

Abstract
Introduction:
The purpose of this study was to determine the effectiveness of an educational program based on the Belief, Attitude, Subjective Norm, and Enabling Factors (BASNEF) Model on the nutritional behavior among second-grade, middle school, female students in Isfahan city.
Materials and Methods:
This quasi-experimental study was performed on 72 students. The samples were randomly divided in two groups (36 in the intervention group and 36 in the control group). The data collection tools were validated and had reliable questionnaires. For the intervention group, a 75-minute educational session was held thrice. The control group had no education. The BASNEF model constructs guided the development of the questionnaires and content of the educational sessions. The independent t-test and paired t-test were used to analyze the data. A two-tailed P value lower than 0.05 was considered to be statistically significant.
Result:
According to the results, the mean scores of knowledge and model variables (Belief, Attitude, Subjective Norm, and Enabling Factors) had a significant difference in the two groups after intervention (P < 0.001). On the basis of the findings, after educational intervention, 36.1% of the students had unfavorable nutritional behavior. In the control group, 88.9% of the students had unfavorable nutritional behavior, before and one month after intervention.
Conclusion:
The present study showed that nutrition education intervention based on the BASNEF model could promote the nutritional behavior in girl students.
Keywords: Belief, attitude, subjective norm, and enabling factors, education, knowledge, nutritional behavior
INTRODUCTION
Adolescence is one of the most important growth periods in humans.[1] Adolescents comprise of 20% of the world's population, 84% of whom are living in developing countries.[2] The physical and mental changes during this period are considered to be influential factors on the adolescent's dietary health,[3] and the demand for nutrients will increases remarkably during this period, because of body mass duplication.[4] Therefore, it is necessary to consider the dietary status of this group of society, as they undergo one of the most critical and important periods of growth and development, which if ignored, can cause some unfavorable consequences, such as loss of appetite or overeating, which may result in underweight or obesity.[5]
Malnutrition in children and adolescents as a health and economical problem, in developed and developing countries, has been noted.[6] Almost 70% of the children with malnutrition are living in Asia and the prevalence of underweight children is high, especially in the south of Asia.[7] The studies conducted on adolescents in our country show an unfavorable dietary status in this age group.[8,9,10,11] The Hazavehei study, conducted in four districts of Isfahan for this purpose, has indicated that 90% of the students have an unfavorable dietary function.[12] One of the contributing factors is lack of knowledge about favorable nutrition in adolescents.[13] For improving the unfavorable nutrition behaviors and increasing the knowledge in students, nutrition education can be very effective. The studies conducted in this field have indicated the effect that nutrition education has had on improving the nutrition behaviors in students.[14,15,16,17] It must be noted that the value of educational programs depends on the effectiveness of these programs, and the effectiveness of these programs depends on the use of theories and models.
It should be noted that the educational programs based on models are more effective than traditional training.
One of the models that is applied for studying and identifying behaviors and creating new behaviors is the BASNEF Model, which has been composed of a different structure, such as, beliefs (attitude toward behavior evaluation), attitude toward behavior, subjective norms, and enabling factors. The effectiveness of this model has been approved in many researches.[18,19,20,21]
For example, a study by Sharifirad showed that the BASNEF-based nutritional educational intervention improved dietary intake as well as glycemic control, three months after intervention.[22]
In the Khani Jeihooni study, the findings indicated that the mean scores of the BASNEF Model variables were significantly increased in the experimental group compared to the control group, after intervention. Applying the BASNEF Model is very effective in developing an educational program for diabetics.[23]
In another study by Roostaei, aimed at nutritional and exercise behaviors, showed that using the BASNEF model as an intervention in the elderly led to increased knowledge, attitude, and intent of act intention about nutrition in them.[24] But, researchers can’t find similar study by using of BASNEF model about nutrition in student.
Considering the unfavorable nutritional behaviors among students and the effect of nutrition education on its reduction and the importance of using the BASNEF Model, the present study was conducted to determine the effectiveness of the educational program, based on the BASNEF model, on the nutritional behaviors among second-grade, middle school, female students in Isfahan city.
MATERIALS AND METHODS
This is a quasi-experimental study conducted in Isfahan (Iran) in 2008, on second-grade, middle school, female students (72 students) from two public schools located at district 4 of the Esfahan Education Department. From five districts of the Education Departments, district 4 was selected randomly, and among the female public middle schools, two schools were chosen, and from each school, two classes, each of which consisted of 36 students, were selected randomly and were assigned to two control and intervention groups.
Two questionnaires were used, one of which was designed based on the BASNEF Model and 24-hour food recall. The questionnaire had three sections: Knowledge (22 questions), BASNEF Model (31), including six questions on attitude toward behavior evaluation, six questions on attitude toward behavior, five questions on belief norms, four questions on subjective norms, five questions on enabling factors, and five questions on behavior intention, which were completed twice before intervention and one month after intervention, in a self-administered format, and 24-hour food recall was completed in three days (two usual days and one holiday) by the interview method.
Content validity was established by five experts, who were health educators and nutritionists. The reliability of the questionnaire was determined by Cronbach's alpha (range, 0.7-0.82).
The Likert scoring method was used to assess the answers as follows: (certainly agree = 4, agree = 3, no idea = 2, disagree = 1, and certainly disagree = 0) and the score range for every section was 0 to 100.
For the knowledge section, one score was given to each correct answer. The score for wrong answers was zero.
Prior to the educational intervention in both groups, the questionnaires were completed and then educational intervention was performed for the intervention group in three educational sessions, (two sessions for students and one session for their mothers), the duration of which was 75 minutes, and pamphlets and a booklet were given to the students after each educational session.
In the first session, the health educator informed them about favorable nutrition behavior and the importance of nutrition behavior in puberty, and tried to promote the attitude toward behavior in the students by group discussion. In the second session, the health educators held group discussions to familiarize the belief norms and subjective norms. In the third session, the specialist, using the food pyramid, tried to educate the students about the five food groups for reforming nutritional behavior. Finally, their mothers were informed about the food pyramid and the necessity for a proper nutritional behavior in students. The students in both groups were intimated in detail about the study and were asked to read and sign a consent form.
Keeping this in view, the number of consumed units for each group was extracted from a 24-hour nutrition record and then the following actions were performed.
Ten scores were devoted to the nutrition group, whose minimum recommended unit number by its pyramid had been supplied. In case no unit was consumed in the nutrition group, a score of zero (0) was denoted. For an amount that was lower than the minimum recommended unit number by its pyramid, the proportion of consumed units was divided by the number of recommended units and multiplied by 10. If a student had consumed the minimum recommended units from each nutrition group, she obtained two scores, which totally became 50 for five groups, of this score. Also the scores were related to the nutrition variety, which totally reached 60 scores, and ultimately if the function of the dietary regime was wonderful the score was equal to 60, if the efficiency and dietary regime was favorable the score was equal to 50-59 scores, and if the dietary regime was unfavorable the score was equal to<50.
Statistical analysis was performed using SPSS (version 18). Comparison between the two groups was done by the independent t-test. Paired t-test analysis was used for comparison in one group before and after intervention. A two-tailed P value lower than 0.05 was considered statistically significant.
RESULTS
A total of 72 students entered the study. The mean and standard deviation of the participants age was 13.03 ± 0.69 years [Table 1].
Table 1.
Frequency of demographic factors in participants before intervention
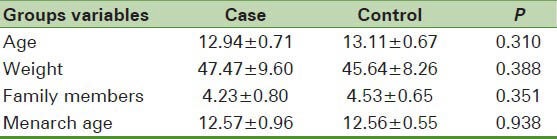
There was no significant difference between fathers and mothers jobs (P = 0.531, P = 0.082), and education level (P = 0.448, P = 0.696) in two groups.
The mean scores of knowledge in the intervention group before and after intervention were 49.76 ± 16.83 and 93.06 ± 5.92, respectively. There was no significant difference between the mean score of knowledge in the two groups (P = 0.263).
The paired t-test showed that the mean score of knowledge had increased significantly one month after intervention (P < 0.001) and there was a significant difference between the two groups.
The independent t-test showed that there was no significant difference between the mean scores of attitude toward behavior evaluation in the two groups before intervention (P = 0.779), while the above difference became significant one month after intervention (P < 0.001). There was no significant difference between the mean of attitude toward behavior in the two groups before and one month after intervention [Table 2].
Table 2.
Mean±SD of grades of constructs of the BASNEF model in participants before and after intervention
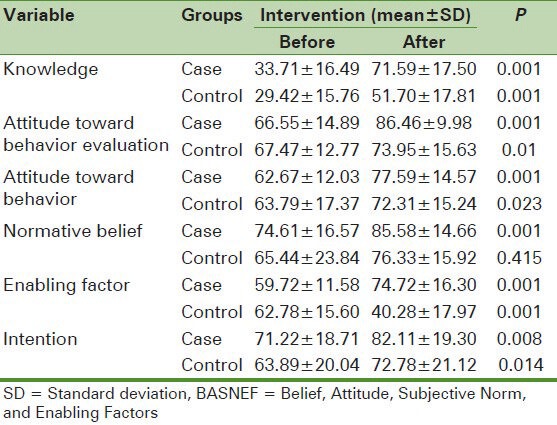
The mean scores of normative beliefs showed no significant difference in the two groups, before intervention, but one month after intervention the mean scores of normative beliefs were significantly higher in the intervention group than in the control group (P = 0.012) [Table 2].
The independent t-test showed that there was no significant difference before educational intervention between the mean score of enabling factors and intention in the two groups (P = 0.349, P = 0.113), but this difference became significant one month after intervention [Table 2].
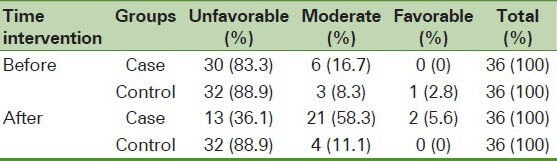
Regarding the nutritional behavior, before intervention, 83.3% of the students had unfavorable nutritional behavior, but after educational intervention their behavior was favorable by 36.1%. In the control group, 88.9% of the students had unfavorable nutritional behavior before and one month after intervention [Table 3].
Table 3.
Frequency of nutritional behavior in participants before and after intervention
DISCUSSION
The mean score of knowledge in the intervention group had a significant increase compared to the control group, one month after intervention, which was indicative of the effect of intervention on improving the students’ knowledge. This result was consistent with the other studies.[14,16,25]
According to the findings, the mean of the knowledge score in the control group had increased. We suspected that this was due to the students’ curiosity, which was a result of their answering the questionnaire and looking for correct answers from their parents and teachers. This was similar to the result of Vakili's study.[26]
Following the intervention the mean score of attitude toward behavior evaluation had increased in the intervention group. This significant difference indicated that educational intervention based on the BASNEF model encouraged the student to have a positive attitude. These findings were consistent with other studies.[20]
One month after intervention the attitude toward evaluation of behavior had increased in the control group. It seemed that increasing the knowledge on nutritional behavior in students and the consideration of the parents and teachers were the causes of this increase.
The paired t-test showed that one month after intervention the attitude toward evaluation of behavior in the control group had increased; the reason for which could be attributed to the increase of knowledge in this group, as also the consideration of parents and teachers to nutritional behaviors in students, which was influential in this respect. This result supports the findings of the Kohzadi study.[27]
Before intervention the mean score of the attitude toward nutritional behavior in the two groups has been high, the reason for which can be attributed to a high attitude toward evaluation of behavior in both the groups. As it is shown in the BASNEF model, evaluation of the behavior results is before intention. When students get a positive evaluation from the results for behavior (favorable nutritional behavior), this factor itself creates a motivation in the students toward better nutritional behavior. This findings shows that the education must be designed to motivate an individual toward favorable nutrition and he/she must understand the helpful results of favorable nutritional behavior, so that their intention toward favorable nutritional behavior is increased.[18,28]
This finding is consistent with other studies.[14,18,28,29]
There is no significant difference in normative beliefs in the two groups before educational intervention in this study, although the mean score of normative beliefs one month after educational intervention has increased significantly in the intervention group. This increase is the result of the educational intervention based on the BASNEF Model in the intervention group and also involvement of their mothers.
Various studies show that in most cases, involvement of the family (especially mothers,[27] friends, peers[29] and daughters of the family)[18] in the educational intervention is effective, such as, in the subjective norms.
These results indicated that the behavior intention in both groups had increased, which could be attributed to other constructs of the model, such as, attitude toward behavior evaluation and attitude toward behavior and normative beliefs. As it was seen in the BASNEF model, these constructs had an effect on intention. These results support the findings of many other studies conducted on these variables.[18,28,30] This finding is consistent with Hazavehei's finding in relation to the BASNEF model.[12]
This study reveals the significant increase in intention as a result of educational intervention in intervention group, which was also proved in other studies.[20,32,33]
Increase in the mean scores of the enabling factors after education in the intervention group is due to the following:
Student's access to educational classes, pamphlets, and an educational booklet
Student's access to the necessary foods provided by the family, especially mothers
Lack of student's access to unhealthy foods through the school's food buffet.
The enabling factors could affect attitude change, this result was consistent with the Mohamaei and Baghiani-Moghadam studies.[19,34] In the mentioned studies, the scores of the enabling factors were significantly improved after intervention, in the intervention group. The increase in the enabling factors was similar to the result of other studies.[33,35]
In the control group also, the mean score of the enabling factors had decreased. Certainly one of the reasons for the decrease was the knowledge on nutrition obtained by the students and the parents’ and teachers’ attention to this subject (favorable nutrition behavior), who felt the necessity to access the enabling factors. These findings were supported by Taghdisi's study as well.[35]
The effect of education with regard to the increase in the mean score of attitude toward behavior evaluation, attitude toward behavior, normative beliefs, behavior intention, and enabling factors has caused behavior improvement in the intervention group. Before intervention 83.3% of the students’ behavior had been unfavorable, but reached 36.1% after intervention; and in the control group, 88.9% of the students had unfavorable nutrition function before and one month after intervention. One month after education, there was an increase in consuming many of the foods in the group of nutrition (milk and milk products, fruits, vegetables, meat and protein foodstuff) in the intervention group, which showed the effect of education on consuming these foods, which was consistent with other studies in the field of nutritional education.[15,17,36]
The study was limited to students in district 4 only. This study was done in twice (before and one month after intervention), which showed only short-term effects of the intervention.
Thus, further research must have participants from different districts and their behavior must be followed for a long time.
CONCLUSION
The present study showed that nutrition education intervention based on the BASNEF model can promote nutrition behaviors in students.
ACKNOWLEDGMENT
The authors would like to thank the manager of schools and students who willingly participated in the study
Footnotes
Source (s) of support: This study was sponsored by Isfahan University of Medical Sciences, the grant code was 388082
Conflict Interest: Nil
REFERENCES
- 1.Spear BA. Nutrition in adolescent. In: Mahan LK, Esco H-Stump S, editors. Krause's Food, Nutrition and Diet Therapy. Philadelphia: WB Saunders; 2000. [Google Scholar]
- 2.Garrow JS, James WP, Ralph A. 10th ed. London: Churchill and Livingstone; 2000. Human nutrition and dietetics. [Google Scholar]
- 3.Mary S, Micheal DR. Adolescents views on food and nutrition. J Nutr Educ. 1986;18:188–92. [Google Scholar]
- 4.Morgan LS, Weinsier R. Osoole taghziyeye balini. In: Kimyagar M, Fallahi E, translators. 1st ed. Tehran: Poorsina; 2002. [Google Scholar]
- 5.Azadbakht M, Mirmiran P. Tehran: Tabib; 2003. Tanzime barnameye ghazaei dar dorehaye mokhtalefe zendegi. [Google Scholar]
- 6.Popkin BM. Nutrition in transition: The changing global nutrition challenge. Asia Pac J Clin Nutr. 2001;10(Suppl):S13–8. [PubMed] [Google Scholar]
- 7.Khor GL. Update on the prevalence of malnutrition among children in Asia. Nepal Med Coll J. 2003;5:113–22. [PubMed] [Google Scholar]
- 8.Doost Mohammadian A, Keshavarz A, Dorosty A, Mahmoodi M, Sadrzadeh Yeganeh H. The relationship between some food factors with the weight status of high of high school adolescent girls in Semnan, 2004. Iran J Nutr Sci Food Technol. 2007;1:51–6. [Google Scholar]
- 9.Salmani Barough N, Pashaeypour Sh, Rezaiepour A, Kazemnejad A. Study of quality of snacking in adolescents (12-18 years old) Hayat. 2007;12:21–9. [Google Scholar]
- 10.Jafari S, Keshavarz A, Dorosty AR. Factors associated with the nutritional status of adolescent girls based on body mass index in Sari. Iran J Nutr Sci Food Technol. 2007;2:51–6. [Google Scholar]
- 11.Alavi Naeini AM, Jazayeri A, Chamari M, Hamedi S. Comparison of the nutritional status of adolescentgirls in the secondary schools of two educational districts of Kerman. Payesh. 2008;7:287–93. [Google Scholar]
- 12.Hazavehei MM, Pirzadeh A, Entezari MH, Hasanzade A, Bahraynian N. Investigating the Knowledge, Attitude and Nutritional Practice of Female Middle School Second Graders in Isfahan in 2008. Knowl Health J. 2009;4:24–7. [Google Scholar]
- 13.Pei-Lin H. Factors influencing students’ decisions to choose healthy or unhealthy snacks at the University of Newcastle, Australia. J Nurs Res. 2004;12:83–91. doi: 10.1097/01.jnr.0000387492.16804.a3. [DOI] [PubMed] [Google Scholar]
- 14.Zalilah MS, Siti Sabariah B, Norlijah O, Normah H, Maznah I, Zubaidah J, et al. Nutrition education intervention improves nutrition knowledge, attitude and practices of primary school children: A pilot study. Int Electron J Health Educ. 2008;11:119–32. [Google Scholar]
- 15.Friel S, Kelleher C, Campbell P, Nolan G. Evaluation of the Nutrition Education at Primary School (NEAPS) programme. Public Health Nutr. 1999;2:549–55. doi: 10.1017/s1368980099000737. [DOI] [PubMed] [Google Scholar]
- 16.Powers AR, Struempler BJ, Guarino A, Parmer SM. Effects of a nutrition education program on the dietary behavior and nutrition knowledge of second-grade and third-grade students. J Sch Health. 2005;75:129–33. [PubMed] [Google Scholar]
- 17.Piperakis SM, Sotiriou A, Georgiou E, Thanou A. Understanding nutrition: A study or greek primary school children habits, before and after classroom nutrition intervention. J Sci Educ Technol. 2004;13:129–36. [Google Scholar]
- 18.Baghianimoghadam MH, Rahaee Z, Morowatisharifabad MA, Sharifirad G, Andishmand A, Azadbakht L. Effects of education on self-monitoring of blood pressure based on BASNEF model in hypertensive patients. J Res Med Sci. 2010;15:70–7. [PMC free article] [PubMed] [Google Scholar]
- 19.Baghyani-Moghadam MH, Shafiei F, Haydarneia AR, Afkhami M. Efficacy of BASNEF model in controlling of diabetic patients in the city of Yazd, Iran. Indian J Community Med. 2005;30:10–2. [Google Scholar]
- 20.Hazavehei MM, Khani Jyhouni A, Hasanzade A, Rashidi M. The effect of educational program based on BASNEF model on diabetic (type II) eyes care in Kazemis clinic (Shiraz) Indian Journal of Endocrinology and Metabolism. 2006;10:145–54. [Google Scholar]
- 21.Khalaj M, Mohammadi Zeidi E. Health education effects on nutritional behavior modification in primary school students in Ghazvin. J Shahrekord Univ Med Sci. 2006;8:41–9. [Google Scholar]
- 22.Sharifirad Gh, Najimi A, Hassanzadeh A, Azadbakht L. Application of BASNEF educational model for nutritional education among elderly patients with type 2 diabetes: Improving the glycemic control. J Res Med Sci. 2011;16:1149–58. [PMC free article] [PubMed] [Google Scholar]
- 23.Khani Jeihooni A, Kashfi SM, Hazavehei SM. Effects of the BASNEF model-based educational programs on blood sugar control, (Type 2 Diabetes) Health Educ Health Promot. 2013;1:33–49. [Google Scholar]
- 24.Roostaei Patapeh S. Tehran (Iran): Tehran University of Medical Sciences, School of Nursing; 2013. Assessing the effect of lifestyle education based on BASNEF model on nutritional and exercise behaviors in the elderly [MS Thesis] [Google Scholar]
- 25.Jeffrey CL, Danielle RP, Volpe SL. Effect of nutrition supplement education on nutrition supplement knowledge among high school students from a low- income community. J Community Health. 2002;27:25–35. doi: 10.1023/a:1020653202522. [DOI] [PubMed] [Google Scholar]
- 26.Vakili M, Baghiani- Moghadam MH, Pirzadeh A, Dehghani M. Assessing the effect of education on knowledge, attitude and practice of guidance school students about milk and dairy products. Knowl Health J. 2008;2:39–43. [Google Scholar]
- 27.Kohzadi K. Tehran (Iran): Tehran University of Medical Sciences, School of Health; 2005. The effect of educational program based on BASNEF Model on the knowledge, attitude and practice among first grade middle school students in Bane city about dental health [MS Thesis] [Google Scholar]
- 28.Hazavehei MM, Asadi Z, Hassanzadeh A, Shekarchizadeh P. Comparing the effect of two methods of presenting physical education P course on the attitudes and practices of female students towards regular physical activity in Isfahan University of Medical Sciences. J Med Educ. 2008;8:121–30. [Google Scholar]
- 29.Taslimi Taleghani M, Djazayeri SA, Keshavarz SA, Sadrzadeh Yeganeh H, Rahimi A. Comparison of the effectiveness of two nutrition education methods on the nutritional knowledge, attitude and practice of first-grade school girl students. Tehran Univ Med Sci J. 2004;2:69–78. [Google Scholar]
- 30.Salehi M, Kimiagar SM, Shahbazi M, Mehrabi Y, Kolahi AA. Assessing the impact of nutrition education on growth indices of Iranian nomadic children: An application of a modified beliefs, attitudes, subjective – norms and enabling – factors model. Br J Nutr. 2004;91:779–87. doi: 10.1079/BJN20041099. [DOI] [PubMed] [Google Scholar]
- 31.Manios Y, Kafas A. Health and nutrition education in elementary schools: Changes in health knowledge, nutrition intakes and physical activity over a six year period. Public Health Nutr. 1999;2:445–8. doi: 10.1017/s1368980099000610. [DOI] [PubMed] [Google Scholar]
- 32.Barati M. Isfahan (Iran): Isfahan University of Medical Sciences, School of Health; 2007. The effect of educational program based on BASNEF model on pregnant women breastfeeding behavior in Arak city [MS Thesis] [Google Scholar]
- 33.Alizadeh R. Tehran (Iran): Tehran University of Medical Sciences, School of Health; 2007. Safety culture educational intervention study using the model of BASNEF promote the production staff of a petrochemical complex Kimia Bandar Mahshahr safe city in 2005 [MS Thesis] [Google Scholar]
- 34.Mohamaei F, Nouri Tajer M, Noohi F, Maleki M. Application of BASNEF health belief model in preventing the occurrence of risk factors contributing to myocardial infarction in patients with coronary artery disease. Iran Heart J. 2004;5:29–32. [Google Scholar]
- 35.Taghdisi MH, Madadzadeh N, Shadzi S, Hasanzadeh A. Effect of education interventions on the coke workers immune performances on BASNEF model basis at Isfahan melting factory 2005. journal of Ilam university of medical sciences. 2008;16:20–9. [Google Scholar]
- 36.Turnin MC, Tauber MT, Couvaraso O, Jouret B, Bolzonella C, Bourgeois O, et al. Evaluation of microcomputer nutritional teaching games In 1,876 children at school. Diabetes Metab. 2001;27:459–64. [PubMed] [Google Scholar]