

Abstract
This study aimed to test a novel method of compliance measurement in Portuguese community pharmacy in Helicobacter pylori patients. A case series design was used where compliance indicators were electronically measured, aside with patients’ reports. Experienced adverse drug reactions, perceived benefit of therapy and quality of life were also measured. Mean compliance proportion was 56% and a positive impact on patients’ perceived health status was found. The method used was welcomed by community pharmacists, albeit having an influence on patients’ normal behaviour.
Keywords: Helicobacter pylori, Peptic ulcer, Compliance, Health status, Drug use, Community pharmacy services, Portugal
INTRODUCTION
The lifetime prevalence of peptic ulcer disease in industrialized countries is 10%, having a considerable social and public health impact.1 Helicobacter pylori chronic infection, together with NSAIDs consumption, has been described as the most common causes of peptic ulcer2 The use of H. pylori eradication therapy is, in this context, of major importance to tackle the burden of this disease. First line treatment for H. pylori eradication has been consensually establishes as the combination of a proton pump inhibitor (PPI) and two anti-infective agents.3 To achieve maximum effectiveness of therapy, optimal compliance is acknowledged as an essential determinant of success. Compliance has been defined as “the extent to which a patient follows doctor’s indications”.4 Several methods for measuring compliance currently exist, while it is acknowledged that all have their shortfalls; for such reason, it has been recommended to use at least two methods combined as a way to overcome this barrier.5 Physical and emotional distress are factors that interact with the development of peptic ulcer6 and, as such, considering the impact of such disease on perceived health status may be considered of great interest.
This study aims to contribute to the improvement of H. pylori eradication therapy through: the evaluation of compliance to triple therapy by means of electronic monitors (EMs); the measurement of the impact of such therapy on patients’ perceived health status; testing the acceptability and feasibility of using this method in the community pharmacy.
METHODS
Study design and period of data collection
The study design was a case series with prospective measurement of compliance to therapy indicators, patients’ reports of experienced adverse drug reactions and perceived benefit of therapy. The study period was between May 2002 and January 2003.
Sample considerations
A sample of regular pharmacy patients was invited to participate. Inclusion criteria were to have triple eradication therapy prescribed and agreeing to be followed-up for one month after finalising therapy. Therapies considered of interest to the study were the association of two anti-infective drugs and a proton pump inhibitor or an H2 receptor antagonist. Exclusion criteria were to have any mental or physical inability.
Data collection tools
Patients were initially informed about the study orally and provided with a detailed leaflet.
Declination to participate in the study was documented using a refusal form.
Patients accepting to participate formalised their agreement by signing a consent form.
The first questionnaire was administered by the pharmacist. The data collected through this tool consisted of: patients’ socio-demographic characteristics, physicians’ speciality, previous prescription of eradication therapy; awareness of being infected by H. pylori and of the reasons for the prescribed treatment; and diagnostic tests performed to confirm H. pylori infection.
The health status questionnaire SF-36 was used to collect baseline data and to evaluate the impact of therapy on patient’s perception of own health one month after finalising therapy.
One day after finalising therapy, patients answered a second questionnaire, where apart from the experiences with handling the medication, data on perceived benefit of therapy and experienced adverse drug reactions were also collected. Self-reported compliance was assessed at this moment asking the patient if he had ever forgotten to take any medication or if he had ever not taken it by his own initiative; how many pills he had taken per day, at what time and if he had always taken it at the right time. Information on concurrent medication was also collected to later evaluate if it could impact on different compliance behaviours.
Measuring compliance
The pharmacist informed the patient that his therapy would be placed into three separate bottles, which should be used during treatment duration, counselling him also on storage conditions. Special care was taken on the explanation that the patient should only open the bottles when taking the medicines. This study used a system for rigorous compliance measurement, an indirect method consisting of electronic monitoring entitled System MEMO CAPS - Medication Event Monitoring. This system uses a bottle container with a special cap containing a microcircuit prepared to register the date and time when the bottle is opened. These containers are used by the patient as a normal pillbox and collected data is then read by specific software.
Compliance indicators
The indicators used comprised taking compliance, dosing compliance and timing compliance, which were compared with self-reports.
○ Taking compliance: Percentage of prescribed dosages taken, calculated by: total number of medication events registered/ total number of prescribed dosages*100%. Example: a patient opened and closed his bottle 170 times; his prescribed regimen was twice daily, for a monitored period of 100 days. This patient’s taking compliance will be (170/200)*100% = 85%. This measure is useful as a compliance global measure. However, this measure is quite basic, since it does not inform on the inter-dosage intervals or on the days that there was an over or under-dosage; as such it is possible that the omitted dosages are covered by extra dosages taken in other days.
○ Correct dosing: Percentage of days where the correct number of prescribed dosages was taken, calculated by: number of days with medication events registered as prescribed/ total number of monitored days*100%. Example: a patient opened and closed his bottle 170 times; his prescribed regimen was twice daily for a monitored period of 100 days; however, only in 58 days there was register for two openings during 24h. Therefore his correct dosing will be: (58/100)*100%=58%. This variable is useful to investigate about the real daily use of therapy. It incorporates daily variability of dosing and it is not influenced by the dosing “catch-up”.
○ Timing compliance: It is calculated by: number of inter-dosage intervals of allowed duration/ number of inter-dosage intervals prescribed*100%. This estimation is performed allowing a default fluctuation of ±25% concerning the duration of action of the medicine, which can obviously be adjusted according to the medicine under study. For example, if a medicine is prescribed once daily, using the default fluctuation, the allowed inter-dosage will be between 18 and 30 h. Should there exist non-taken dosages, the inter-dosage intervals will be by definition lower than the prescribed, which means that the timing compliance doesn’t necessarily sum up to 100%. Example: a patient opened and closed his bottle 170 times; his prescription was for sulfalazine twice daily, for a monitoring period of 100 days. However only in 45 days the inter-dosage intervals had duration between 18 and 30 hours. The timing compliance will be: (45/199)*100%=26%. This measure takes into account inter-dosage intervals, which make sense under the pharmacological point of view.
Compliant versus non-compliant
Patients who had all these indicators proportions equal or over 80% were globally classified as compliant, whereas those who had them lower than 80% were classified as non-compliant. This measure was considered as a global classification score per individual, taking into account the three indicators for each of the three medicines.
Consistency between electronic and self-reported information
Three other variables were developed to assess the consistency of the two methods used to evaluate patients’ compliance. When the information reported by the patient was the same as the one registered electronically, information was considered consistent for each of the three indicators. Conversely, the opposite information was classified as inconsistent. Since the patient was being observed in the use of three medicines, the information was only considered consistent when there was absolute concordance in all three indicators, generating a global indicator relating to consistency.
Statistical analysis: Data was stored into a database using Access 2000 and statistical analysis was performed using the software SAS version 8.2 (SAS Institute). At a first stage the analysis consisted of quality control of information and at a second stage consisted of an exploratory analysis of data with development of new variables. Compliance indicators were directly estimated by the correspondent software Power View version 1.4 (AARDEX Ltd). Due to the sample size, the analysis consisted only of characterisation of the variables under study, by absolute and relative frequencies. For continuous variables, such as age, compliance proportions and the scores for each health status domain, central tendency measures were also calculated and their 95% confidence intervals, whenever considered relevant for the study objectives. Bivariate analysis was used to correlate some interest variables, such as the characterisation of health status among compliant and non-compliant individuals and comparison of compliance behaviours among incident and prevalent individuals concerning eradication therapy.
Health-status measurement
The impact of therapy on patients’ perception of their health status was evaluated through the use of the Short-Form 36 (SF36). For all different domains, a score was calculated at baseline and after one month. The difference between these values, for each domain, was assumed to be the measure of impact of therapy on patients’ health status. The average scores obtained in each follow-up moment were equally compared to evaluate if the difference had statistical significance. Additionally, the same type of analysis was undertaken comparing the two sub-groups of patients: compliant and non-compliant.
RESULTS
Pharmacists’ and patients’ participation
A total of 25 patients were recruited from 17 community pharmacies, extracted from the 30 initially agreeing to participate. There were no patient refusals or drop-outs. Two cases were excluded, one due to a change in prescribed therapy, which led to not meeting the inclusion criteria any longer, and another because the electronic registers exhibited improper use of the device. At the end of the study, there were therefore data from 23 patients suitable for analysis.
Patients’ characterization
The majority of patients recruited were female (74%). Most patients were aged between 46 and 65 (39%), and the extreme age groups (25-45 and ≥ 65) had equal proportions (30%). Primary or secondary school education were the most frequently found (65%), but there were still 22% of illiterate patients in the sample, whilst only 13% had university or college education.
Characterization of the exposition to H. pylori eradication therapy
The majority of patients were prescribed H. pylori eradication therapy for the first time (87%; n=20). Only 3 patients had been previously prescribed a similar therapy, 9, 12 and 24 months before. The therapeutic regime was instituted by a GP in 61% of cases; the remaining (n=9; 39%) having been prescribed by a gastroenterologist (n=5), an internal medicine specialist (n=2) and a medical oncologist (n=1); doctor’s speciality was missing in one case. Almost every patient (n=22; 96%) performed complementary diagnostic tests before being prescribed the eradication therapy.
Nearly three quarters of the patients (n=17; 74%) reported having been informed by their doctor about the status of the H. pylori infection, acknowledging an infective agent as responsible for the symptoms and justifying prescribed therapy. The analysis of the way patients express themselves may be considered most useful in the context of understanding their perceptions of illness and medicines; as such, some quotes extracted from interviews with patients are here presented (table 1).
Table 1.
Quotes extracted from patient interviews asking about the reason for therapy
| Why are you going to take this medication? |
|---|
| P1: They have detected H. pylori in the respiratory test |
| P3: Aphtes caused by bacteria |
| P4: Because of the problem, to cure it |
| P18: I don’t know |
| P9: I have gastritis and some little worms that need to be removed |
| P15. Because I had an active infection, like a throat infection, I needed to take antibiotic to kill the bacteria |
| P23: I bled, I did an endoscopy with biopsy and accused the presence of a bacteria |
These extracts demonstrate that whilst some patients acknowledge the involvement of bacteria, others seem to be unaware of their responsibility for symptoms presented, which is a fundamental aspect as it may condition the compliance behaviour of individuals.
Compliance to therapy
Three types of indicators were obtained through the use of electronic devices: taking compliance, timing compliance and dosing compliance. Each of these indicators was estimated for every medicine under study (total of 63; 3 per patient), where the results showed a greater dispersion in timing compliance, as depicted in table 2.
Table 2.
Compliance indicators
| Indicator | Mean (%) | Standard deviation (%) | [minimum; maximum] (%) | <80% (n; %) | ≥80% (n; %) |
|---|---|---|---|---|---|
| Taking compliance | 96.1 | 8.6 | [66.7; 121.4] | 5; 7.3 | 64; 92.7 |
| Dosing compliance | 91.9 | 14.8 | [12.5;100.0] | 14; 20.3 | 55; 79.7 |
| Timing compliance | 85.9 | 23.0 | [12.5;100.0] | 15; 21.7 | 54; 78.3 |
Considering compliant patients as those simultaneously presenting the 3 indicators with a value equal or above 80%, only 56% of the patients were classified as such (n=13).
Example of compliance indicators for a non-compliant patient
Among the 10 non-compliant patients, a case was selected to describe with greater detail the results obtained using MEMO CAPS. A 31-year old female, with frequency of secondary school, had an eradication therapy prescribed by her GP for the first time, following an endoscopy. The doctor informed her that she had an infection which was responsible for her gastric problem. The reason stated for such therapy was “aphtes caused by bacteria”. The therapeutic regime instituted was amoxicillin (1000 mg twice daily for 8 days), clarithromycin (500 mg twice daily for 8 days) and omeprazole (20 mg twice daily for 8 days and once daily for the following 40 days). [Figure 1]
Figure 1.
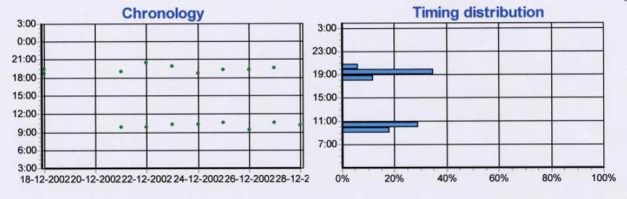
Calendar
Reporting her drug usage, the patient declared taking amoxicillin at 7H00 and at 20H00, except on plot for amoxicillin weekends, when the morning administration was postponed. There was no left over pill; the patient stated that she had never forgotten to take any medicine, but that she would sometimes take it at different hours. Medication was perceived as beneficial and no adverse drug effect was reported. Reading the information contained in the devices, registered data was verified to be consistent with the information provided by the patient. Amoxicillin’s taking compliance was 77%, dosing compliance was 73% and timing compliance was 43%.
Factors potentially associated with patient’s compliant behaviour
Some of the variables hypothesised to influence the way patients deal with their medication were the perceived benefit therapy, experience of adverse effects, and concurrent use of other medication, amongst others. Results found exploring the impact of each of these on compliance behaviour are presented in table 3.
Table 3.
Compliance to therapy, according to different factors
| Variables | Compliant | Non-compliant | P | |||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Gender | Female | 12 | 71 | 5 | 29 | 0.05 |
| Male | 1 | 17 | 5 | 83 | ||
| Age (years) | 25-64 | 9 | 53 | 7 | 47 | >0.05 |
| ≥65 | 4 | 57 | 3 | 43 | ||
| Educational level: | No qualifications (illiterate) | 3 | 60 | 2 | 40 | >0.05 |
| ≥ Primary school | 10 | 56 | 8 | 45 | ||
| Benefit from therapy perceived: | Yes | 8 | 57 | 6 | 43 | >0.05 |
| No | 4 | 50 | 4 | 50 | ||
| Experienced adverse effects: | Yes | 7 | 58 | 5 | 42 | >0.05 |
| No | 6 | 55 | 5 | 46 | ||
| Taken medication before: | Yes | 2 | 67 | 1 | 33 | >0.05 |
| No | 11 | 55 | 9 | 45 | ||
| Concurrent medication: | No (n=0) Yes | 3 | 38 | 5 | 63 | 0.05 |
| (n ≥ 1) | 9 | 69 | 4 | 31 | ||
| Agreement in hour of taking: | Yes | 8 | 73 | 3 | 27 | 0.05 |
| No | 5 | 42 | 7 | 58 | ||
Despite the limited capacity of the analysis due to sample size, overall trends may be observed: women, patients aged between 46 and 64 years and the less literate were found to be more compliant. Patients prescribed more drugs and those with eradication therapy with daily dosages at the same hour were found to be more compliant. Patients perceiving therapy as beneficial were more compliant and conversely those experiencing adverse drug effects were less compliant.
Comparison of compliance results measured by self-report and by electronic monitoring
Patients tended to report quite accurately what happened, where there was 70% of agreement in information on timing compliance and 52% in taking compliance. Greater discrepancies were found in dosing compliance, where non-consistent information corresponded to 52% of the cases.
Differential compliance by medicine class
The lowest compliance proportions were found for the imidazoles (88.5%, 81.5% and 70.7% for taking, dosing and timing compliance respectively). Possible reasons include the fact that these drugs are administered three times daily and/or time of dosage is frequently non-coincident with other antibiotics and/or PPIs; these drugs have higher incidence of adverse drug reactions, such as metallic taste; the perceived benefit from this class is not so clear to patients under treatment.
Impact of therapy on patients’ perceived health status
Comparing perceived health status at baseline and one month after finalizing therapy, a positive impact in most domains was found (table 4); however, this difference was only significant for the physical functioning (PF) domain. A negative impact was found for the domains measuring health transformation (HT) and the emotional role (RE).
Table 4.
Quality of life domains at times of follow-up
| Domains | t0 | t1 | t1-t0 | |||
|---|---|---|---|---|---|---|
| Average (%) | Standard deviation (%) | Average (%) | Standard deviation (%) | Average (%) CI 95% | P | |
| Health Transformation (HT) | 3.4 | 0.9 | 2.6 | 0.9 | -0.8 [-1.3;-0.2] | 0.0077 |
| General Health (GH) | 45.7 | 19.2 | 48.6 | 19.0 | 3.0 [-4.8;10.7] | 0.6516 |
| Physicial Functioning (PF) | 65.8 | 27.0 | 78.4 | 16.7 | 13.7 [3.3;24.1] | 0.0123* |
| Role Physical (RP) | 68.9 | 26.3 | 81.0 | 21.1 | 12.2 [-3.1;27.5] | 0.1485 |
| Social Functioning (SF) | 63.3 | 27.2 | 72.9 | 24.5 | 9.5 [-5.6;29.2] | 0.2310 |
| Role Emotional (RE) | 78.2 | 21.4 | 74.6 | 25.9 | -3.6 [-18.7;24.7] | 0.6012 |
| Vitality (VT) | 44.4 | 22.8 | 54.9 | 25.3 | 10.4 [-1.9;22.8] | 0.111 |
| Mental Health (MH) | 43.3 | 22.3 | 56.4 | 31.0 | 14.2 [-1.0;29.4] | 0.069 |
| Bodily Pain (BP) | 53.6 | 30.5 | 65.6 | 23.7 | 12.0 [-5.2;29.2] | 0.138 |
DISCUSSION
None of the patients withdrew from the study due to handling problems nor was any device damaged. There were no refusals, but this can, to a great extent, be attributed to the selection method used, as one of the inclusion criteria was to be a regular customer.
The compliance indicator showing a higher proportion of disagreement with patient self-report was dosing compliance. This might be due to the fact that it is more difficult for the patient to remember omitted dosages; it can also be hypothesised that such behaviour might be intentional leading to patient’s reluctance in admitting it to their pharmacist. It is interesting to notice that although low timing compliance proportions were observed, these were also reported by patients, leading to suppose that patients do not consider this aspect as a determinant of therapeutic success.
Electronic measurement has been described as most suitable for long-term therapies, particularly those with high costs.7 In this study, electronic monitoring was used for an acute situation, where no wash-out period was used. This implies that patients were aware of being under observation, which may affect their normal behaviour, leading to the Hawthorne effect.8 This is supported by the following patient’s quote: “although having experienced adverse effects, I continued with this medication because I was participating in this study”.
In an observational study, where the aim is to measure compliance behaviours to short-term therapies, one possible way to minimise this bias would be to evaluate a similar sample of patients through another method, such as pill-count. However, this solution would only allow characterization of taking compliance.
One of the findings in the current study highlights the need to improve doctor-patient communication. Some patients where timing compliance was lower than 80% were totally complying with what they had been told, i.e., taking medicines with meals; such direction of use does not necessarily imply that the resulting inter-dosage intervals should be 8 h or 12 hours (for 3 and 2 meals, respectively).
One important limitation of this study was the study design chosen, as a cross-sectional approach limits the ability to explore the impact of some of the studied variables on compliance, as the direction of cause and effect is not clear and can therefore result in misleading interpretations of phenomena, such as disregarding the possibility of protopathic bias; patients’ perceptions (e.g. perceived benefit from therapy) are a good example, where the researcher is not aware if these influenced behaviour (i.e. compliance) or vice-versa.
The measurement of perceived health-status before and after eradication therapy was intended as an indirect way of evaluating medication effectiveness. There was indeed an improvement in most domains and the lack of statistical significance can be, at least partly, explained by sample size.
CONCLUSIONS
The use of electronic devices for measuring compliance to H. pylori eradication therapy in a sample of Portuguese community pharmacies was feasible for regular patients of such pharmacies. This can be assumed since no patient refused to participate, no patient dropped-out and no patient damaged the devices during the study. However, it must be acknowledged that such method may result in overestimation of compliance proportions as patients are aware they are being observed. In acute therapies, this method may be better considered as a stimulating strategy9 rather than a measuring tool. Conversely, used in chronic conditions, it may be used for measurement purposes provided the appropriate wash-out period is guaranteed.
H. pylori eradication therapy seems to have had an impact on patients’ health-status, although it was not possible to show statistical significance in most domains.
Contributor Information
Ana Paula Martins, Centre for pharmacoepidemiology Research (CEFAR-ANF) and Faculty of Pharmacy, University of Lisbon (Portugal).
Ana Patrícia Ferreira, Centre for pharmacoepidemiological Research (CEFAR-ANF).
Filipa Alves da Costa, Centre for pharmacoepidemiological Research (CEFAR-ANF) and Instituto Superior de Ciências da Saúde Egas Moniz, Lisbon (Portugal).
José Cabrita, Faculty of Pharmacy, University of Lisbon (Portugal)..
References
- 1.Sonnenberg A. Everhart J.E. The prevalence of self-reported peptic ulcer in the United States. Am J Public Health. 1996;86(2):200–205. doi: 10.2105/ajph.86.2.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Laporte J.R, Carne X, Vidal X, Moreno V, Juan J. Upper gastrointestinal bleeding in relation to previous use of nonsteroidal anti-inflammatory drugs. Catalan Countries Study on Upper Gastrointestinal Bleeding. Lancet. 1991;337(8733):85–89. doi: 10.1016/0140-6736(91)90744-a. [DOI] [PubMed] [Google Scholar]
- 3.Unge P. What other regimens are under investigation to treat Helicobacter pylori infection? Gastroenterology. 1997;113:137–148. doi: 10.1016/s0016-5085(97)80027-3. [DOI] [PubMed] [Google Scholar]
- 4.Sackett D. L, Haynes R. B. John Hopkins University Press; Baltimore: 1976. Compliance with therapeutic regimens. [Google Scholar]
- 5.Farmer K. C. Methods for Measuring and Monitoring Medication Regimen Adherence in Clinical Trials and Clinical Practice. Clin Ther. 1999;21(6):1074–1090. doi: 10.1016/S0149-2918(99)80026-5. [DOI] [PubMed] [Google Scholar]
- 6.Levenstein S, Kaplan GA, Smith MW. Psychological predictors of peptic ulcer incidence in the Alameda County Study. J Clin Gastroenterol. 1997;24(3):140–146. doi: 10.1097/00004836-199704000-00004. [DOI] [PubMed] [Google Scholar]
- 7.Cramer J. A, Spilker B. Raven Press; New York: 1991. Patient Compliance in Medical Practice and Clinical Trials. [Google Scholar]
- 8.Hennekens C. H, Buring J. E. Descriptive studies in Epidemiology in Medicine. In: Mayrent S. L, editor. Little, Brown and Company; Boston: 1987. [Google Scholar]
- 9.World Health Organisation. Geneva: 2003. Adherence to long-term therapies: evidence for action. [Google Scholar]