

Abstract
Background:
Military hospitals are responsible for preserving, restoring and improving the health of not only armed forces, but also other people. According to the military organizations strategy, which is being a leader and pioneer in all areas, providing quality health services is one of the main goals of the military health care organizations. This study was aimed to evaluate the service quality of selected military hospitals in Iran based on the Joint Commission International (JCI) standards and comparing these hospitals with each other and ranking them using the analytic hierarchy process (AHP) technique in 2013.
Materials and Methods:
This was a cross-sectional and descriptive study conducted on five military hospitals, selected using the purposive sampling method, in 2013. Required data collected using checklists of accreditation standards and nominal group technique. AHP technique was used for prioritizing. Furthermore, Expert Choice 11.0 was used to analyze the collected data.
Results:
Among JCI standards, the standards of access to care and continuity of care (weight = 0.122), quality improvement and patient safety (weight = 0.121) and leadership and management (weight = 0.117) had the greatest importance, respectively. Furthermore, in the overall ranking, BGT (weight = 0.369), IHM (0.238), SAU (0.202), IHK (weight = 0.125) and SAB (weight = 0.066) ranked first to fifth, respectively.
Conclusion:
AHP is an appropriate technique for measuring the overall performance of hospitals and their quality of services. It is a holistic approach that takes all hospital processes into consideration. The results of the present study can be used to improve hospitals performance through identifying areas, which are in need of focus for quality improvement and selecting strategies to improve service quality.
Keywords: Accreditation, analytic hierarchy process technique (AHP), evaluation, Iran, Joint Commission International standards, military hospital, quality
INTRODUCTION
Success in the health care depends on the health care system as a whole. If patients do not have access to needed health care facilities, health care measures will fail. Furthermore, success in health care depends largely on health care providers. The main mission of hospitals is to provide quality care for patients and meeting their needs and expectations. Fulfilling this important mission requires the institutionalization of quality in hospitals and hence that each hospital member considers it as part of his/her duties and not as a separate task. The results of several studies on assessing the quality of hospital services and patients’ satisfaction with hospital care indicate that they face many challenges and failures. Therefore, the quality of hospital services should continuously be paid enough attention so that hospital administrators become aware of potential problems in various fields and try to solve them.[1,2,3,4,5,6]
Service quality management and measurement is vital and essential for healthcare organizations. Providing sufficient information on patients’ expectations and perceptions of service quality can help health care organization to identify factors affecting their competitive advantages and to prevent the waste of resources. It seems that raising the principles of quality in the health sector can improve the process of providing health care and provide patients’ satisfaction as a critical element in today's competitive world. Furthermore, it can be sure of the quality of services by evaluating their effectiveness.[7,8] Hence, most health care policymakers and managers consider providing standards-based services, evaluating performance, using the quality models and accrediting health care providers as essential and inevitable in order to improve the quality of services. On the other hand, in recent decades, a wave of evaluation and quality improvement models has influenced providing health services in most countries. All interest groups and stakeholders in the field of health, including policy makers, managers, health care providers, service recipients and insurance organizations are trying to improve health services provided and increase responsiveness to the community through performing accreditation of health care providers and assessing their services.[9,10,11,12,13]
Scope of the evaluation and assessment includes structure (including facilities, equipment, physical space, budget, human resources, etc.,) process (including management processes, diagnostic processes, treatment processes, support processes, etc.,) and outcome (including the patient's condition at discharge, patients’ readmissions, etc.).[14,15,16] In assessing health care services, some factors should be considered including service availability, accessibility, acceptability, comprehensiveness, costs and affordability.[17,18,19]
To measure the performance of hospitals, many methods have been proposed. World Health Organization has categorized the methods of measuring hospital performance into five groups: Forensic inspections, surveys of consumer experiences, evaluations carried out by a third party, statistical indices and internal evaluations.[20,21]
In 1996, European Commission established a 3 year project under expert project. One of the aims of this project was to identify and analyze different systems used in the Europe Union for improving independent external quality evaluation. The research group of Europe Union studied four main groups of standards that were more common in Europe, including health care accreditation, the International Organization for Standardization's (ISO) 9000 standards, the European Foundation for Quality Management (EFQM) Excellence Model and visitation or peer review-based schemes among which the accreditation standards are considered to be more specific for health care organizations than ISO and EFQM for Healthcare Organization standards.
Where there is a strong demand for commitment and transparency, accreditation can be selected as a means of government surveillance and supervision. The advantages of EFQM model are its simplicity and ease of application. It can be implemented at relatively low cost and has been experimented in various countries with some differences. In health care, EFQM model has been applied for operating standards of those specific areas of health care that are similar to the industry, such as clinical outcomes, employees and patients’ satisfaction, etc., Traditionally, the ISO standards are used as a way to ensure standardization of special products and functions (mainly documenting processes and management system). ISO standards are used more for the mechanical units, such as laboratory, radiology and transportation and are applied in all hospitals and clinics. The audit process is carried out according to the standards and does not have any aim of improving the organization.[22]
Accreditation is an independent and voluntary program, which was originated in the USA in 1917 by Joint Commission on Accreditation of Healthcare Organizations (JCAHO) to accredit and evaluate heath care provider organizations, such as hospitals. Its international branch, called the Joint Commission International (JCI), began in 1998 to assess the needs and develop a set of accreditation standards. The first edition of its international accreditation standards was released in 1999 and its first accreditation survey at the national level was conducted in November 1999. Currently, this program is the most complete and comprehensive accreditation program around the world. This institution has been established in response to the global interest in accreditation and quality improvement.[22,23,24]
Iranian Ministry of Health and Medical Education recently has developed and customized the national accreditation standards, derived from the Joint Commission's standards, for accrediting and evaluating hospitals. However, the results of studies on available challenges of Iran health system indicate that this sector is faced with some challenges, including the position of institution responsible for accreditation, legal basis, the lack of a proper and precise definition for accreditation process and the lack of a good mix of institutions participating in the accreditation process. The Ministry of Health's efforts in recent years has somewhat improved the available processes; however, there is a huge gap to access the full success.
Several studies have been conducted on accreditation and evaluation of health care organizations using JCAHO standards. Amerioun et al. evaluated a laboratory in a military hospital using JCI standards.[25] Khodayari et al. conducted a research to study and evaluate the readiness of selected hospitals of Tehran University of Medical Sciences to attract medical tourists.[26]
Furthermore, a study by Abbasi et al. in their study on the readiness of Isfahan selected hospitals for establishing JCI standards concluded that those hospitals’ readiness for establishing patient-centered standards was about 64% and for establishing organization-centered standards was about 66%.[27] Yousefian et al. in their study showed that the adaptation rate of the JCI standards to the Health Care Excellence Model in the studied hospitals was about 70%.[28] Furthermore, Ahmadi et al. in their study concluded that the adaptation rate of the Ministry of Health standards for hospitals to the JCI hospital accreditation standards was about 50%.[29] The results of another study (2013), also, indicated that medical equipment management according to the JCI standards resulted in patient safety.[30]
Military hospitals are responsible for preserving, restoring and improving the health of not only armed forces but also other people. In other words, these hospitals provide health services for all members of society. According to the military organizations strategy, which is being a leader and pioneer in all areas, providing quality health services is one of the main goals of the military health care organizations. Therefore, to achieve this goal, applying appropriate models of continuous quality improvement and measurement of service quality using national and international standards has become a main objective whereby health care organizations try to improve community health through identifying and eliminating their weaknesses. This study aimed to evaluate the service quality of selected military hospitals in Iran based on the JCI standards and comparing these hospitals with each other and ranking them using the analytic hierarchy process (AHP) technique in 2013.
MATERIALS AND METHODS
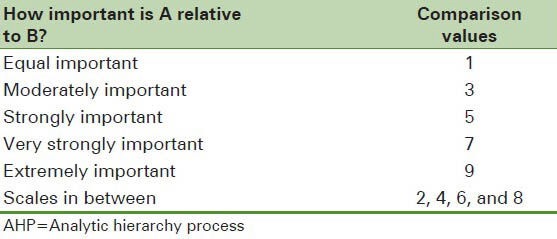
This was a cross-sectional and descriptive study conducted on 5 selected military hospitals in Iran in 2013. These 5 military hospitals, selected using purposive sampling method, were located in the provinces of Tehran, Khorasan Razavi, West Azerbaijan, Kermanshah and Hormozgan. Required data collected using checklists of accreditation standards, which were filled out through observations, interviews and document reviews. To determine the weights of studied criteria, a questionnaire was designed as a pair-wise comparison matrix based on the JCI standards. The validity of this questionnaire was confirmed by 6 experts. Furthermore, its reliability was approved (α = 0.85). The importance of each criterion was determined relative to other criterion on the basis of numerical paired comparison values whereby 9 referred to extremely important, 7 to very strongly important, 5 to strongly important, 3 to moderately important and 1 to equal important. 2, 4, 6 and 8 were considered as scales in between.
Then, this questionnaire was given to 48 experts in a meeting using nominal group technique. Nominal groups included eight groups each of which consisted of a physician, a nurse, a medical equipment expert, a construction and installation expert, an administrative and personnel issues expert and a health services management expert. These groups compared the criteria with each other as pair-wise comparisons and weighted them after detailed discussions. Studied hospitals were ranked by evaluation team using JCI checklists and according to the weight of each criterion. Expert Choice 11.0 was used to analyze the collected data. Standards included 13 areas in two separate sections:
Section I: Patient-centered standards, including
Access to care and continuity of care
Patient and family rights
Assessment of patient
Care of patient
Anesthesia and surgical care
Medication and management use
Patient and family education.
Section II: Management-centered standards, including
Quality improvement and patient safety
Prevention and control of infections
Leadership and management
Safety and facilities management
Staff qualifications and education
Management of communication and information.[27]
AHP technique was used for prioritizing. AHP technique, introduced by Thomas L. Saati in the 1970s, is one of the most widely used multi-criteria decision making techniques for solving unstructured problems in various fields such as management, politics, economics, social sciences, medicine, etc., AHP technique determines the weights of indices and prioritizes options. This technique provides a framework for group cooperation and collaboration in decision-making.
AHP is based on three principles, including
Drawing a hierarchical tree,
Setting priorities and
The logical consistency of judgments [Figure 1].
Figure 1.
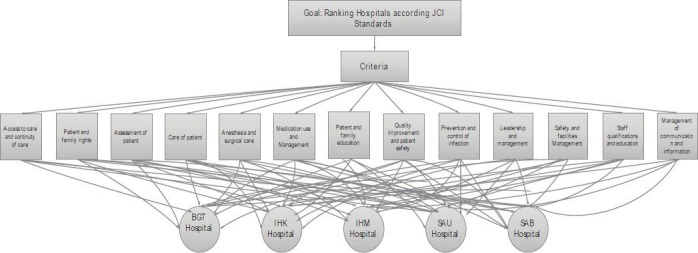
The overall performance of analytic hierarchy process technique (AHP)
In this technique, after determining options and criteria, they will be compared with each other as pair-wise comparisons. Then, the following algorithm will be followed:
Normalizing the pair-wise comparison matrix
Calculating arithmetic mean of each row of normalized pair-wise comparison matrix (relative weights)
Multiplying relative weights of indices by the arithmetic mean of options
Ranking and prioritizing options.
Afterwards, inconsistency rate is calculated. If inconsistency rate is less than or equal to 1, there is consistency in paired comparisons and the study can be continued. Otherwise, the decision maker should review and revise the paired comparisons.[31,32]
To fill out the pair-wise comparison matrix, scale of 1-9 is applied to determine the relative importance of each criterion in relation to the other criterion, according to the studied characteristics [Table 1].
Table 1.
AHP pair-wise comparison values
Five selected hospitals in this study were
A hospital located in Tehran Province: BGT
A hospital located in Khorasan Razavi Province: IHM
A hospital located in Kermanshah Province: IHK
A hospital located in West Azerbaijan Province: SAU
A hospital located in Hormozgan Province: SAB.
RESULTS
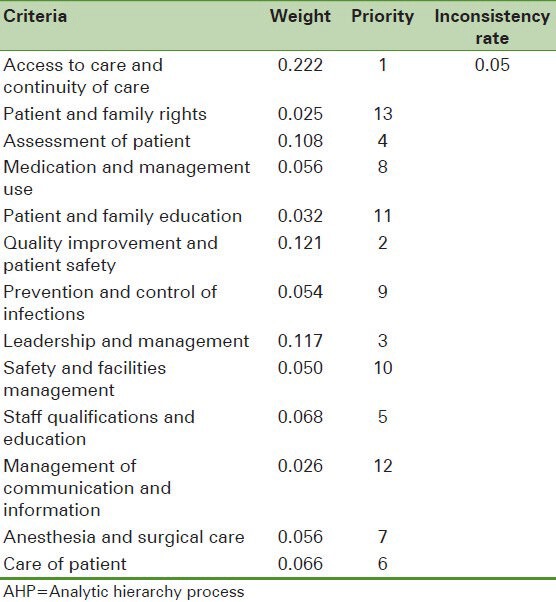
The results showed that among JCI standards, the standards of Access to care and continuity of care (weight = 0.122), Quality improvement and patient safety (weight = 0.121) and Leadership and Management (weight = 0.117) had the greatest importance, respectively [Table 2].
Table 2.
Ranking studied criteria using AHP technique
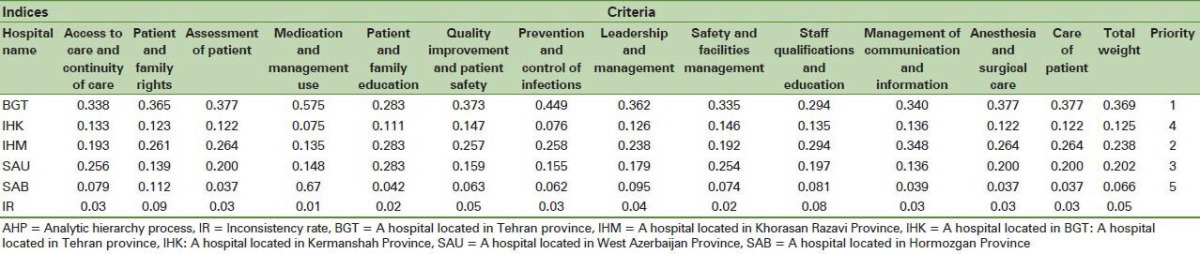
In the overall ranking, BGT (weight = 0.369), IHM (0.238), SAU (0.202), IHK (weight = 0.125) and SAB (weight = 0.066) ranked first to fifth, respectively. BGT ranked first according to all criteria, except management of communication and information. In terms of management of communication and information, IHM (weight = 0.348) ranked first. With regard to staff qualifications and education, IHM and BGT (weight = 0.294) were in the highest priority. BGT, IHM and SAU (weight = 0.283) had the same rank according to the standard of Patient and family education. The status of other criteria and their weights, as well as inconsistency rate has been shown in Table 3.
Table 3.
Ranking military hospitals using AHP technique
DISCUSSION
This study aimed to rank military hospitals in Iran according to the JCI standards using AHP technique. Measuring performance of military hospitals quantitatively is a difficult and complex process and during the last two decades, organizations have been faced with the challenge of how they can improve quality and patient safety.[33] Accreditation standards play an important role in improving quality and organizational culture, as well as in controlling costs.[34] In the present study, first, patient-and management-centered standards were weighted using pair-wise comparison matrix. Then, studied hospitals were compared with each other and their rankings were determined using AHP technique. Using this method, the performance of these hospitals in various fields, as well as, their overall performance was measured. This enables service recipients to have a good judgment about hospitals and choose the best one for receiving needed services accordingly.
Applying and meeting standards can improve patient care, increase patient satisfaction and finally, increase the organizational efficiency and effectiveness. The results of a study conducted in Egypt showed that patients’ satisfaction in hospitals that had met the accreditation standards was higher than others. In the U.S., hospitals are ranked and its results are published with the goal of providing the best care for patients by the hospitals.[35,36]
The results of the present study showed that among JCI standards, the standards of access to care and continuity of care, quality improvement and patient safety and leadership and management had the greatest importance. Access to care and continuity of care is a patient-centered standard and quality improvement and patient safety, as well as leadership and management are management-centered standards. Access to care and continuity of care is an important standard and patients should be admitted to hospital to receive required inpatient and out-patient services according to that hospital's missions and resources, as well as, patients’ identified needs. On the other hand, the hospital should plan and implement processes to provide continuous care to patients and inter-organizational coordination between health professionals and health staff. The standard of Access includes access, continuity of care, as well as appropriate discharge, referral and transfer of patients.[37]
The standard of quality improvement and patient safety is very important to the extent that it may can cause physical and biological hazards such as nosocomial infections, adverse events, medical errors and incorrect diagnoses and treatments.[38,39,40] One of the factors affecting the improvement of health systems quality and effectiveness is leadership and management which have been neglected in some countries, especially developing countries.[41]
Other JCI standards placed in the next rankings. These standards were Assessment of Patient, Staff qualifications and education, care of patient, Anesthesia and Surgical Care, Medication and management use, Prevention and control of infections, Safety and facilities Management, Patient and family education, management of communication and information and patient and family rights. The specific needs of all patients receiving health services are determined through performing certain assessment process. Furthermore, the use of medication is organized according to the regulations, as well as patients’ needs. Based on the JCI standards, hospitals should provide training programs to increase patients and their families’ participation in care and decision-making processes. Patient rights standards include the rights of patients and their families and giving informed consent.[37]
Given the importance of Anesthesia and surgical care, it has been considered as an area in the JCI standards indicating its important role in improving the quality of hospital services. Meeting the standards of this area is highly effective in preventing infections and implementing control programs.[42,43] Today, prevention and control of infections and addressing their related problems are considered as a major issue in patient safety. Therefore, some countries have developed strategies for improving patient safety by the standards of prevention and control of infections.[44] Another JCI standard is management of communication and information, which plays a great role in improving the quality of services.[45]
Furthermore, the current study results showed that among the studied hospitals, the hospital BGT had the best overall performance and quality of services and ranked first. Compared with other hospitals, this hospital achieved high score according to all criteria, except Management of communication and information. In terms of Management of communication and information, BGT was lower than IHM and higher than other hospitals. It can be due to that the Hospital Information System of IHM was better than that in BGT. BGT had high performance in establishing the JCI standards and its documentation had been done using scientific methods. After BGT, other hospitals including IHM, SAU, IHK, SAB ranked second to fifth, respectively. BGT and IHM had the same rank according to standard of Staff qualifications and education indicating that staff qualification test, training and empowering them were the main objectives of these hospitals and compared with other hospitals, had better performance in this regard. BGT, IHM and SAU had the same rank in Patient and family education and other hospitals placed in the next ranks. SAB achieved the lowest ranking according to all standards and was considerably different from other hospitals indicating that this hospital had made no serious attempt to establish the JCI standards and was far from its optimum condition. In terms of other criteria and standards, the hospital BGT, IHM, SAU, IHK and SAB ranked first to fifth, respectively.
Several studies conducted on ranking hospitals have been used different criteria and indices. In a study conducted in India, four hospitals were compared with each other using fuzzy AHP approach. In This study, SERVQUAL criteria had been used for assessing the quality of hospital services, which are different from criteria used in the present study. SERVQUAL model is not comprehensive enough and unlike the JCI standards, it cannot assess the quality of hospital services accurately[46] because the interpretation of patients’ perception of quality and quality services is difficult.[47]
In another study conducted in Canada, studied hospitals were ranked based on hospital mortality from acute myocardial infarction.[48] Lingsma et al. (2010) ranked 10 hospitals based on outcome standards. In this study, death or disability after 1 year had been defined as poor outcome.[49]
The results of another study showed that complications had a major role in the quality of hospital care.[50] Girotti et al. in their study concluded that the severity or number of complications should be considered in ranking hospitals.[51] In a research, studied hospitals were ranked according to the number of surgeries.[52] Also, the results of a study showed that ranking hospitals based on outcomes is unreliable.[53] Finally, in a study, the infection potential ranking of hospitals had been done based on producing biomedical wastes using fuzzy approach.[54]
The comparison of the present study results with those of other studies indicates that ranking hospitals only based on one or more criteria and indices is not enough and cannot provide a basis for reliable ranking of hospitals. In the present study, structure, process and outcome standards have been used for ranking studied hospitals; while in other studies, hospitals have mainly been ranked using only outcome standards.
CONCLUSION
Hospitals are trying to improve their performances and activities in order to increase service quality and patients’ satisfaction. Therefore, hospital managers and administrators can evaluate and improve their service delivery strategies through ranking and comparing their hospitals with other hospitals. AHP is an appropriate technique for measuring the overall performance and their quality of services. It is a holistic approach that takes all the hospital processes into consideration. Systems with good performance will have many benefits and advantages for patients and involves many incentives for health care providers to improve their service quality and reduce their costs.[55] The present study proposed a method for ranking studied military hospitals and assessing their quality of services.
The results of this study can be used to improve hospitals’ performance through identifying areas which are in need of focus for quality improvement, and selecting strategies to improve service quality.
ACKNOWLEDGMENT
We would like to thank the hospitals’ heads and staff for their kind cooperation with researchers in collecting and analyzing the data.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Altuntas S, Dereli T, Yilmaz MK. Multi-criteria decision making methods based weighted SERVQUAL scales to measure perceived service quality in hospitals: A case study from Turkey. Total Qual Manage Bus Excell. 2012;23:1379–95. [Google Scholar]
- 2.Amin M, Nasharuddin SZ. Hospital service quality and its effects on patient satisfaction and behavioural intention. Clin Gov. 2013;18:238–54. [Google Scholar]
- 3.Botje D, Klazinga NS, Wagner C. To what degree is the governance of Dutch hospitals orientated towards quality in care? Does this really affect performance? Health Policy. 2013;113:134–41. doi: 10.1016/j.healthpol.2013.07.015. [DOI] [PubMed] [Google Scholar]
- 4.Işik O, Tengilimolu D, Akbolat M. Measuring health care quality with the servqual method: A comparison in public and private hospitals. HealthMED. 2011;5(6 Suppl 1):1921–30. [Google Scholar]
- 5.Shen YC, Eggleston K. The effect of soft budget constraints on access and quality in hospital care. Int J Health Care Finance Econ. 2009;9:211–32. doi: 10.1007/s10754-009-9066-2. [DOI] [PubMed] [Google Scholar]
- 6.Zhao LP, Yu GP, Liu H, Ma XM, Wang J, Kong GL, et al. Control costs, enhance quality, and increase revenue in three top general public hospitals in Beijing, China. PLoS One. 2013;8:e72166. doi: 10.1371/journal.pone.0072166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Freeman T. Using performance indicators to improve health care quality in the public sector: A review of the literature. Health Serv Manage Res. 2002;15:126–37. doi: 10.1258/0951484021912897. [DOI] [PubMed] [Google Scholar]
- 8.Lazar EJ, Fleischut P, Regan BK. Quality measurement in healthcare. Annu Rev Med. 2013;64:485–96. doi: 10.1146/annurev-med-061511-135544. [DOI] [PubMed] [Google Scholar]
- 9.Ehrmeyer SS. Satisfying regulatory and accreditation requirements for quality control. Clin Lab Med. 2013;33:27–40. doi: 10.1016/j.cll.2012.11.007. [DOI] [PubMed] [Google Scholar]
- 10.Greenfield D, Braithwaite J. Health sector accreditation research: A systematic review. Int J Qual Health Care. 2008;20:172–83. doi: 10.1093/intqhc/mzn005. [DOI] [PubMed] [Google Scholar]
- 11.Meurer SJ, Rubio DM, Counte MA, Burroughs T. Development of a healthcare quality improvement measurement tool: Results of a content validity study. Hosp Top. 2002;80:7–13. doi: 10.1080/00185860209597989. [DOI] [PubMed] [Google Scholar]
- 12.Scrivens E. International trends in accreditation. Int J Health Plann Manage. 1995;10:165–81. doi: 10.1002/hpm.4740100303. [DOI] [PubMed] [Google Scholar]
- 13.Scrivens E. A taxonomy of the dimensions of accreditation systems. Soc Policy Adm. 1996;30:114–24. [Google Scholar]
- 14.Bilec MM, Geary M, Ries RJ, Needy KL, Cashion MK., III A method for quantifying the benefits of greening a healthcare facility. Eng Manage J. 2010;22:3–11. [Google Scholar]
- 15.Donabedian A. Quality assessment and assurance: Unity of purpose, diversity of means. Inquiry. 1988;25:173–92. [PubMed] [Google Scholar]
- 16.Rublee DA. The quality of care: How can it be assessed? The Journal of The American Medical Association (JAMA) 1988;260:1743–8. doi: 10.1001/jama.260.12.1743. [DOI] [PubMed] [Google Scholar]
- 17.Chaudhry M, Gauld R, Horsburgh S. Hospital quality-of-care performance measurement and reporting: What New Zealand can learn from the United States and United Kingdom. N Z Med J. 2012;125:51–63. [PubMed] [Google Scholar]
- 18.Kalogeropoulou M. Measurement of patient satisfaction: A method for improving hospital quality and effectiveness. Arch Hell Med. 2011;28:667–73. [Google Scholar]
- 19.Khan AM, Prasad PN, Rajamanoharane S. Service quality performance measurement management in corporate hospitals using analytical hierarchy process. Int J Manuf Technol Manage. 2012;26:196–212. [Google Scholar]
- 20.Bahadori M, Sadeghifar J, Hemouzadeh P, Hkimzadeh SM, Nejati M. Combining multiple indicators to assess hospital performance in Iran using the Pabon Lasso Model. Australas Med J. 2011;4:175–9. doi: 10.4066/AMJ.2011.620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bahadori M, Shams L, Sadeghifar J, Hamouzadeh P, Nejati M. Classification of health structural indicators using scalogram model in Golestan province, northern Iran. Iran J Public Health. 2012;41:58–65. [PMC free article] [PubMed] [Google Scholar]
- 22.Donahue KT, vanOstenberg P. Joint Commission International accreditation: Relationship to four models of evaluation. Int J Qual Health Care. 2000;12:243–6. doi: 10.1093/intqhc/12.3.243. [DOI] [PubMed] [Google Scholar]
- 23.Day SW, McKeon LM, Garcia J, Wilimas JA, Carty RM, de Alarcon P, et al. Use of Joint Commission International standards to evaluate and improve pediatric oncology nursing care in Guatemala. Pediatr Blood Cancer. 2013;60:810–5. doi: 10.1002/pbc.24318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kweon TD. Update of sedation in view of Joint Commission International standards. J Korean Med Assoc. 2011;54:1284–8. [Google Scholar]
- 25.Amerioun A, Tofighi SH, Mahdavi SM, Mamaghani H, Meskarpour Amiri M. Assessment of International Joint Commission (IJC) accreditation standard in a military hospital laboratory. J Mil Med. 2011;13:75–80. [Google Scholar]
- 26.Khodayari R, Tourani S, Qaderi A, Salehi M, Jafari H. Capabilities assessing of teaching hospitals in Iran University of medical sciences in attracting medical tourists according to JCI patient-oriented standards. Hospital. 2011;9:51–6. [Google Scholar]
- 27.Abbasi S, Tavakoli N, Moslehi M. Readiness of hospitals with quality management systems based on Joint Commission on accreditation standards. Health Inf Manag. 2012;9:512. [Google Scholar]
- 28.Yousefian S, Harat AT, Fathi M, Ravand M. A proposed adaptation of Joint commission international accreditation standards for hospital-JCI to the health care excellence model. Adv Environ Biol. 2013;7:956–67. [Google Scholar]
- 29.Ahmadi M, Khoshgam M, Mohammadpoor A. Comparative study of the Ministry of Health standards for hospitals with Joint Commission International hospital accreditation standards. Hakim Res J. 2008;10:45–52. [Google Scholar]
- 30.Huang J, Gao P, Guo E. The research of medical equipment management based on JCI standard. (2226-31).Appl Mech Mater. 2013:278–80. [Google Scholar]
- 31.Bahadori M, Babaei M, Mehrabian F. Prioritization factors influencing job motivation in employees of a military center using analysis hierarchy process (AHP) J Mil Med. 2013;14:237–244. [Google Scholar]
- 32.Bahadori M, Sadeghifar J, Ravangard R, Salimi M, Hakimzadeh SM. Factors affecting purchasing decisions of radiology equipment. Australas Med J. 2012;5:460–1. [Google Scholar]
- 33.Jovanovic B. Hospital accreditation as method for asssessing quality in health care. Arch Oncol. 2005;13:156. [Google Scholar]
- 34.van Ostenberg P. Joint Commission International (JCI): A partner in quality and safety. Jt Comm J Qual Patient Saf. 2004;30(Suppl 1):5–8. [Google Scholar]
- 35.Al Tehewy M, Salem B, Habil I, El Okda S. Evaluation of accreditation program in non-governmental organizations’ health units in Egypt: Short-term outcomes. Int J Qual Health Care. 2009;21:183–9. doi: 10.1093/intqhc/mzp014. [DOI] [PubMed] [Google Scholar]
- 36.Kamerow D. Quality rankings for US hospitals are released. BMJ. 2011;343:d6539. doi: 10.1136/bmj.d6539. [DOI] [PubMed] [Google Scholar]
- 37.JCI Standards. 2013. [Last cited on 2013 Sep 08]. Available from: http://www.jointcommissioninternational.org/./jcia/ias400_standards_lists_onl .
- 38.Bahrami MA, Montazeralfaraj R, Chalak M, Tafti AD, Tehrani GA, Ardakani SE. Patient safety culture challenges: Survey results of Iranian educational hospitals. Middle East J Sci Res. 2013;14:641–9. [Google Scholar]
- 39.Kalra J, Kalra N, Baniak N. Medical error, disclosure and patient safety: A global view of quality care. Clin Biochem. 2013;46:1161–9. doi: 10.1016/j.clinbiochem.2013.03.025. [DOI] [PubMed] [Google Scholar]
- 40.Taneva S. There is a need for a multidisciplinary approach to patient safety. Healthc Pap. 2013;13:30–5. doi: 10.12927/hcpap.2013.23340. 78. [DOI] [PubMed] [Google Scholar]
- 41.Pfeffermann G. Leadership and management quality: Key factors in effective health systems. World Hosp Health Serv. 2012;48:18–20. [PubMed] [Google Scholar]
- 42.Leaphart CL, Graham D, Pieper P, Celso BG, Tepas JJ., 3rd Surgical quality improvement: A simplified method to apply national standards to pediatric trauma care. J Pediatr Surg. 2009;44:156–9. doi: 10.1016/j.jpedsurg.2008.10.119. [DOI] [PubMed] [Google Scholar]
- 43.Lübbeke A, Hovaguimian F, Wickboldt N, Barea C, Clergue F, Hoffmeyer P, et al. Effectiveness of the surgical safety checklist in a high standard care environment. Med Care. 2013;51:425–9. doi: 10.1097/MLR.0b013e31828d1489. [DOI] [PubMed] [Google Scholar]
- 44.Cookson B, Mackenzie D, Coutinho AP, Russell I, Fabry J. Consensus standards and performance indicators for prevention and control of healthcare-associated infection in Europe. J Hosp Infect. 2011;79:260–4. doi: 10.1016/j.jhin.2011.07.008. [DOI] [PubMed] [Google Scholar]
- 45.Tekin M, Kilinç C. A study on the effects of information technologies and technology management on increasing the quality of service in hospitals. Int J Econ Perspect. 2010;4:331–40. [Google Scholar]
- 46.Sinimole KR. Performance evaluation of the hospital services-A fuzzy analytic hierarchy process model. Int J Productivity Qual Manage. 2012;10:112–30. [Google Scholar]
- 47.Manian FA, Gillman M, Spitznagel EL. A comparison between rankings of top hospitals by the U.S. News and World Report and the consumer reports patient ratings: Clarity or confusion for the empowered consumer? J Consum Health Internet. 2012;16:162–9. [Google Scholar]
- 48.Kosseim M, Mayo NE, Scott S, Hanley JA, Brophy J, Gagnon B, et al. Ranking hospitals according to acute myocardial infarction mortality: Should transfers be included? Med Care. 2006;44:664–70. doi: 10.1097/01.mlr.0000215848.87202.c7. [DOI] [PubMed] [Google Scholar]
- 49.Lingsma HF, Steyerberg EW, Eijkemans MJ, Dippel DW, Scholte Op, Reimer WJ, Van Houwelingen HC, et al. Comparing and ranking hospitals based on outcome: Results from The Netherlands Stroke Survey. QJM. 2010;103:99–108. doi: 10.1093/qjmed/hcp169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Williams S, Pauly MV, Rosenbaum PR, Ross R, Schwartz JS, Shpilsky A, et al. Ranking hospitals by the quality of care for medical conditions: The role of complications. Trans Am Clin Climatol Assoc. 1996;107:263–73. [PMC free article] [PubMed] [Google Scholar]
- 51.Girotti ME, Ko CY, Dimick JB. Hospital morbidity rankings and complication severity in vascular surgery. J Vasc Surg. 2013;57:158–64. doi: 10.1016/j.jvs.2012.06.099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Aikawa N. Hospital rankings by number of surgeries. Nihon Geka Gakkai Zasshi. 2005;106:411. [PubMed] [Google Scholar]
- 53.Ranstam J, Wagner P, Robertsson O, Lidgren L. Health-care quality registers: Outcome-orientated ranking of hospitals is unreliable. J Bone Joint Surg Br. 2008;90:1558–61. doi: 10.1302/0301-620X.90B12.21172. [DOI] [PubMed] [Google Scholar]
- 54.Bid SD, Mistry NJ. Infection potential ranking of hospitals based on generation of biomedical waste: A fuzzy approach. J Intell Fuzzy Syst. 2013;24:657–63. [Google Scholar]
- 55.Bes RE, van den Berg B. Ranking sources of hospital quality information for orthopedic surgery patients: Consequences for the system of managed competition. Patient. 2013;6:75–80. doi: 10.1007/s40271-013-0011-6. [DOI] [PubMed] [Google Scholar]