

Abstract
Purpose
This study was conducted to evaluate prognostic factors and cancer-specific survival (CSS) in a cohort of 41 patients with urachal carcinoma by use of a Bayesian model-averaging approach.
Materials and Methods
Our cohort included 41 patients with urachal carcinoma who underwent extended partial cystectomy, total cystectomy, transurethral resection, chemotherapy, or radiotherapy at a single institute. All patients were classified by both the Sheldon and the Mayo staging systems according to histopathologic reports and preoperative radiologic findings. Kaplan-Meier survival curves and Cox proportional-hazards regression models were carried out to investigate prognostic factors, and a Bayesian model-averaging approach was performed to confirm the significance of each variable by using posterior probabilities.
Results
The mean age of the patients was 49.88±13.80 years and the male-to-female ratio was 24:17. The median follow-up was 5.42 years (interquartile range, 2.8-8.4 years). Five- and 10-year CSS rates were 55.9% and 43.4%, respectively. Lower Sheldon (p=0.004) and Mayo (p<0.001) stage, mucinous adenocarcinoma (p=0.005), and larger tumor size (p=0.023) were significant predictors of high survival probability on the basis of a log-rank test. By use of the Bayesian model-averaging approach, higher Mayo stage and larger tumor size were significant predictors of cancer-specific mortality in urachal carcinoma.
Conclusions
The Mayo staging system might be more effective than the Sheldon staging system. In addition, the multivariate analyses suggested that tumor size may be a prognostic factor for urachal carcinoma.
Keywords: Follow-up studies, Survival, Urachal cancer
INTRODUCTION
The urachus is a vestigial tubular structure that connects the urinary bladder to the allantois during early embryonic development [1]. Carcinomas of the urachus are believed to originate either from malignant transformation of columnar metaplasia from the lining of transitional epithelium or from enteric remnants during embryologic development [2]. The estimated annual incidence of urachal carcinoma is 0.01% of all cancers in adults; the overall incidence of the disease ranges from 0.55% to 1.20% of bladder tumors in Japan and from 0.07% to 0.70% of bladder tumors in Western countries [3]. Two systems have been proposed for staging urachal cancers. The first system was proposed by Sheldon et al. [4] in 1984. A more simplified system was recently proposed by the Mayo Clinic, although neither system has been validated [5]. However, the two staging systems have no criteria on tumor size in urachal cancer. Primary treatment of potentially localized disease includes wide local excision of the urachus, umbilicus, and surrounding soft tissue combined with partial or radical cystectomy and bilateral pelvic lymphadenectomy [6]. Debate exists regarding radical versus partial cystectomy [7]. The long-term prognosis of urachal cancer is poor because of its late presentation with local invasion and distant metastasis despite appropriate surgical treatment [8].
In our study, we reviewed all cases of urachal carcinomas that were diagnosed and treated at a single institute over the past 25 years. To date, there have been no randomized trials and fewer than 300 cases reported in the literature [9]. Moreover, there have not been any reports from a case series or a cohort study including more than 20 cases in a single-center series with long-term follow-up from Asia. Thus, we conducted this study to evaluate the prognostic factors of patients with urachal cancer by using a Bayesian model-averaging approach and to analyze prognosis by using data from the longest follow-up study and largest cohort of patients in Asia to date.
MATERIALS AND METHODS
1. Patient cohort
We reviewed the medical records of Severance Hospital from January 1988 to May 2012 and identified 41 patients who were newly diagnosed with urachal carcinoma. After Institutional Review Board approval, patient characteristics were obtained from medical records. In all patients, cystoscopy, abdominopelvic computed tomography, chest simple x-ray film, or bone scintigraphy were performed. In addition, histopathologic findings from transurethral resection specimens, partial cystectomy, or radical cystectomy and radiologic findings were examined to confirm urachal carcinoma.
2. Good clinical practice protocols
The study was performed in agreement with applicable laws and regulations, good clinical practices, and ethical principles as described in the Declaration of Helsinki. The Institutional Review Board of the Severance Hospital approved this study protocol (approval no. 4-2012-0897).
3. Outcome assessments of urachal cancer
All patients were classified by both the Sheldon staging system and the Mayo staging system according to histopathologic reports and preoperative radiologic findings. Tumor size was calculated on the basis of the maximal diameter in the pathologic reports. In patients without partial or radical cystectomy, tumor size was measured by using the long diameter on computed tomography. Patients who underwent adjuvant therapy were defined as those who received various regimens of chemotherapy, radiotherapy, or both. Histopathologic classifications were based on the pathological reports from our institute as follows: (1) mucinous adenocarcinoma, (2) nonmucinous adenocarcinoma, and (3) other pathologic findings originating from the urachus such as squamous cell carcinoma or signet ring cell carcinoma.
4. Statistical analyses
The end points of our study were 5- and 10-year cancer-specific survival (CSS) rates. Survival was defined as the time from diagnosis until death from urachal carcinoma. Patients alive at the final follow-up or who died of other causes were censored at that point. Associations between patient, tumor, and surgical variables were tested for their impact on survival by Pearson chi-square test. Kaplan-Meier survival curves were constructed and compared by using the log-rank test. The two above-mentioned staging systems, age, and tumor size were compared in terms of their ability to predict CSS by use of multivariate analysis with Kaplan-Meier survival curves and Cox proportional-hazards regression models with forward stepwise selection. Additionally, we used Bayesian model averaging to identify the best set of predictors for mortality across all feasible models on the basis of Bayesian probability theory. From these averaged estimates, the posterior probability that a coefficient was nonzero was calculated. The posterior probability, P(B≠0), is interpreted as the probability that a predictor has an effect. The interpretation of P(B≠0) has been categorized as follows: <50% is evidence against an effect; 50%-75% is weak evidence; 75%-95% is positive evidence; 95%-99% is strong evidence; and >99% is very strong evidence of an effect. Two-sided tests were performed and p-values <0.05 were considered statistically significant. Statistical analyses were performed with R statistics software (R ver. 3.0.3; R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org) by using BMA for a Bayesian model-averaging approach.
RESULTS
The general characteristics of the 41 patients who were diagnosed with urachal carcinoma at the Severance Hospital over the last 25 years are shown in Table 1. Five- and 10-year CSS rates were 55.9% and 43.4%, respectively (Fig. 1).
TABLE 1.
Characteristics of 41 patients with urachal carcinoma
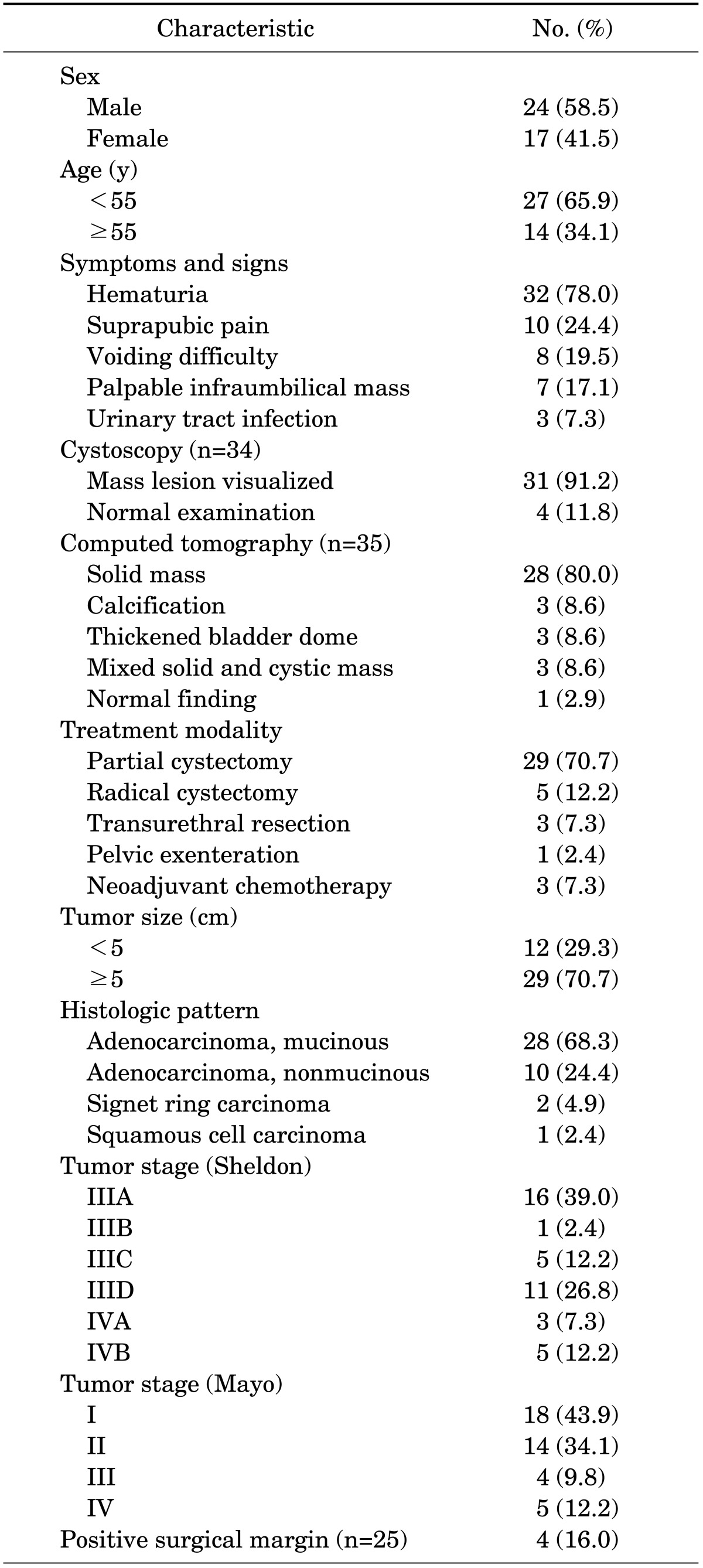
FIG. 1.
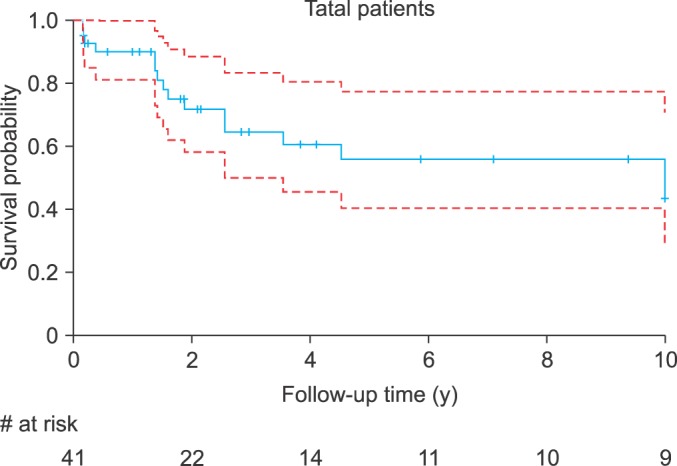
Cancer-specific survival (CSS) in 41 patients in the study cohort. Five- and 10-year CSS rates were 55.9% and 43.4%, respectively.
There was no statistical difference in CSS according to the patients' age, which was divided into two groups of <55 and ≥55 years (Fig. 2A). The patients were also divided into two subgroups according to the Sheldon staging system: IIIA, IIIB, and IIIC vs. IIID, IVA, and IVB. The subgroup with stage IIIA, IIIB, and IIIC showed significantly higher 10-year CSS in a log-rank test (p=0.004) (Fig. 2B). Ten-year CSS was also significantly different according to Mayo stage. Two subgroups including Mayo stages I and II vs. Mayo stages III and IV were created, and the group of Mayo stages I and II showed significantly higher 10-year CSS by use of the log-rank test (p<0.001) (Fig. 2C).
FIG. 2.

(A) <55 y vs. ≥55 y; (B) Sheldon stage IIIA, IIIB, and IIIC vs. Sheldon stage IIID, IVA, and IVB; (C) Mayo stages I and II vs. Mayo stages III and IV; (D) mucinous adenocarcinoma vs. others; and (E) <5 cm vs. ≥5 cm.
The histopathological results showed that there were 28 patients (68.3%) with mucinous adenocarcinoma, 11 (24.4%) with nonmucinous adenocarcinoma, 2 (4.9%) with signet ring cell carcinoma, and 1 (2.4%) with squamous cell carcinoma. The patients were then divided into two subgroups according to histopathological results: those with mucinous adenocarcinoma and those with other histopathologic findings. Ten-year CSS was significantly different between the two subgroups (p=0.005) (Fig. 2D). For our patient cohort, the mean tumor size was 6.31±2.84 cm. The patients were divided into two subgroups according to tumor size: <5 cm (n=12, 29.3%) vs. ≥5 cm (n=29, 70.7%). There were significant differences between the two subgroups according to a log-rank test (p=0.023) (Fig. 2E).
Adjuvant therapy was performed in 17 patients: 15 and 1 patients underwent chemotherapy and radiotherapy, respectively, and only 1 patient underwent both treatments. Subgroups were created according to whether patients did or did not undergo adjuvant therapy.
In univariate and multivariate Cox proportional-hazards regression models, we controlled for age, size, Sheldon staging system, Mayo staging system, histology, and adjuvant chemotherapy. In the univariate analysis, larger tumor size, higher Sheldon and Mayo stages, and nonmucinous adenocarcinoma were significant factors of poor prognosis for urachal carcinoma. In the multivariate Cox proportional-hazards regression analysis with Sheldon stage, there were no independent prognostic factors in three variables. However, in the multivariate analysis with Mayo stage, higher Mayo stage (hazard ratio [HR], 18.327; 95% confidence interval [CI], 3.986-84.270; p<0.001) and larger tumor size (HR, 6.617; 95% CI, 1.323-33.086; p=0.021) were independent factors for poor prognosis (Table 2).
TABLE 2.
Univariate and multivariate cox hazard proportional regression model for various factors
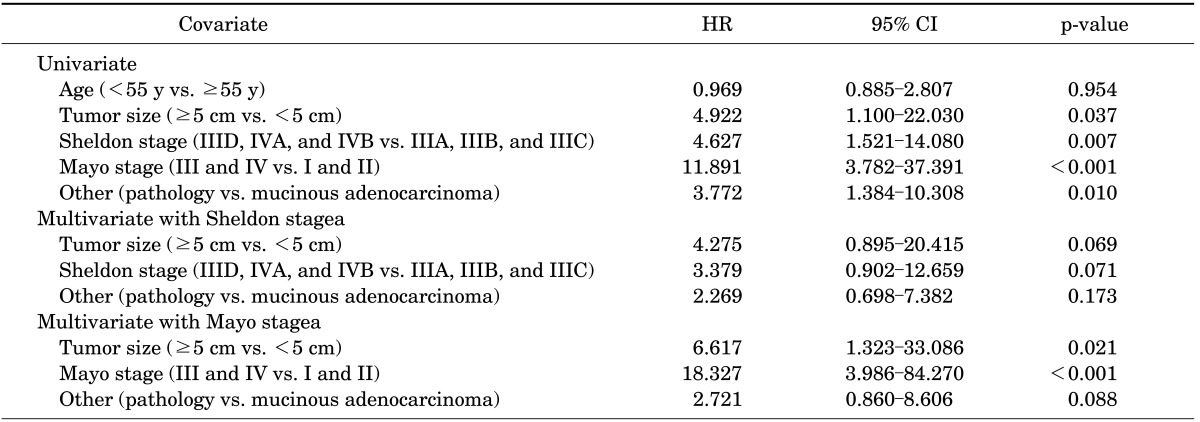
HR, hazard ratio; CI, confidence interval.
By use of the Bayesian model-averaging approach, higher Mayo stage was suggested as the most significant factor for mortality of urachal carcinoma (P(B≠0)=100%); the second was larger size of urachal cancer (P(B≠0)=95.8%) (Table 3).
TABLE 3.
Cox proportional hazard regression model coefficient estimates derived by using bayesian model averaging
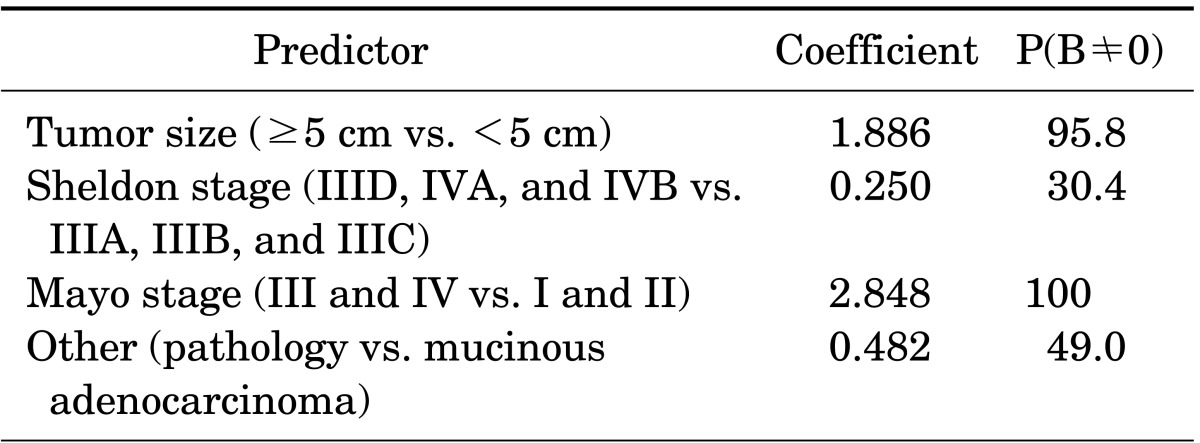
P(B≠0), the posterior probability that a coefficient is nonzero.
DISCUSSION
Urachal cancer was initially reported to have a 5-year survival rate of 6.5% to 15%, which represents a poor prognosis [10,11]. This poor prognosis is mainly attributable to the fact that the tumor occurs at the urachal remnant, which is located at the anterior portion of the bladder, thereby delaying symptom progression and making an early diagnosis difficult. In addition, the bladder wall is easily invaded owing to the absence of capsular formation in the bladder, and complete surgical resection is often unsuccessful because of inaccurate preoperative diagnosis [12]. Metastases initially are also seen primarily in the pelvic lymph nodes, locally in the space of Retzius, or at the apex of the bladder, and distant metastatic sites are noted in multiple organs, including liver, lung, bone, brain, and lymph nodes [5,13,14]. However, according to studies conducted since the 1980s, the 5-year survival rate has been reported to be up to 40% to 61% [15]. In the present study, the 5-year CSS and 10-year CSS were 53.0% and 45.5%, respectively.
Many studies with long-term follow-up of urachal cancer have recently been reported. Herr et al. [16] conducted a study on 50 patients who underwent extended partial cystectomy and reported that a survival rate of 70% was shown in a median 5-year follow-up, that pathological tumor stage and negative surgical margin were the most critical survival predictors, and that wide resection of the tumor and urachus was important. Pinthus et al. [17] conducted a 25-year follow-up study on the survival rate of 40 patients with urachal cancer and reported that the 5-year and 10-year overall survival rates were 61.3% and 49.2%, respectively, in a median 6-year follow-up, and that the survival rate was significantly higher in 32 patients who underwent a surgical treatment than in the remaining patients who did not undergo the surgical treatment. However, because surgical treatment was associated with a lower preoperative stage than neoadjuvant chemotherapy, it is inconclusive whether surgical treatment improves survival more than does nonsurgical treatment. In this study, the three patients who did not undergo surgical treatment had Mayo stages III (one patient) and IV (two patients) disease, which are higher stages than those of the other patients. Ashley et al. [5] reported that 5-year CSS was 49% in 66 patients with urachal cancer in a 54-year long-term follow-up. A multivariate analysis reported that grade and surgical margin were prognostic factors that are significantly associated with survival and that lymphadenectomy and adjuvant therapy had no survival benefit. That study concluded that no effective treatment was available for metastatic urachal cancer.
In the present study, survival was analyzed by dividing the patients into the adjuvant therapy group and the no adjuvant therapy group. As a result, the survival rate was significantly lower in the adjuvant therapy group than in the no adjuvant therapy group. This is likely attributed to the fact that the patients who underwent adjuvant therapy showed local recurrence (45.5%) or metastasis during the follow-up (27.3%) or had a high disease stage (Mayo stage III, one patient; Mayo stage IV, one patient) upon diagnosis. Siefker-Radtke [18] recently reported that the risk factors of urachal carcinoma associated with recurrence following surgery include (1) positive margin, (2) positive lymph node, (3) other metastasis, and (4) failure to resect the umbilicus en bloc with the urachal ligament and bladder. The aforementioned risk factors were significantly consistent with those shown in the results of this study.
In Asia, Ghazizadeh et al. [19] reported a secondary analysis that was conducted on 157 patients with urachal cancer collected from the Japanese literature in the past 49 years. They reported an incidence of 0.55% to 1.2%, higher than that of Western countries, and a 5-year survival rate of 6% in 66 patients. Because their study, however, was a secondary study via a literature review from 1932 to 1981, it seems unsuitable for the current diagnosis and treatment of urachal cancer. In China, Shou et al. [20] reported that 12 patients with cancer of urachal origin were observed out of 27 patients with bladder adenocarcinoma. In their study, the overall 5-year survival rate was 25.9% in the patients with urachal carcinoma. The low survival rate shown in this study is likely attributable to the fact that the study had a small sample size of 12 patients despite the long-term follow-up starting from 1970. In Japan, Asano et al. [21] reported that 9 of 15 urachal carcinoma patients (60%) survived after total cystectomy. Their study, however, did not report the survival rate and had no patient group for other treatment modalities. In Korea, Cho et al. [22] analyzed the oncologic outcomes of 31 patients (17 urachal and 14 nonurachal adenocarcinoma patients). They classified the patients into urachal and nonurachal groups according to Sheldon criteria, followed by analysis. No significant difference in CSS was found between the urachal and nonurachal groups for a mean follow-up period of 4.5 years, but the tumor size (≤4 cm) and histological type affected the survival rate in the case of mucinous adenocarcinoma. Their study had disadvantages in that it had a small size of 17 patients with cancer of urachal origin despite the long-term follow-up results, as shown in Shou et al. [20], and that it did not clearly present the median follow-up period and overall survival or CSS. A comparative analysis of previous studies is summarized in Table 4.
TABLE 4.
Previous studies on cancer-free survival for urachal carcinoma
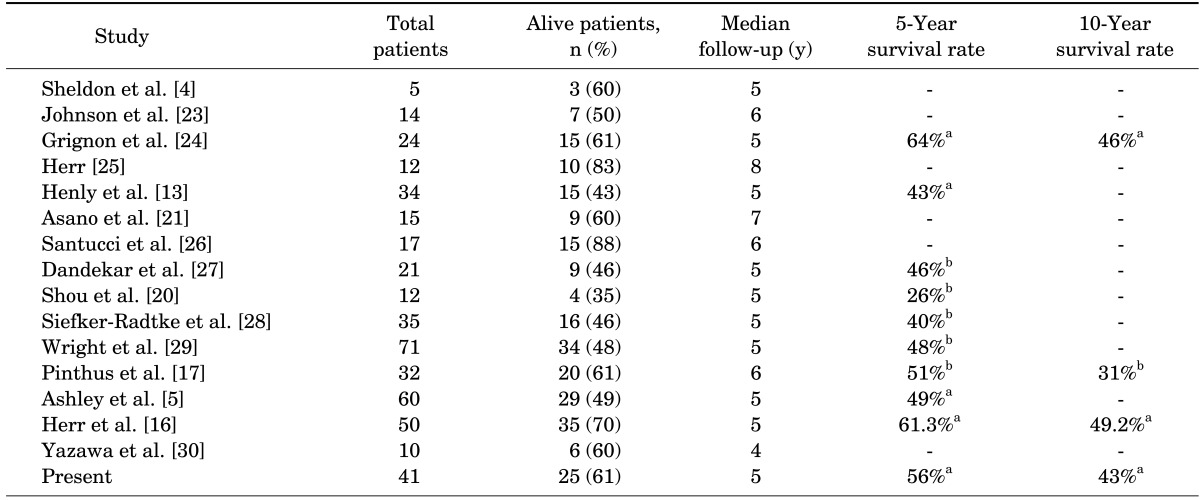
a:Cancer-specific survival. b:Overall survival.
The present study was conducted to investigate the survival of 41 patients with urachal cancer. It is the first study with long-term follow-up and a large sample size in Asia, and various risk factors were analyzed. Both the Sheldon staging system and the Mayo staging system showed a significant difference in the survival rate according to group. However, only the Mayo system showed a significant difference in both the multivariate analysis and the Bayesian model-averaging approach. This result is likely attributable to the fact that the Mayo system proposed by Ashley et al. [5] in 2006 is simpler and has four stages that are easier to apply in clinical practice than is the Sheldon system. The clinical significance of tumor size is still controversial. Cho et al. [22] reported that the size significantly affected CSS. In most studies, however, tumor size was not included in the staging system, which means that it might not affect the survival rate. In a Bayesian model-averaging approach, higher tumor size was the second higher posterior probability rank. In the future, a new staging system should consider larger tumor size as a prognostic factor following systematic review and meta-analysis for CSS of urachal cancer.
CONCLUSIONS
We have reported 41 cases of urachal carcinoma seen at a single institute over a recent 25-year period. The patient 5- and 10-year CSS rates were 55.9% and 43.4%, respectively. According to the survival rate in our study, the Mayo staging system might be more effective than the Sheldon staging system. In addition, higher Mayo stage and larger tumor size may be risk factors that can be used to predict CSS of urachal carcinoma.
Footnotes
The authors have nothing to disclose.
References
- 1.Paner GP, Barkan GA, Mehta V, Sirintrapun SJ, Tsuzuki T, Sebo TJ, et al. Urachal carcinomas of the nonglandular type: salient features and considerations in pathologic diagnosis. Am J Surg Pathol. 2012;36:432–442. doi: 10.1097/PAS.0b013e31823fe49c. [DOI] [PubMed] [Google Scholar]
- 2.Van Calsteren K, Van Mensel K, Joniau S, Oyen R, Hanssens M, Amant F, et al. Urachal carcinoma during pregnancy. Urology. 2006;67:1290.e19–1290.e21. doi: 10.1016/j.urology.2005.12.041. [DOI] [PubMed] [Google Scholar]
- 3.Scabini S, Rimini E, Romairone E, Scordamaglia R, Vallarino L, Giasotto V, et al. Urachal tumour: case report of a poorly understood carcinoma. World J Surg Oncol. 2009;7:82. doi: 10.1186/1477-7819-7-82. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 4.Sheldon CA, Clayman RV, Gonzalez R, Williams RD, Fraley EE. Malignant urachal lesions. J Urol. 1984;131:1–8. doi: 10.1016/s0022-5347(17)50167-6. [DOI] [PubMed] [Google Scholar]
- 5.Ashley RA, Inman BA, Sebo TJ, Leibovich BC, Blute ML, Kwon ED, et al. Urachal carcinoma: clinicopathologic features and long-term outcomes of an aggressive malignancy. Cancer. 2006;107:712–720. doi: 10.1002/cncr.22060. [DOI] [PubMed] [Google Scholar]
- 6.Mohile SG, Schleicher L, Petrylak DP. Treatment of metastatic urachal carcinoma in an elderly woman. Nat Clin Pract Oncol. 2008;5:55–58. doi: 10.1038/ncponc1009. [DOI] [PubMed] [Google Scholar]
- 7.Cothren C, Ferucci P, Harken AH, Veve R, Finlayson CA, Johnson JL. Urachal carcinoma: key points for the general surgeon. Am Surg. 2002;68:201–203. [PubMed] [Google Scholar]
- 8.Chan ES, Ng CF, Chui KL, Lo KL, Hou SM, Yip SK. Novel approach of laparoscopic transperitoneal en bloc resection of urachal tumor and umbilectomy with a comparison of various techniques. J Laparoendosc Adv Surg Tech A. 2009;19:423–426. doi: 10.1089/lap.2008.0266. [DOI] [PubMed] [Google Scholar]
- 9.Elser C, Sweet J, Cheran SK, Haider MA, Jewett M, Sridhar SS. A case of metastatic urachal adenocarcinoma treated with several different chemotherapeutic regimens. Can Urol Assoc J. 2012;6:E27–E31. doi: 10.5489/cuaj.11109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mostofi FK, Thomson RV, Dean AL., Jr Mucous adenocarcinoma of the urinary bladder. Cancer. 1955;8:741–758. doi: 10.1002/1097-0142(1955)8:4<741::aid-cncr2820080417>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 11.Nadjmi B, Whitehead ED, Mckiel CF, Jr, Graf EC, Callahan DH. Carcinoma of the urachus: report of two cases and review of the literature. J Urol. 1968;100:738–743. doi: 10.1016/s0022-5347(17)62614-4. [DOI] [PubMed] [Google Scholar]
- 12.Cho KS, Yang WJ, Cho NH, Yang SC, Hong SJ, Choi YD. The clinical characteristics and prognosis of urachal cancer. Korean J Urol. 2004;45:1229–1234. [Google Scholar]
- 13.Henly DR, Farrow GM, Zincke H. Urachal cancer: role of conservative surgery. Urology. 1993;42:635–639. doi: 10.1016/0090-4295(93)90526-g. [DOI] [PubMed] [Google Scholar]
- 14.Hong SH, Kim JC, Hwang TK. Laparoscopic partial cystectomy with en bloc resection of the urachus for urachal adenocarcinoma. Int J Urol. 2007;14:963–965. doi: 10.1111/j.1442-2042.2007.01855.x. [DOI] [PubMed] [Google Scholar]
- 15.Kakizoe T, Matsumoto K, Andoh M, Nishio Y, Kishi K. Adenocarcinoma of urachus. Report of 7 cases and review of literature. Urology. 1983;21:360–366. doi: 10.1016/0090-4295(83)90152-8. [DOI] [PubMed] [Google Scholar]
- 16.Herr HW, Bochner BH, Sharp D, Dalbagni G, Reuter VE. Urachal carcinoma: contemporary surgical outcomes. J Urol. 2007;178:74–78. doi: 10.1016/j.juro.2007.03.022. [DOI] [PubMed] [Google Scholar]
- 17.Pinthus JH, Haddad R, Trachtenberg J, Holowaty E, Bowler J, Herzenberg AM, et al. Population based survival data on urachal tumors. J Urol. 2006;175:2042–2047. doi: 10.1016/S0022-5347(06)00263-1. [DOI] [PubMed] [Google Scholar]
- 18.Siefker-Radtke A. Urachal carcinoma: surgical and chemotherapeutic options. Expert Rev Anticancer Ther. 2006;6:1715–1721. doi: 10.1586/14737140.6.12.1715. [DOI] [PubMed] [Google Scholar]
- 19.Ghazizadeh M, Yamamoto S, Kurokawa K. Clinical features of urachal carcinoma in Japan: review of 157 patients. Urol Res. 1983;11:235–238. doi: 10.1007/BF00272286. [DOI] [PubMed] [Google Scholar]
- 20.Shou J, Ma J, Xu B. Adenocarcinoma of the urinary bladder: a report of 27 cases. Zhonghua Zhong Liu Za Zhi. 1999;21:461–463. [PubMed] [Google Scholar]
- 21.Asano K, Miki J, Yamada H, Maeda S, Abe K, Furuta A, et al. Carcinoma of urachus: report of 15 cases and review of literature: is total cystectomy the treatment of choice for urachal carcinoma? Nihon Hinyokika Gakkai Zasshi. 2003;94:487–494. doi: 10.5980/jpnjurol1989.94.487. [DOI] [PubMed] [Google Scholar]
- 22.Cho SY, Moon KC, Park JH, Kwak C, Kim HH, Ku JH. Outcomes of Korean patients with clinically localized urachal or non-urachal adenocarcinoma of the bladder. Urol Oncol. 2013;31:24–31. doi: 10.1016/j.urolonc.2010.10.002. [DOI] [PubMed] [Google Scholar]
- 23.Johnson DE, Hodge GB, Abdul-Karim FW, Ayala AG. Urachal carcinoma. Urology. 1985;26:218–221. doi: 10.1016/0090-4295(85)90112-8. [DOI] [PubMed] [Google Scholar]
- 24.Grignon DJ, Ro JY, Ayala AG, Johnson DE, Ordonez NG. Primary adenocarcinoma of the urinary bladder. A clinicopathologic analysis of 72 cases. Cancer. 1991;67:2165–2172. doi: 10.1002/1097-0142(19910415)67:8<2165::aid-cncr2820670827>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- 25.Herr HW. Urachal carcinoma: the case for extended partial cystectomy. J Urol. 1994;151:365–366. doi: 10.1016/s0022-5347(17)34950-9. [DOI] [PubMed] [Google Scholar]
- 26.Santucci RA, True LD, Lange PH. Is partial cystectomy the treatment of choice for mucinous adenocarcinoma of the urachus? Urology. 1997;49:536–540. doi: 10.1016/s0090-4295(96)00574-2. [DOI] [PubMed] [Google Scholar]
- 27.Dandekar NP, Dalal AV, Tongaonkar HB, Kamat MR. Adenocarcinoma of bladder. Eur J Surg Oncol. 1997;23:157–160. doi: 10.1016/s0748-7983(97)80012-1. [DOI] [PubMed] [Google Scholar]
- 28.Siefker-Radtke AO, Gee J, Shen Y, Wen S, Daliani D, Millikan RE, et al. Multimodality management of urachal carcinoma: the M. D. Anderson Cancer Center experience. J Urol. 2003;169:1295–1298. doi: 10.1097/01.ju.0000054646.49381.01. [DOI] [PubMed] [Google Scholar]
- 29.Wright JL, Porter MP, Li CI, Lange PH, Lin DW. Differences in survival among patients with urachal and nonurachal adenocarcinomas of the bladder. Cancer. 2006;107:721–728. doi: 10.1002/cncr.22059. [DOI] [PubMed] [Google Scholar]
- 30.Yazawa S, Kikuchi E, Takeda T, Matsumoto K, Miyajima A, Nakagawa K, et al. Surgical and chemotherapeutic options for urachal carcinoma: report of ten cases and literature review. Urol Int. 2012;88:209–214. doi: 10.1159/000334414. [DOI] [PubMed] [Google Scholar]