

Abstract
Compression of the ulnar nerve in Guyon’s canal is an uncommon phenomenon. Reports of ulnar nerve palsy secondary to ulnar artery pseudoaneurysm at this anatomical location are very rare and equivalent pathology just distal to this site is unheard of. Here we present such a case, which featured a delayed onset of symptoms. This followed penetrating trauma to the hand. Our methods for diagnosis, operative planning and surgical treatment are included.
Keywords: Pseudoaneurysm, Ulnar, Guyon’s
Compression of the ulnar nerve in Guyon’s canal is an uncommon phenomenon, described as early as 1908 by Hunt. 1 Reports of ulnar nerve palsy secondary to ulnar artery pseudoaneurysm at this anatomical location are very rare.
Case history
A 33-year-old man presented to our clinic 3 weeks after a penetrating glass laceration to the hypothenar eminence of his non-dominant right hand. He had attended casualty at the time of his injury while on holiday abroad where the wound was treated with adhesive strips. He reported that there were no functional problems with the hand at the time of the injury but motor and sensory symptoms developed progressively over the subsequent weeks.
At the time of our assessment, ulnar clawing of the hand was apparent; the ring and little metacarpophalangeal joints were held in hyperextension with flexion at the interphalangeal joints of the corresponding fingers. Clinically, a sensory deficit was apparent (light touch, 2 point discrimination) in a well demarcated medial one and a half digit ulnar distribution. There was weakness of the interosseous muscles, abductor digiti minimi and lumbricals to the ring and little fingers (Medical Research Council score 3/5). Froment’s sign was positive. A pulsatile mass was palpable over the hypothenar eminence. A clinical diagnosis of pseudoaneurysm of the ulnar artery causing neurapraxia of the ulnar nerve was made. The patient underwent ultrasonography and magnetic resonance angiography provided further clarity, demonstrating a pseudoaneurysm measuring 24mm of the ulnar artery as it coursed into the palm, immediately prior to its continuation as the superficial palmar arch (Fig 1).
Figure 1.
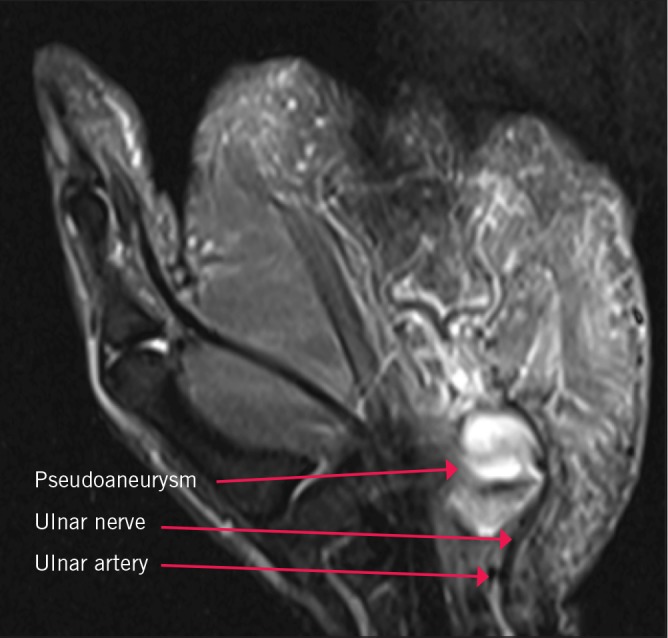
Magnetic resonance angiography showing anatomical boundaries of pseudoaneurysm
There was no evidence of ulnar nerve transection. Maximal ulnar nerve compression was at a site just distal and medial to the apex of the hook of the hamate, and therefore distal to the anatomical boundaries of Guyon’s canal. These findings were confirmed at the time of surgery when the injured segment of artery was excised. This included the branch to deep palmar arch. An end-to-end anastomosis using 8/0 nylon interrupted sutures was performed. The ulnar nerve and its branches were visualised clearly throughout the zone of injury, proximal and distal to it, and seen to be completely intact. Following surgery, clinical examination revealed partial resolution of all symptoms and initial clinical findings. Within a week there was further clinical and symptomatic improvement.
Figure 2.
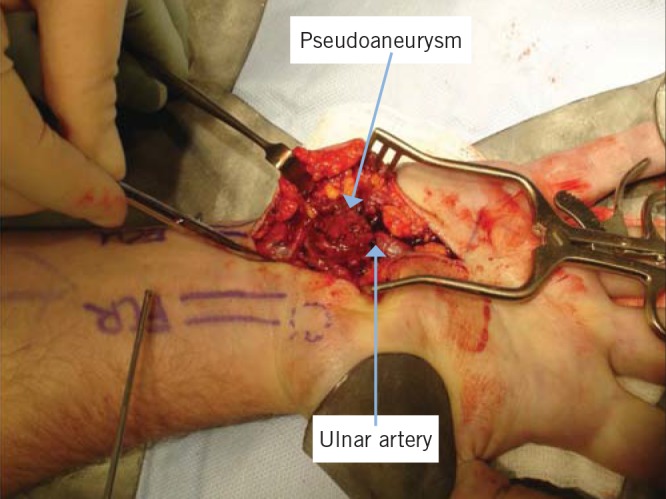
Pseudoaneurysm dissection and exposure
Discussion
Originally described in 1861 by Felix Guyon, 2 Guyon’s canal is a semirigid fibro-osseous tunnel through which the ulnar nerve, artery and, occasionally, communicating veins run. Traumatic aneurysms can be either true or false (pseudoaneurysm) depending on the extent of injury to the arterial wall. True aneurysms in the hand are most commonly caused by blunt trauma such as with those found in association with hypothenar hammer syndrome. Rare causes of true aneurysms of the hand include atherosclerosis, tumours, arteritis and osteogenesis imperfecta. 3 A false aneurysm is usually caused by penetrating injury of the arterial wall. This can be traumatic or iatrogenic (such as complication of arterial catheterisation), leading to the formation of an extra-arterial haematoma that becomes organised with a fibrous capsule.
Arterial aneurysms are less common in upper than in lower limbs. 4 Pseudoaneurysm as a cause of nerve palsy at any anatomical location is very unusual. A review of the literature revealed rare reports of upper limb pseudoaneurysms following penetrating trauma causing nerve palsies. 5,6 We were only able to find two reports, both from 1982, citing formation of a pseudoaneurysm in Guyon’s canal as a cause for ulnar nerve palsy causing sensory symptoms. 7,8 One case was from penetrating trauma and the other from blunt trauma. Following resection and end-to-end anastomosis, a pseudoaneurysm recurred in both of these cases.
In contrast to these, our patient’s pathology was just distal to Guyon’s canal. He presented with both sensory and motor symptoms. At follow-up there had been no recurrence of a pseudoaneurysm following resection and end-to-end anastomosis, suggesting this is a viable treatment option rather than just ligating the ulnar artery even in the presence of good radial arterial inflow. As with other neurological compression syndromes, prognosis depends on prompt treatment. 9
References
- 1.Hunt JR. Occupational neuritis of the deep palmar branch of the ulnar nerve. J Nerv Ment Dis 1908; 35: 673–689. [Google Scholar]
- 2.Guyon F. Note sur une disposition anatomique propre à la face antérieure de la région du poignet et non encore décrite. Bull Soc Anat Paris 1861; 6: 184–186. [Google Scholar]
- 3.Rothkopf DM, Bryan DJ, Cuadros CL, May JW. Surgical management of ulnar artery aneurysms. J Hand Surg Am 1990; 15: 891–897. [DOI] [PubMed] [Google Scholar]
- 4.Salari GR, Arend P, Ide Vet al Ulnar artery false aneurysm: temporary ultrasound-guided compression closure in an unusual case. Acta Chir Belg 1997; 97: 257–259. [PubMed] [Google Scholar]
- 5.Loréa P, Schuind F. False aneurysm appearing as delayed ulnar nerve palsy after ‘minor’ penetrating trauma in the forearm. J Trauma 2001; 51: 144–145. [DOI] [PubMed] [Google Scholar]
- 6.Milling MA, Kinmonth MH. False aneurysm of the ulnar artery. Hand 1977; 9: 57–59. [DOI] [PubMed] [Google Scholar]
- 7.Kalisman M, Laborde K, Wolff TW. Ulnar nerve compression secondary to ulnar artery false aneurysm at the Guyon’s canal. J Hand Surg Am 1982; 7: 137–139. [DOI] [PubMed] [Google Scholar]
- 8.Carlson CS, Clark GL. False aneurysm of ulnar artery in Guyon’s canal. J Hand Surg Am 1983; 8: 223–224. [DOI] [PubMed] [Google Scholar]
- 9.Rahimizadeh A. Unusual delayed radial nerve palsy caused by a traumatic aneurysm of a collateral radial artery: report of two cases. Neurosurgery 1992; 30: 628–630. [DOI] [PubMed] [Google Scholar]