

Abstract
Purpose
To evaluate how much the improvement of lower urinary tract symptoms (LUTS) affects sexual function and which storage symptoms or voiding symptoms have the greatest effect on sexual function.
Materials and Methods
A total of 187 patients were enrolled in this study. Patients were randomly assigned to receive either tamsulosin 0.2 mg (group A) or tamsulosin 0.2 mg and solifenacin 5 mg (group B). At 4 weeks and 12 weeks, the LUTS and sexual function of the patients were evaluated by use of the International Index of Erectile Function-5 (IIEF5), International Prostate Symptom Score (IPSS), Overactive Bladder Symptom Score (OABSS) questionnaire, uroflowmetry, and bladder scan.
Results
Both groups A and B showed statistically significant improvements in IPSS, OABSS, and quality of life (QoL). Group A showed improved maximum flow rate, mean flow rate, and residual urine volume by time. Group B did not show an improvement in flow rate or residual urine volume but total voiding volume increased with time. The IIEF5 score was not improved in either group. In group A, the IIEF5 score dropped from 13.66±4.97 to 11.93±6.14 after 12 weeks (p=0.072). Group B showed a decline in the IIEF5 score from 13.19±5.91 to 12.45±6.38 (p=0.299). Although group B showed a relatively smaller decrease in the IIEF5 score, the difference between the two groups was not significant (p=0.696).
Conclusions
Tamsulosin monotherapy and combination therapy with solifenacin did not improve erectile function despite improvements in voiding symptoms and QoL. The improvement in storage symptoms did not affect erectile function.
Keywords: Erectile dysfunction, Lower urinary tract symptoms, Overactive urinary bladder
INTRODUCTION
Lower urinary tract symptoms (LUTS) and sexual dysfunction are frequently observed in aged men. Large-scale epidemiologic studies have reported that LUTS are closely and independently associated with sexual dysfunction [1]. Through the relieving of LUTS, α-blockers result in improvement of sexual dysfunction [2,3]. Theoretically, modulation of α-adrenergic activity, which decreases smooth muscle tone in the bladder neck, prostate capsule, and corpus cavernosum, may improve LUTS and sexual dysfunction at the same time. By contrast, as the result of a blood pressure lowering effect or another uncertain mechanism, α-blockers may have an adverse effect on erectile function [4]. The results of our recent study suggested that tamsulosin 0.2 mg did not exhibit any significant effect on sexual function [5].
Storage symptoms such as urgency, urge incontinence, and nocturia are more bothersome than voiding symptoms [6]. Anticholinergics are an effective medication for overactive bladder (OAB) with urgency and with or without urge incontinence. A recent study reported that anticholinergics and α-blocker combination therapy was effective for patients with benign prostatic hyperplasia and OAB [7,8]. However, the relationship between storage symptoms and sexual dysfunction is not well known. Knowing the effect of storage symptoms on sexual dysfunction would allow for more valuable management of sexual dysfunction.
In this study, we evaluated how much the improvement of LUTS affects sexual function and which storage symptoms or voiding symptoms have the greatest effect on sexual function as assessed by the International Prostate Symptom Score (IPSS), overactive bladder symptoms score (OABSS), and International Index of Erectile Function (IIEF) questionnaires.
MATERIALS AND METHODS
A total of 187 patients were enrolled in this multicenter, prospective, randomized, comparative, open-label study from July 2011 to June 2012. The primary purpose of this study was to evaluate the effect of treatment of LUTS on patients with sexual dysfunction. The second purpose was to assess which voiding symptoms or storage symptoms most affected sexual dysfunction. The Ethic Committee of each participatory institution approved this clinical study, and written consent was provided by all subjects prior to participation (11-008).
Men 40 years of age or older who had LUTS as indicated by an IPSS>12, urinary frequency (≥8/d), urgency (≥1/d), and symptoms on a 3-day voiding diary were invited to participate. All patients were sexually active more than once per month regardless of IIEF score. Patients with urologic malignancy, urinary tract infection, medical renal disease, medical liver disease, or clinically significant bladder outlet obstruction (residual urine>100 mL) were excluded from study. Patients who took medications such as androgens, antiandrogens, and phosphodiesterase type 5 inhibitors were also excluded. All patients provided informed consent.
Initially, patients were evaluated by history taking, physical examination, urine analysis with microscopic assay, uroflowmetry (UFM), bladder scan, voiding diary, IIEF, IPSS, and OABSS questionnaires. Patients were randomly assigned to receive either tamsulosin 0.2 mg only (group A) or tamsulosin 0.2 mg and solifenacin 5 mg combination (group B) by block randomization. At 4 weeks and 12 weeks, the LUTS and sexual function of the patients were evaluated by the IIEF, IPSS, and OABSS questionnaire. UFM and bladder scan were performed for functional study (Fig. 1).
FIG. 1.

Flow of the study.
Clinicopathologic variables between the two groups were statistically analyzed by use of two-sample t-tests. Mixed model analysis was performed to compare the outcomes of each group. SAS 9.1.3 (SAS Institute Inc., Cary, NC, USA) was used for statistical analysis. In all tests, p-values of 0.05 were considered statistically significant.
RESULTS
A total of 187 patients were registered for this study. Group A consisted of 93 patients and group B consisted of 94. Twenty-two patients dropped out at the 4-week follow-up (group A, 13 patients; group B, 9 patients), and 28 patients dropped out at the 12-week follow-up (group A, 16 patients; group B, 12 patients). Overall, 64 patients (68.8%) in group A and 73 patients (77.7%) in group B completed this study. The baseline clinicopathologic data are shown in Table 1.
TABLE 1.
All clinicopathogic factors were not different between two groups except OABSS
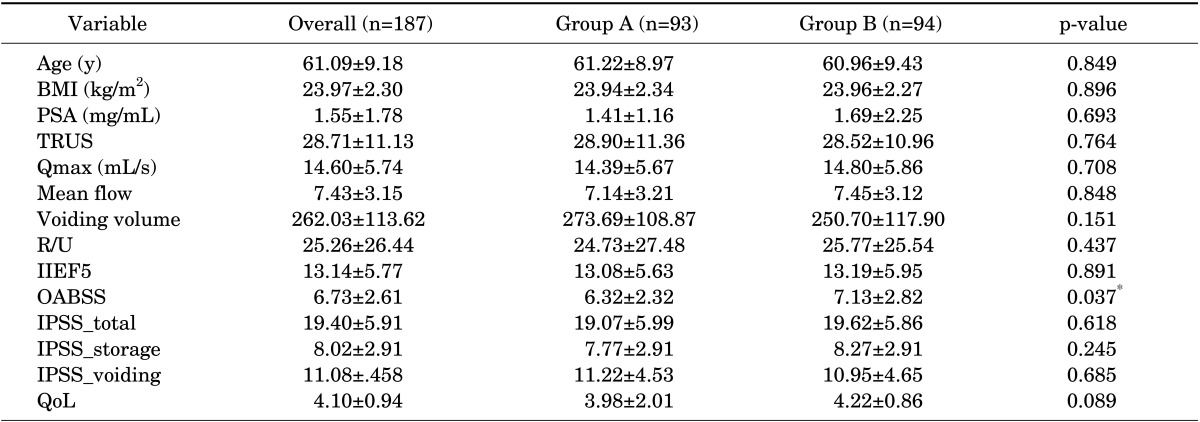
Values are presented as mean±standard deviation.
OABSS, overactive bladder symptom score; BMI, body mass index; PSA, prostate-specific antigen; TRUS, transrectal ultrasound; Qmax, maximum flow rate; R/U, residual urine; IIEF5, International Index of Erectile Function-5; IPSS, International Prostate Symptom Score; QoL, quality of life.
Group A: tamsulosin 0.2 mg only. Group B: tamsulosin 0.2 mg+solifenacin 5 mg.
The mean age of the enrolled patients (n=187) was 61.09±9.18 years. Mean prostate volume and PSA were 28.71±11.13 mL and 1.55±1.78 ng/dL, respectively. UFM study showed a total voiding volume of 262.02 mL, mean flow rate of 7.43 mL/s, and maximum flow rate (Qmax) of 14.6 mL/s. Residual urine checked by bladder scan was 25.26 mL. Mean IPSS was 19.40±5.91 (voiding symptoms, 11.08±4.58; storage symptoms, 8.02±2.91). Mean OABSS, quality of life (QoL), and IIEF scores were 6.73±2.61, 4.10±0.95, and 13.14±5.77, respectively. No clinicopathologic factors were significantly different between the two groups except the OABSS, which was higher in group B than in group A (6.32 vs. 7.13, p=0.037) (Table 1).
UFM study showed the Qmax, mean flow rate, and residual urine volume improved with time in group A. Group B did not show an improvement in flow rate or residual urine volume with time, whereas total voiding volume did increase. Overall, groups A and B did not differ significantly in UFM scale (Qmax, p=0.404; mean flow rate, p=0.179; voiding volume, p=0.677) (Fig. 2). Because residual urine volume did not decrease, group B showed a greater residual urine volume than that in group A (p=0.013).
FIG. 2.

(A-C) The groups did not differ significantly on variables of the uroflowmetry scale except for residual urine volume. (D) Because residual urine volume did not decrease, group B showed a much greater residual urine volume than that in group A (p=0.013). Group A: tamsulosin 0.2 mg only. Group B: tamsulosin 0.2 mg+solifenacin 5 mg. *Statistically significant by time (p<0.05).
In the questionnaire analysis of LUTS, both groups showed statistically significant improvement in the IPSS, OABSS, and QoL. When the IPSS was divided into storage and voiding symptoms, both groups showed significant improvement in both categories of symptoms. However, the difference between the two groups was not significant (p=0.083 and p=0.358) (Fig. 3). The OABSS was higher in group B than in group A at baseline (p=0.037). However, after treatment for 12 weeks, there was no significant difference in the OABSS in either group (p=0.905, data not shown).
FIG. 3.

Both groups showed a statistically significant improvement in the International Prostate Symptom Score (IPSS), overactive bladder symptom score (OABSS), and quality of life (QoL) score. However, a statistically significant difference was not observed between the two groups. Group A: tamsulosin 0.2 mg only. Group B: tamsulosin 0.2 mg+solifenacin 5 mg. *Statistically significant by time (p<0.05).
The IIEF5 score was not improved in either group (Fig. 4). In group A, the IIEF5 score dropped from 13.66±4.97 to 11.93±6.14 after 12 weeks of medication (p=0.072). Group B also showed a decline in the IIEF5 score (from 13.19±5.91 to 12.45±6.38, p=0.299). Although group B showed a relatively smaller decrease in the IIEF5 score compared with group A, the difference between the two groups was not statistically significant (p=0.696).
FIG. 4.
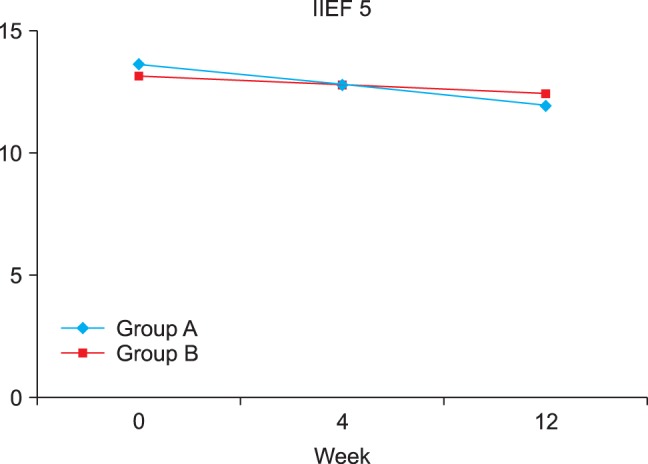
Neither group of patients with lower urinary tract symptoms showed an improvement in sexual dysfunction. Although the International Index of Erectile Function-5 (IIEF5) score decreased relatively less in group B compared with group A, the difference between the two groups was not statistically significant (p=0.696). Group A: tamsulosin 0.2 mg only. Group B: tamsulosin 0.2 mg+solifenacin 5 mg.
Adverse effects were reported for 15 patients. In group A, six patients complained of mild adverse effects (gastric discomfort in 5, dry mouth in 1). These mild adverse effects resolved in all patients without any management. Nine patients in groups B had a mild adverse effect (gastric discomfort in 3, itching in 1, dry mouth in 2, general weakness in 1, constipation in 1, and urticaria in 1). Patients with urticaria took a dermatologic medicine. The combination group showed more adverse effects, but urinary retention was not reported in the study period.
DISCUSSION
The Multinational Survey of the Aging Male suggested that LUTS were an independent prognostic factor for sexual dysfunction [9]. LUTS medication improves the sexual dysfunction of LUTS patients [2,3]. However, LUTS are divided into voiding symptoms and storage symptoms. α-Blockers and 5-androgen receptor inhibitors are an effective medication for men with LUTS [10,11]. However, these medications are not sufficient for managing all patients with LUTS, because LUTS originate not only from pathologic benign prostatic hyperplasia also as a result of a detrusor muscle condition [12]. Several studies have reported that OAB is highly associated with male sexual dysfunction [13,14,15].
Storage symptoms such as frequency, nocturia, urgency, and urge incontinence are more common and bothersome than voiding symptoms such as weak stream, intermittency, hesitancy, strain, and postvoid dribbling [6]. A previous study reported that 51% of LUTS patients have storage symptoms and 26% have voiding symptoms at age ≥18 years, and 74% of patients have storage symptoms and 37% have voiding symptoms at age ≥60 years [16]. Other studies showed that 28% of men aged ≥40 years had LUTS. Storage symptoms only (13%) was more frequent than voiding symptoms only (6%). Mixed symptoms (9%) were more frequent than voiding symptoms, too [17]. Thus, α-blocker monotherapy may not be the appropriate treatment in patients with LUTS including OAB because of failure to relieve the storage symptoms. In a previous study, the combination treatment of α-blocker and anticholinergic was a safe and effective modality in LUTS patients with OAB [8]. However, it has not been sufficiently evaluated whether anticholinergic monotherapy or combination therapy with an α-blocker and an anticholinergic improves sexual function in LUTS patients with OAB. In this study, although not statistically significant, the IIEF score of the combination therapy group decreased relatively less than in the monotherapy group.
In a recent previous study of initial combination treatment with tamsulosin 0.2 mg and solifenacin 5 mg, the authors reported that earlier combination treatment improves storage symptoms and QoL [7]. Their clinicopathologic data and results were very similar to ours. Their data showed that the combination group had an improved IPSS storage score, QoL, and OABSS at 4 weeks, but that there was no significant difference in any of the questionnaire scores between the two groups in 12 weeks. Additionally, they reported that the measured UFM values did not differ statistically between the two groups. We checked UFM variables and bladder scans in this study, also. In contrast with the questionnaire, the values measured by UFM gave us some important information. The combination group showed increased voiding volume with time (250.7 mL at baseline, 265.5 mL at 4 weeks, 279.6 mL at 12 weeks, p=0.019), whereas flow rate and residual urine volume did not change. In another study also, the combination of tamsulosin 0.4 mg and solifenacin 6 mg/9 mg did not affect the uroflow rate or residual urine [18]. The lack of change in residual urine volume in group B directly affected the lack of occurrence of urinary retention in this study.
The subscale numbers 1, 3, 5, and 6 of the IPSS imply voiding symptoms and the numbers 2, 4, and 7 imply storage symptoms. The storage subscale of IPSS included urgency but not urge incontinence. Thus, we also used the OABSS. At baseline, although the storage symptom score was not significantly different, group B had a higher OABSS than group A. This difference may be because of reference to different symptom durations on the questionnaires. The IPSS asks about voiding symptoms during the last month in contrast with the last week on the OABSS. Second, the question about frequency is quite different: "How often have you had to urinate less than every two hours?" on the IPSS vs. "How many times do you typically urinate from waking in the morning until sleeping at night?" on the OABSS [19,20]. Frequency (question 1) and nocturnal frequency (question 2) on the OABSS were statistically higher in group B (p=0.059, p=0.008, Mann-Whitney test, data not shown). Urgency (question 3) was not significantly different (p=0.533). The mean number of instances of urge incontinence (question 4) was 0.91 in group A and 1.11 in group B. This difference was also not statistically significant (p=0.568).
It is well known that OAB has a greater negative impact on everyday life and a detrimental effect on sexual life in women [21]. Anticholinergics improve sexual function in female patients with OAB [22,23]. The mechanism by which anticholinergics affect sexual function differs substantially between men and women. Investigators have suggested that the occurrence of urinary leakage during intercourse may be stressful in women, and anticholinergics may improve sexual function by aborting urinary leakage [22]. However, the detrusor muscle and sexual function are regulated by a shared neurologic nerve pathway and neurotransmitters [23]. Thus, anticholinergics including solifenacin may indirectly affect the sexual function of both men and women. In our study, a direct comparison between anticholinergics and an α-blocker or placebo was lacking because there was no solifenacin only treatment group. This study showed that sexual function improved regardless of solifenacin. To understand the effect of anticholinergics on sexual function in men, additional study including a solifenacin only treatment group will be necessary.
This study had several limitations. First, a difference in follow-up loss was present among the centers, and group B showed a higher OABSS at baseline. This may indicate a selection bias even though this was a prospective study. However, the clinicopathologic data in this study were similar to previous studies, and other data were well distributed between the two groups. Data were collected from patients who completed the study. Second, tamsulosin is reported to result in de novo ejaculatory discomfort in about 10% of patients [5]. Ejaculatory discomfort is an important sexual problem. However, this topic was not addressed in the present study. Third, this study did not include a placebo group or solifenacin monotherapy group. If male OAB patients without bladder outlet obstruction are treated by anticholinergics, improved sexual function may be observed as in female patients with OAB. Last, due to the relatively short follow-up duration and small patient number, the results of this study should be interpreted cautiously.
CONCLUSIONS
Tamsulosin monotherapy and combination therapy with tamsulosin and solifenacin did not improve erectile function in LUTS patients. The improvement of storage symptoms was not significantly associated with sexual function.
Footnotes
I (Kwangsung Park, corresponding author including other authors) got grants from Astellas Pharma Korea, Inc. However, Astellas Pharma Korea, Inc only had a financial role for this research.
References
- 1.Rosen RC, Wei JT, Althof SE, Seftel AD, Miner M, Perelman MA, et al. Association of sexual dysfunction with lower urinary tract symptoms of BPH and BPH medical therapies: results from the BPH Registry. Urology. 2009;73:562–566. doi: 10.1016/j.urology.2008.05.034. [DOI] [PubMed] [Google Scholar]
- 2.Jeh SU, Chung KH, Jung JH, Hyun JS. Improvement of lower urinary tract symptoms and sexual function after treatment with alpha-blocker. Korean J Urol. 2009;50:369–374. [Google Scholar]
- 3.Kumar R, Nehra A, Jacobson DJ, McGree ME, Gades NM, Lieber MM, et al. Alpha-blocker use is associated with decreased risk of sexual dysfunction. Urology. 2009;74:82–87. doi: 10.1016/j.urology.2008.12.080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nordling J. Efficacy and safety of two doses (10 and 15 mg) of alfuzosin or tamsulosin (0.4 mg) once daily for treating symptomatic benign prostatic hyperplasia. BJU Int. 2005;95:1006–1012. doi: 10.1111/j.1464-410X.2005.05456.x. [DOI] [PubMed] [Google Scholar]
- 5.Kim SW, Lee WC, Kim MT, Ko K, Lee WK, Lee CH, et al. Effects of low-dose tamsulosin on sexual function in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Korean J Urol. 2013;54:697–702. doi: 10.4111/kju.2013.54.10.697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Roehrborn CG, Kaplan SA, Kraus SR, Wang JT, Bavendam T, Guan Z. Effects of serum PSA on efficacy of tolterodine extended release with or without tamsulosin in men with LUTS, including OAB. Urology. 2008;72:1061–1067. doi: 10.1016/j.urology.2008.06.067. [DOI] [PubMed] [Google Scholar]
- 7.Lee SH, Byun SS, Lee SJ, Kim KH, Lee JY. Effects of initial combined tamsulosin and solifenacin therapy for overactive bladder and bladder outlet obstruction secondary to benign prostatic hyperplasia: a prospective, randomized, multicenter study. Int Urol Nephrol. 2014;46:523–529. doi: 10.1007/s11255-013-0551-7. [DOI] [PubMed] [Google Scholar]
- 8.Kaplan SA, Roehrborn CG, Chancellor M, Carlsson M, Bavendam T, Guan Z. Extended-release tolterodine with or without tamsulosin in men with lower urinary tract symptoms and overactive bladder: effects on urinary symptoms assessed by the International Prostate Symptom Score. BJU Int. 2008;102:1133–1139. doi: 10.1111/j.1464-410X.2008.07761.x. [DOI] [PubMed] [Google Scholar]
- 9.Rosen R, Altwein J, Boyle P, Kirby RS, Lukacs B, Meuleman E, et al. Lower urinary tract symptoms and male sexual dysfunction: the multinational survey of the aging male (MSAM-7) Eur Urol. 2003;44:637–649. doi: 10.1016/j.eururo.2003.08.015. [DOI] [PubMed] [Google Scholar]
- 10.Haillot O, Fraga A, Maciukiewicz P, Pushkar D, Tammela T, Hofner K, et al. The effects of combination therapy with dutasteride plus tamsulosin on clinical outcomes in men with symptomatic BPH: 4-year post hoc analysis of European men in the CombAT study. Prostate Cancer Prostatic Dis. 2011;14:302–306. doi: 10.1038/pcan.2011.13. [DOI] [PubMed] [Google Scholar]
- 11.McConnell JD, Roehrborn CG, Bautista OM, Andriole GL, Jr, Dixon CM, Kusek JW, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349:2387–2398. doi: 10.1056/NEJMoa030656. [DOI] [PubMed] [Google Scholar]
- 12.Lemack GE. Defining the role of overactive bladder treatments in men with lower urinary tract symptoms. Nat Clin Pract Urol. 2007;4:174–175. doi: 10.1038/ncpuro0754. [DOI] [PubMed] [Google Scholar]
- 13.Leliefeld HH, Stoevelaar HJ, McDonnell J. Sexual function before and after various treatments for symptomatic benign prostatic hyperplasia. BJU Int. 2002;89:208–213. doi: 10.1046/j.1464-4096.2001.01817.x. [DOI] [PubMed] [Google Scholar]
- 14.Aslan G, Cavus E, Karas H, Oner O, Duran F, Esen A. Association between lower urinary tract symptoms and erectile dysfunction. Arch Androl. 2006;52:155–162. doi: 10.1080/01485010500379871. [DOI] [PubMed] [Google Scholar]
- 15.Irwin DE, Milsom I, Reilly K, Hunskaar S, Kopp Z, Herschorn S, et al. Overactive bladder is associated with erectile dysfunction and reduced sexual quality of life in men. J Sex Med. 2008;5:2904–2910. doi: 10.1111/j.1743-6109.2008.01000.x. [DOI] [PubMed] [Google Scholar]
- 16.Irwin DE, Milsom I, Hunskaar S, Reilly K, Kopp Z, Herschorn S, et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50:1306–1314. doi: 10.1016/j.eururo.2006.09.019. [DOI] [PubMed] [Google Scholar]
- 17.Glasser DB, Carson C, 3rd, Kang JH, Laumann EO. Prevalence of storage and voiding symptoms among men aged 40 years and older in a US population-based study: results from the Male Attitudes Regarding Sexual Health study. Int J Clin Pract. 2007;61:1294–1300. doi: 10.1111/j.1742-1241.2007.01454.x. [DOI] [PubMed] [Google Scholar]
- 18.Kaplan SA, He W, Koltun WD, Cummings J, Schneider T, Fakhoury A. Solifenacin plus tamsulosin combination treatment in men with lower urinary tract symptoms and bladder outlet obstruction: a randomized controlled trial. Eur Urol. 2013;63:158–165. doi: 10.1016/j.eururo.2012.07.003. [DOI] [PubMed] [Google Scholar]
- 19.Homma Y, Yoshida M, Seki N, Yokoyama O, Kakizaki H, Gotoh M, et al. Symptom assessment tool for overactive bladder syndrome--overactive bladder symptom score. Urology. 2006;68:318–323. doi: 10.1016/j.urology.2006.02.042. [DOI] [PubMed] [Google Scholar]
- 20.Barry MJ. Evaluation of symptoms and quality of life in men with benign prostatic hyperplasia. Urology. 2001;58(6 Suppl 1):25–32. doi: 10.1016/s0090-4295(01)01300-0. [DOI] [PubMed] [Google Scholar]
- 21.Kim YH, Seo JT, Yoon H. The effect of overactive bladder syndrome on the sexual quality of life in Korean young and middle aged women. Int J Impot Res. 2005;17:158–163. doi: 10.1038/sj.ijir.3901270. [DOI] [PubMed] [Google Scholar]
- 22.Rogers R, Bachmann G, Jumadilova Z, Sun F, Morrow JD, Guan Z, et al. Efficacy of tolterodine on overactive bladder symptoms and sexual and emotional quality of life in sexually active women. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19:1551–1557. doi: 10.1007/s00192-008-0688-6. [DOI] [PubMed] [Google Scholar]
- 23.Hajebrahimi S, Azaripour A, Sadeghi-Bazargani H. Tolterodine immediate release improves sexual function in women with overactive bladder. J Sex Med. 2008;5:2880–2885. doi: 10.1111/j.1743-6109.2008.00976.x. [DOI] [PubMed] [Google Scholar]