therole of dietary restraint. Eat Behav. 2009;10:65–7. doi: 10.1016/j.eatbeh.2008.10.006. [DOI] [PubMed] [Google Scholar]
- 22.Shidfar MR, Hosieni M, Shojaeizadeh D, Asasi N, Majlesi F, Nazemi S, et al. The effect of health education program on awareness and attitude cardiovascular diseases in the Mashhad hospitalPersian. J Birjand Univ Med Sci. 2007;14:18–27. [Google Scholar]
- 23.Hall CP, Hall JD, Pfriemer JT, Wimberley PD, Jones CH. Effects of a culturally Sensitive Education Program on the Breast Cancer Awareness and Beliefs of Hispanic Women. Oncol Nurs Forum. 2007;34:1195–202. doi: 10.1188/07.ONF.1195-1202. [DOI] [PubMed] [Google Scholar]
- 24.Taghdisi MH, Nejadsadeghi E. The effect of health education based on health belief model on behavioral promotion of urinary infection prevention in pregnant women. J Res Health. 2012;2:126–36. [Google Scholar]
- 25.Glanz K, Rimer BK, Viswanath K. Francisco: Jossey-BassInc Pub; 2008. Health behavior and health education: Theory, research, and practice; pp. 45–62. [Google Scholar]
- 26.Moodi M, Hassanzadeh A, Charkazi A, Shahnazi H, Sharifirad GH. A Survey of the psycho-cognitive factors affecting breast cancer screening behaviors at different stages of change among female teachers in Isfahan, Iran. J Health Syst Res. 2011;7:770–81. [Google Scholar]
- 27.Lance ColemanC. Health beliefs and high risk sexual behaviors among HIV-Infected African American men. ApplNurs Res. 2007;20:110–5. doi: 10.1016/j.apnr.2007.04.003. [DOI] [PubMed] [Google Scholar]
- 28.Karimy M, Niknami SH, Amin Shokravi F, Shamsi M, Hatami A. The Relationship of Breast self-examination with Self-esteem and Perceived Benefits/Barriers of Self-efficacy in Health Volunteers of Zarandiehcity. Iran J Breast Dis. 2009;2:41–8. [Google Scholar]