

Abstract
Background:
Cardiovascular diseases (CVD) are the most common cause of mortality and morbidity in women. Intervention programs aimed at improving the lifestyle can reduce the incidence of these diseases and their factors. The purpose of this study was to evaluate the difference of the interventions impact on CVD risk factors and the women's physical and biochemical indicators based on education levels.
Materials and Methods:
As part of Isfahan Healthy Heart Program after identifying the status of women over the age of 18 and over five years, a large educational or environmental intervention was performed in different methodologies and in order to improve the lifestyle. Some organizations such as health care centers and the Literacy Campaign Organization have cooperated for low educated women. Demographic data and risk factors such as obesity, hypertension, diabetes and serum lipids were investigated and compared during the first and last phase. Data were entered in SPSS-15 software and were analyzed by using T-test in two independent samples, Chi-square test and Fisher exact test.
Results:
Findings of this study showed that performing the five years interventions could reduce physical and biochemical indexes such as nutrition, lipid profile, waist circumference and waist-to-hip ratio in both groups (P < 0.005). In the pre-intervention phase, 6391 subjects and after the intervention 4786 women participated. After Interventions, women with higher educational levels were showed significant decrease in Body Mass Index (BMI) (P = 0.01) and dyslipidemia (P = 0.02).
Conclusion:
The present study showed that the community-based interventions even in low-literate women could cause effective changes on improving lifestyle and CVD risk factors. Due to the greater impact of interventions in literate women, effective interventions should be considered in the society to decrease the prevalence of Non-Communicable Diseases (NCDs).
Keywords: Education level, lifestyle modification, literacy movement, risk factors, women
INTRODUCTION
Women in their midlife are facing with cardiovascular risk factors such as dyslipidemia, hypertension, obesity, smoking, diabetes and inactivity.[1] Despite the progress that has been made in diagnosis and treatment in obstetrics and gynecology diseases and attention to this fact that women's life expectancy is 10 years longer than men, but now ischemic heart disease is a major cause of mortality in women.[2] The study in Iran showed that the raw women's health education is lower than in men. This means that women are more vulnerable to the consequences of low health literacy. They may have less sense in written and verbal information provided by health professionals and act less according to the required methods and regulations.[3] On the other hand, women do not recognize the risk factors for cardiovascular disease or deny them. Besides, physicians, despite the extensive training conducted in the community, do not perform complete control of risk factors in women.[4] The performed interventions in the field of health promotion and controlling the risk factors are related to socioeconomic factors.[5] It seems that the education given to women regarding health and proper style of life varies due to differences in their socio-economic status. Education is perhaps the most important economic indicator, because it will not change with time after the adolescence the same as jobs and income. In addition, its information is easily accessible and classified and unlikely the adulthood health level would affect it.[6] Different strategies in low educated women show good and variable effect of their life style. The purpose of this study was to evaluate the impact of community-based trainings by Women Healthy Heart Program in the Literacy Movement Organization and health care centers on the correct style of life, risk factors for cardiovascular diseases and women's physical and biochemical factors according to their education level.
MATERIALS AND METHODS
The Women Healthy Heart Program was a part of the Isfahan Healthy Heart Program (IHHP). It was an interventional community-based study. This study was performed on all women over 18 years in Isfahan and Najaf Abad as the intervention cities and Arak as the control city. Inclusion criteria were having more than 18 years of age, non-pregnant, absence of hemorrhagic disease and mental retardation, Iranian nationality, and history of residing in the above cities for at least 10 years.[7] After performing the first phase, which was to assess the lifestyle and cardiovascular risk factors in women in 2002, lifestyle modification was performed by using different interventions including public education strategies, health personnel and intersectional collaboration between the women at the community level. In the final phase, after 5 years of intervention, the women's lifestyle and risk factors were re-examined in an independent sample. The annual evaluation studies were performed in the control city on the independent samples of women without any interventions. The interventions were conducted at literacy campaigns schools and health centers in the intervention cities. The method of choosing solutions was different in each organization. Initially the training contents based on literacy levels and age were prepared such as pamphlets, books and CD in various fields of the correct styles of living including healthy nutrition, physical activity, dealing with stress and the harmful effects of smoking. In this section, it was briefly described about the implementation method of the project in the interventions section. The project strategies and executive operations were set in three categories: Educational, environmental and legislation. Some examples of these interventions were as follows:
Educational: Such as women's education through group training sessions, face to face, educational pamphlets and books, training of trainers, providing appropriate models to increase regular physical activities at home, education of sport and physical activity in the family by using the training CD provided by this program
Environmental: Development of physical space available for the sport and physical activity of the women
Directive or legislation: Integration of classes associated with the healthy lifestyle in the pre-marriage training sessions at health care centers, development and integration of books prepared by the program in the literacy campaigns movement training classes.
The major interventions in Isfahan and Najaf Abad were as follows.
Educating the young women attending pre-marriage training classes in health care centers
This intervention was conducted by experts at the Provincial Health Center and health care centers for training of young couples before marriage. It has been provided with the necessary training for the prevention and control of non-communicable diseases (NCDs) to young couples in pre-marriage training classes. These classes were held every day of the week. Half an hour out of four hours of training for young couples was dedicated to a healthy lifestyle education. Thus, this intervention was well integrated into the system and there was no need to pay specific costs.
Training the trainers of literacy movement organization
It was the other target groups of the women project. Most of the learners were middle-aged women. In order to implement this intervention, initially the literacy trainers were trained with necessary trainings to transfer them to the literacy-learning women. Each year a workshop was held in 2 or 3 days (4 hours per day) for training the instructors and trainers of Literacy Movement Organization. The trainers had to transfer the trainings during the classes. On the other hand, a book was prepared entitled “healthy heart” for this group and it was used by the Literacy Movement Organization for training the learners. Therefore, the training was provided periodically during the academic year to the learners.
Training of the referred women to health care centers
Due to the large number of women who were referred to the health care centers for different services of family planning, childcare and vaccinations of their children, one of the effective ways to provide preventive education and control of non-communicable diseases and related risk factors was to use this situation and providing training to referred women to healthcare centers. This training was performed by technicians and experts of family health care centers. Besides face-to-face training, which was lasted for an average of 5 minutes, each week a class was held for one to two hours for group training of the women and during this class about 15 minutes was devoted to lifestyle modification. Other interventions were also conducted in this regard including distribution of posters, educational pamphlets and training to use the IVR (Interactive Voice Response) 149 to the referred women. It should be mentioned that the phone number of 149 (IVR system) is allocated for the provincial health authority and Isfahan Healthy Heart Program added a section to it entitled “Non-communicable diseases prevention and controlling these diseases”.
Along with the education of the women's in the society, more than six educational pamphlets were published and distributed in the community and the interventions’ workplaces. All women were asked to complete an informed consent form in order to be familiar with the procedures and requirements of the program. Afterwards, a demographic questionnaire was completed and the statuses of women's education levels were recorded. The variables were including nutrition, physical activity and the major risk factors (obesity, high blood pressure, smoking status, diabetes and high lipids). They were studied in the first and final phase. All women were classified based on completed academic years and were placed in two groups of 0-5 years and ≥6 years. Nutritional status was determined by a quantitative food frequency questionnaire and the global dietary index (GDI) was calculated. This questionnaire included the following: Weekly consumption data about seven food groups including number of consumption of prepared foods, fruits and vegetables, poultry, fish, beans and soy protein, sweets, fats, ghee and butter, red meat, full-fat milk, eggs and finally, the frequency of vegetable oil and olive oil consumption. Each food group was calculated based on its atrogenes role. The maximum score was two and the minimum was zero. Therefore, more GDI value was indicated higher atrogenes.[8]
Physical activity level was calculated based on the overall physical activity (TDPA: Total daily physical activity), which was included three physical activity categories of transport, leisure-time job and working at home based on the Mets unit per day.[9]
For physical examinations and biochemical tests in the first and final phases, the subjects were requested to refer to the desired centers after 12 hours of fasting. Initially, the following items were measured based on global standards: Blood pressure, weight, height, waist circumference and hip circumference.[10] Weight and height were measured without shoes by a trained person with light and thin clothes. Weight was measured by Seca scales made in Germany with 0.5 kg error. Height was measured with a plastic tape and error of 0.5 cm. Body Mass Index (BMI) was calculated based on weight (in kilograms) divided by squared stature (in meters). If the BMI was more than 30 kg per square meter or the waist-to-hip ratio was greater than 0.8, the subjects were considered as obese.[11] Waist circumference was measured at a standing position from the median interval between the last rib and the highest part of the pelvis, and the hip circumference from the femur bone area and then the ratio was calculated.[12] Blood pressure was measured by trained physicians and based on standard criteria after a five minutes rest, twice from the right arm and the mean values were recorded as the person's blood pressure. Hypertension was defined by the World Health Organization as the mean systolic blood pressure (SBP) greater than, or equal to 140 mmHg and diastolic blood pressure (DBP) greater than, or equal to 90 mm Hg or the drug use.[13] The blood samples were obtained from all women during this two-stage sampling. After the serum separation, biochemical tests were conducted at the Laboratory of Cardiovascular Research Center. Measured levels of total cholesterol (TC) and triglyceride (TG) were performed by the enzymatic method with Hitachi902 auto-analyzer. High-density cholesterol (HDL-C) was measured by heparin-manganese deposition technique.[14] Low-density cholesterol (LDL-C) was measured by specific kit[15] and if TG >400 mg/dl, LDL-C was calculated with the formula of Friedwald.[16] Individuals with dyslipidemia had the following conditions: Total cholesterol above 240 milligrams per deciliter, or LDL cholesterol above 160 milligrams per deciliter, or HDL cholesterol less than 50 mg per deciliter, or triglycerides more than 250 mg per deciliter.[17] Fasting blood sugar (FBS) was measured by the glucose oxidize enzymatic method. According to W.H.O. standard, individuals were considered diabetic who had a history of using hypoglycemic drugs or based on the American Diabetes Association criteria, had fasting blood glucose of ≥126 mg dl.[18] All of these projects were periodically under External Evaluation and Process.
Statistical analysis
All data were entered into SPSS-15 software and were analyzed by independent samples T-test, Chi-square and Fisher exact tests. All variables analyzed in 2001 and 2007 then effects and different between two times interventions were checked. P < 0.005 was significant.
RESULTS
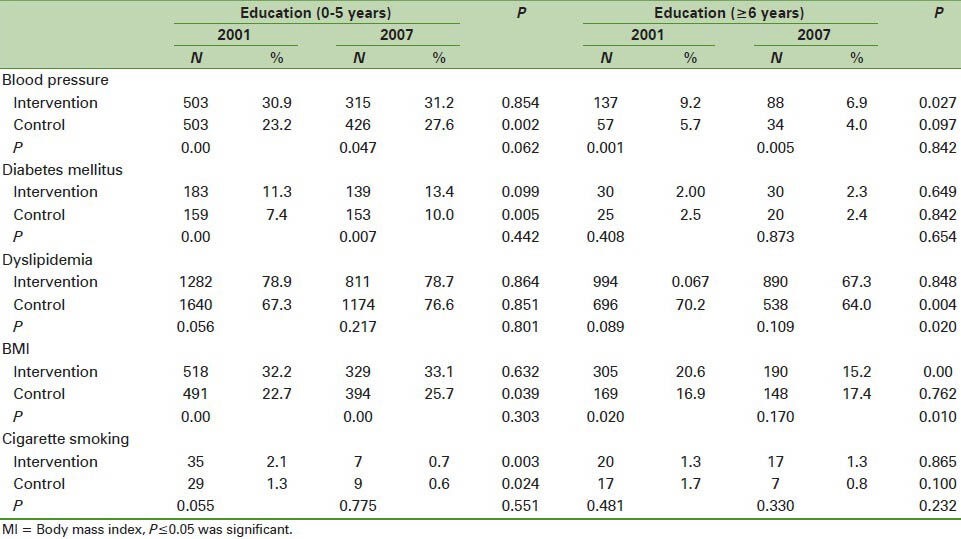
6391 women at the pre-intervention phase and 4786 women in the post-interventions phase were involved. Table 1 showed any significant different in diabetes mellitus after intervention in two groups of low and high educated. But different in blood pressure, BMI and cigarette smoking in high educated were significant after intervention (P < 0.05). Different in blood pressure, diabetes mellitus, BMI and cigarette smoking were statistically significant in control group in low educated women (P < 0.05).
Table 1.
Prevalence of cardiovascular disease risk factors based on the education level of women before and after the interventions
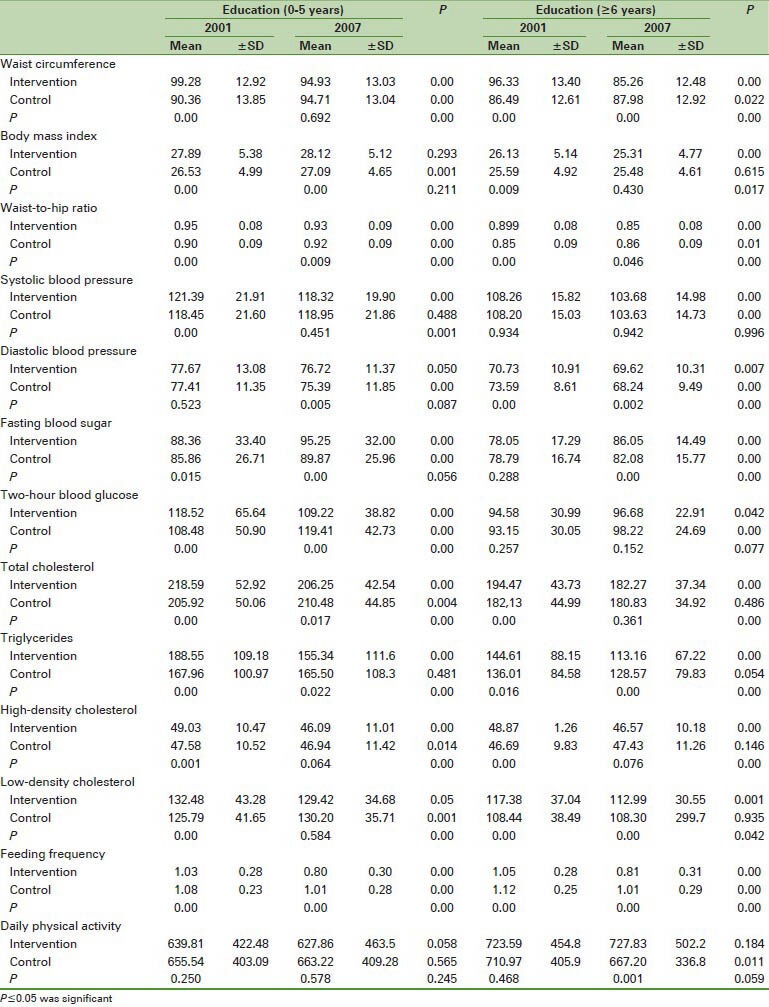
The mean and standard deviation of the following variables were listed in Table 2. They were included physical and biochemical variables, blood pressure, nutrition and physical activity and in women in both groups before and after intervention based on the number of years of education (0-5 years, and ≥6 years). As it could be seen and after further interventions, these variables have shown, significant differences in both groups, but the SBP and 2 hpp indexes in women with lower education (5-0 years) and variables of BMI, DBP and FBS in the second group of the women had significant statistical differences (P < 0.05).
Table 2.
Comparison of mean and standard deviation of physical and biochemical factors based on the education level
DISCUSSION
This paper showed effect of interventional program in illiteracy and low educated women that we saw limit studies in this regard. This study showed that community-based education has been able to change nutritional indicators, lipid profile (TC, TG, HDL-C and LDL-C), and Waist circumference and waist-to-hip ratio in both groups of women with different educational levels. In addition, significant changes were found in blood glucose, body mass index and diastolic blood pressure in women with higher education levels and systolic blood pressure and two-hour blood sugar on low literacy females. Although, the prevalence of cardiovascular disease risk factors had no remarkable difference between the two groups after the interventions, but BMI and dyslipidemia were decreased in women with higher education levels. Therefore, the changes were greater in the group with ≥6 years of education. As it was noted, education is an important socio-economic indicator. It does not change like jobs and income over passing the time and after adolescence. In addition, it is easily accessible and classified and does not affect the probability of the disease in the lifetime.[6] Several studies have investigated the relationship between education level and cardiovascular risk factors in both genders and the results were in line with the present study, so it could be noted that education had an impact on lifestyle and thus the influence on the prevalence and severity of cardiovascular risk factors.[19,20] Another study indicated a lower incidence of obesity, hypertension and lipid disorders in women with higher education, but there was no relationship with cigarette smoking. All of the men had greater prevalence of risk factors except the total cholesterol and LDL-C in those with a lower education level.[6] The study of Lee JR examined the relationship between education and CVD fatality among women with CVD. A significant interaction was found between education and age in predicting the mortality due to CVD. It stated that education levels in women with CVD independently from other conventional risk factors could be an important predictor of age-related mortality from CVD.[21] A study was conducted (2001-2006) and investigated the relationship between education and the 5 year incidence of cardiovascular events based on the clinical features and dietary habits in women and men. The survey results showed that there was a significant prevalence of hypertension, diabetes and dyslipidemia in subjects with lower education and they had more unhealthy eating habits comparing with people with higher education. Finally, in this study, after adjustment for age and gender roles, it was found that low education is positively related to the 5 year incidence of cardiovascular events.[22] A study from the Tehran Lipid and Glucose Study Series investigated the relationship between education levels and cardiovascular disease in men and women ≥45 years. It was inversely associated with the CVD risk in the raw models of women with higher educational levels. However, in the multivariate model, the risk of CVD decreased 39% in literacy levels less than diploma compared with illiteracy. This study in the support of developed countries showed that educational status along with other risk factors were inversely associated with CVD in a population of Iranian men and older women.[23] Another study from Tehran Lipid and Glucose Study Series has examined the education status on cardiovascular risk factors. The results of this study, in line with the present study, showed that by the increasing level of education, decreased the levels of BMI and WHR. It reported the prevalence of overweight and obesity in less educated and illiterate women. It also indicated that the triglycerides decreased in women with lower education levels but levels of HDL-C were increased.[24] The study of Sotoudeh and colleagues also showed that the pre-menopausal and post-menopausal women with higher education levels had a significantly lower prevalence of general obesity and Android. This lower incidence may be due to their higher nutritional knowledge.[25] The present study did not show any effects by physical activity interventions. Meanwhile, another study was performed at the workplace for the intervention and health promotion on physical activity, diet and smoking. It was shown that the interventions had been able to increase significantly the physical activity comparing with the control group. Fruits, vegetables and fiber intake were also increased in the intervention group, but there was no difference in fat intake and smoking in both groups.[26] This study did not provide a breakdown of gender and education level, but showed the positive impact of interventions in some aspects of nutrition in line with the present study. The other interventions that took place in Finland Carolina for controlling the risk factors of hypertension demonstrated that interventions for controlling and lowering blood pressure had a direct relationship with socio-economic status. Blood pressure was reduced further in those who had higher socio-economic status. However, in any socio-economic statuses, the interventions were effective and hypotension had occurred in all populations. These researchers have suggested that the risk control program should be conducted as community-based and regular in the entire community. Meanwhile, all of the population of the community would benefit differently from them.[5] A study that examined the trends of cigarette smoking in Korea (1999-2003) showed an increasing trend in cigarette smoking in the women.[27] Another evaluation was performed in the same country was found that cigarette smoking increased among women of 20-44 years old, but there was a decline in women older than 45 years old.[28] Another study showed that interventions for smoking cessation in the general media could positively influence the behavior of smoking and even bring down the prevalence of smoking. Time of presenting, their continuation and the amount of them through the mass media had an impact on the efficiency. The study also showed that the effectiveness of interventions for smoking cessation was not associated with age, gender, education and race in both men and women.[29] According to the lower consumption of cigarettes in our society comparing with the Western societies and the increasing trends of cigarette smoking by women, there was no significant difference in terms of active smokers.[30] In previous conducted studies, no study was found with particular attention to women interventions in terms of education levels. However, in general and by noticing to the sum of the current studies, it seems that the health-related requirements vary in literate, low literacy or illiterate women and the interventions need to be done according to their needs. In the present study, the interventions’ effectiveness was significantly more in women with higher education levels and may be preferred to design separate interventions for low-literacy women. Since the women constitute half of the society population and their health has a direct effect on the entire family, if the mother has healthy behaviors, the children will learn from her. It seems that it is required to continue ongoing programs and interventions to control the cardiovascular risk factors in the following ways: Informing by mass media (radio, television, newspapers and magazines), training the women in aggregation sites, encourage and motivate the women to raise awareness and literacy level, performing healthy nutrition programs for the families and creating mobility. Overall, community-based and regular interventions should be taken into account for different needs of women in order to have effective steps towards the health of the entire community.
Strength and limitation
Our strength was community based and large sample size in different part of our society. Limitation of this study was small number of referral of low educated women to literacy campaign and majority of women were home worker then we can access to them only by mass media.
ACKNOWLEDGEMENT
The authors appreciate and are grateful for the sincere cooperation of the Literacy Movement Organization staff and the involved healthcare centers and of the partners in Najaf Abad, Isfahan and Arak cities.
Footnotes
Source of Support: The study is part of the Isfahan Healthy Heart Program supported by Grant No. 31309304 from the Iranian Budget and Programming Organization in the Department of Health of the Ministry of Health and Medical Education, Isfahan Cardiovascular Research Center, and Isfahan Provincial Health Centre, both affiliated to the Isfahan University of Medical Sciences.
Conflict of Interest: None declared
REFERENCES
- 1.Vaskilampi T. Sociological aspects of community-based health intervention programmes. Rew Epidemiol Sante Publique. 1981;29:187–97. [PubMed] [Google Scholar]
- 2.Mark DB. Sex bias in cardiovascular care: Should women be treated more like men. JAMA. 2000;283:659–61. doi: 10.1001/jama.283.5.659. [DOI] [PubMed] [Google Scholar]
- 3.Tehrani BA, Amirkhani MA, Haghdoost AA, Alaviyan M, Asgharifard H, Baradaran H, et al. Health literacy in 5 province of Iran and effective etiology of it. Strides in Development of Medical Education. 2007;4:1–9. [Google Scholar]
- 4.Wong J, Wong SH. Trend in life style cardiovascular risk factor in women, analysis from the Canadian national publication healthy survey. Int J Nurs Stud. 2006;166:1196–202. doi: 10.1016/s0020-7489(01)00013-x. [DOI] [PubMed] [Google Scholar]
- 5.Nissinena A, Tumilehto Y, Salonen JT, Koltke TE, Piha T. The influence of socioeconomic factor on blood pressure control during a community-based hypertension control programme. Acta Cardiol. 1986;41:99–109. [PubMed] [Google Scholar]
- 6.Roohafza HR, Sadeghi M, Kelishadi R. Cardiovascular risk factors in Iranian adults according to educational levels: Isfahan healthy heart program. Asia Pac J Public Health. 2005;17:9–14. doi: 10.1177/101053950501700103. [DOI] [PubMed] [Google Scholar]
- 7.Sarraf-Zadegan N, Sadri G, Malek Afzali H, Baghaei M, Mohammadi Fard N, Shahrokhi S, et al. Isfahan Healthy Heart Program: A comprehensive integrated community-based program for cardiovascular disease prevention and control. Design, methods and initial experience Acta Cardiol. 2003;58:309–20. doi: 10.2143/AC.58.4.2005288. [DOI] [PubMed] [Google Scholar]
- 8.Mohammadifard N, Kelishadi R, Safavi M, Sarrafzadegan N, Sajadi F, Sadri GH, et al. Effect of a community-based intervention on nutritional behavior in a developing country setting: The Isfahan Healthy Heart Program. Public Health Nutr. 2009;12:1422–30. doi: 10.1017/S1368980008004230. [DOI] [PubMed] [Google Scholar]
- 9.Saidie M, Rabie K, Kelishadi R, Sadeghi M The association of leisure time physical activity, TV watching, obesity and lipid profile in an Iranian population. Pak J Med Sci. 2005;21:476–81. [Google Scholar]
- 10.WHO. Obesity: Preventing and Managing the Global Epideemic. Report of a Consultation. WHO Technical Report Series. 2000;(894) [PubMed] [Google Scholar]
- 11.National Institutes of Health. United States: NIH Publication; 2000. The practical guide identification, evaluation and treatment of overweigh and obesity in adults; p. 9. [Google Scholar]
- 12.Sadeghi M, Poormoghadas M, Roohafza HR, Talaei M, Golshadi I. The relationship between women physical fitness and obesity and the severity of CAD. J Qazvin Univ. 2008;12:46–53. [Google Scholar]
- 13.Lenfant CE, Chobanian AV, Jones DW, Roccela EJ. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC VII) Hypertension. 2003;41:1178–9. doi: 10.1161/01.HYP.0000075790.33892.AE. [DOI] [PubMed] [Google Scholar]
- 14.Warnick GR, Benderson J, Albers JJ. Dextran sulfate Mg2 + precipitation procedure for quantitation of high-density lipoprotein cholesterol. Clin Chem. 1982;28:1379–88. [PubMed] [Google Scholar]
- 15.Braunwald E, Zipes D, Libby P. Heart Disease. 6th ed. Philadelphia: WB Saunders Company; 2001. Risk factors for atherosclerotic disease; pp. 1010–65. [Google Scholar]
- 16.Friedewald WT, levy RI, Fredrickson DS. Estimation of the concentration of low density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. [PubMed] [Google Scholar]
- 17.Sadeghi M, Roohafza HR. Serum lipid distribution and prevalence of dislipidemia in urban and rural communities in Iran-IHHP study. Pakistan Journal of Cardiology. 2004;15(2):88–94. [Google Scholar]
- 18.Report of a WHO consultation, part 1: Diagnosis and Classification of Diabetes Mellitus. Geneva: WHO; 1999. World Health organization: Definition, Diagnosis and classification of Diabetes Mellitus and its Complication. [Google Scholar]
- 19.Potvin L, Richard L, Edwards AC. Knowledge of cardiovascular disease risk factors among the Canadian population: Relationships with indicators of socioeconomic status. Canadian Medical Association journal. 2000;162(9 Suppl):S5–11. [PMC free article] [PubMed] [Google Scholar]
- 20.Stelmach W, Kaczmarczyk-Chalas K, Bielecki W, Drygas W. How education, income, control over life and life style contribute to risk factors for cardiovascular disease among adults in a post-communist country. Public Health. 2005;119:498–508. doi: 10.1016/j.puhe.2004.09.006. [DOI] [PubMed] [Google Scholar]
- 21.Lee JR, Paultre F, Mosca L. The association between educational level and risk of cardiovascular disease fatality among women with cardiovascular disease. Womens Health Issues. 2005;15:80–8. doi: 10.1016/j.whi.2004.11.004. [DOI] [PubMed] [Google Scholar]
- 22.Panagiotakos DB, Pitsavos C, Chrysohoou C, Vlismas K, Skoumas Y, Palliou K, et al. The effect of clinical characteristics and dietary habits on the relationship between education status and 5 year incidence of cardiovascular disease: The ATTICA study. Eur J Nutr. 2008;47:258–65. doi: 10.1007/s00394-008-0720-0. [DOI] [PubMed] [Google Scholar]
- 23.Hajsheikholeslami F, Hatami M, Hadaegh F, Ghanbarian A, Azizi F. Association of educational status with cardiovascular disease: Teheran Lipid and Glucose Study. Int J Public Health. 2011;56:281–7. doi: 10.1007/s00038-010-0225-5. [DOI] [PubMed] [Google Scholar]
- 24.Mirmiran P, Mohammadi NF, Allahverdian S, Azizi F. Influence of educational level and marital status on dietary intake, obesity and other cardiovascular risk factors (Tehran Glucose and Lipid Study) J Shaheed Beheshti Univ Med Sci Health Serv. 2003;26:271–80. [Google Scholar]
- 25.Sotoudeh G, Niazi A, Khosravi SH, KhajehNasir F, Koohdany F. Population study of the prevalence of overweight, obesity and its associated factors in general and Android premenopausal and postmenopausal women. J Nurs Midwifery Tehran Univ Med Sci. 1389;16:54–47. [Google Scholar]
- 26.Emmons KM, Linnan LA, Shadel WG, Marcus B, Abrams DB. The Working Healthy Project: A worksite health-promotion trail targeting physical activity, diet and smoking. J Occup Environ Med. 1999;41:545–55. doi: 10.1097/00043764-199907000-00003. [DOI] [PubMed] [Google Scholar]
- 27.Cho HJ, Khang YH, Jun HJ, Kawachi I. Marital status and smoking in Korea: The influence of gender and age. Soc Sci Med. 2008;66:609–19. doi: 10.1016/j.socscimed.2007.10.005. [DOI] [PubMed] [Google Scholar]
- 28.Khang YH, Cho HJ. Socioeconomic inequality in cigarette smoking: Trends by gender, age, and socioeconomic position in South Korea, 1989-2003. Prev Med. 2006;42:415–22. doi: 10.1016/j.ypmed.2006.02.010. [DOI] [PubMed] [Google Scholar]
- 29.Bala MM, Strzeszynski L, Topor-Madry R, Cahill K. Mass media interventions for smoking cessation in adults. Cochrane Database Syst Rev. 2013 Jun 6;6:CD004704. doi: 10.1002/14651858.CD004704.pub3. [DOI] [PubMed] [Google Scholar]
- 30.Sadeghi M, Aghdak P, Motamedi N, Tavassoli A, Kelishadi R, Sarrafzadegan N. Do intervention strategies of women healthy heart project (WHHP) impact differently on working women and housewives? ARYA Atheroscler. 2011;6:129–35. [PMC free article] [PubMed] [Google Scholar]