

Abstract
Objective
Symptomatic thoracic disc herniation often requires prompt surgical treatment to prevent neurological deterioration and permanent deficits. Anterior approaches offer direct visualization and access to the herniated disc and anterior dura but require access surgeons and are often associated with considerable postoperative pain and pulmonary complications. A disadvantage with using posterior approaches in the setting of central calcified thoracic disc herniation however, has been the limited visualization of anterior dura and difficulty to accurately assess the extent of decompression.
Methods
We report our experience with intraoperative ultrasound (US) guidance during a modified posterior transpedicular approach for removal of a central calcified thoracic disc herniation with a review of pertinent literature.
Results
The herniated thoracic disc was successfully removed with posterior approach with the aid of intraoperative US. The patient had significant neurological improvement at three months follow-up.
Conclusion
Intraoperative ultrasound is a simple yet valuable tool for real-time imaging during transpedicular thoracic discectomy. Visualization provided by intraoperative US increases the safety profile of posterior approaches and may make thoracotomy unnecessary in a selected group of patients, especially when a patient has existing pulmonary disease or is otherwise not medically fit for the transthoracic approach.
Keywords: Calcified disc, Discectomy, Intraoperative ultrasound, Thoracic disc herniation, Transpedicular
INTRODUCTION
Symptomatic disc herniation located in the thoracic spine is a relatively uncommon disease with an estimated annual incidence of 1:1000 to 1:10000003,9,10). On the other hand, it is thought to represent 0.25 to 0.75% of all symptomatic disc herniations, making it common enough so that any spine surgeon will occasionally face this problem2,3). These patients may present with subtle complaints of localized or radiated pain as well as severe myelopathy with motor and sensory deficits, usually requiring prompt surgical treatment1,6,23).
Since the first description of a herniated thoracic disc by C. A. Key in 1838, surgical management of thoracic disc herniation (TDH) has proven to be a challenge. In Mixter and Barr's famous 1934 report on surgery for disc herniation, four patients had TDHs-of those, three underwent surgery with disastrous results : two of them developed paraplegia postoperatively while the third died of unknown causes10,21). Poor results such as these were replicated throughout the early and mid-twentieth century and soon recognized to be secondary to cord manipulation during a laminectomy-only posterior approach17,18). Consequently, several posterolateral and anterior approaches were developed to avoid cord manipulation, such as lateral extracavitary12) and its variant, costotransversectomy15), transthoracic-transpleural16), transpedicular23), video-assisted thoracoscopic19) and transthoracic-retropleural, either open20) or minimally-invasive28). Today, cord manipulation is recognized as extremely deleterious and kept to a minimum; accordingly, neurologic morbidity rates have decreased steeply after these new techniques were introduced. Other complications are more commonly encountered today, such as those resulting from a transthoracic exposure (pleural effusion, post-thoracotomy pain, etc.) or incomplete cord decompression1,3,9,29).
Given the limited visualization of the anterior dura afforded by posterolateral approaches and the frequently calcified nature of TDHs, the preferred approach for midline TDHs is anteriorly through the thoracic cavity, either transpleural or, as recently described, retropleural3,10,29). We present a case in which the application of intraoperative ultrasound (US) enabled us to successfully perform a transpedicular approach for a midline, calcified TDH and discuss its potential applications and deficiencies.
CASE REPORT
Presentation
A 41-year-old woman with a prior medical history of Coccidioides meningitis requiring a ventriculoperitoneal shunt (VPS) in 2010, presented with a complaint of inability to walk, involuntary movements of her lower extremities and nocturia for 4 months. On exam, she could only stand with assistance and was unable to walk more than 2-3 steps (Nurick 4). Spastic paraparesis (MRC 4/5, Nurick 4) with patellar and ankle clonus and up-going toes to plantar stimulation were noted. Sensation was normal, as well as her upper extremity exam. A diagnosis of thoracic myelopathy was made and computed tomography (CT) and magnetic resonance imaging (MRI) were obtained. A large, calcified, midline TDH was found at T7-8 causing cord deformation and signal change (Fig. 1). Brain imaging was also obtained and remained unchanged compared to after her VPS three years before.
Fig. 1.

Preoperative CT (A and B) and MR (C and D) demonstrate a large, calcified, midline disc herniation at T7-8 with significant cord signal change.
Surgical technique
Following endotracheal intubation and continuous blood pressure monitoring, the patient was positioned prone on the open Jackson frame. Care was taken at all times to maintain a mean blood pressure of at least 80 mm Hg and intraoperative somatosensory evoked potential (SSEP) and motor evoked potential (MEP) monitoring were set up. The T7-8 level was localized with fluoroscopy and marked in the skin. A midline, 7 cm longitudinal incision centered on that projection was made. The spinous, transverse and articular processes of T6 through T8 were exposed with the Bovie cautery and vertebral levels were confirmed once again with anteroposterior fluoroscopy. Laminectomies from T6 to T8 were performed with a high-speed bur and epidural bleeding controlled with a combination of hemostatic agents. At this point, the ultrasound probe (UST-9120 3.75-10 MHz Multi-Frequency Convex probe, Hitachi Aloka, Tokyo, Japan) was brought into the field and utilized to localize the anterior TDH, thus confirming the T7-8 level again (Fig. 2A, B). The US convex probe was covered with gel and placed inside a sterile drape. This probe was brought intermittently into the operative field for use by the surgeon himself, when the cavity would be filled with warm saline. Care was maintained at all times to provide a minimum working distance of 3 cm to the exposed dura.
Fig. 2.
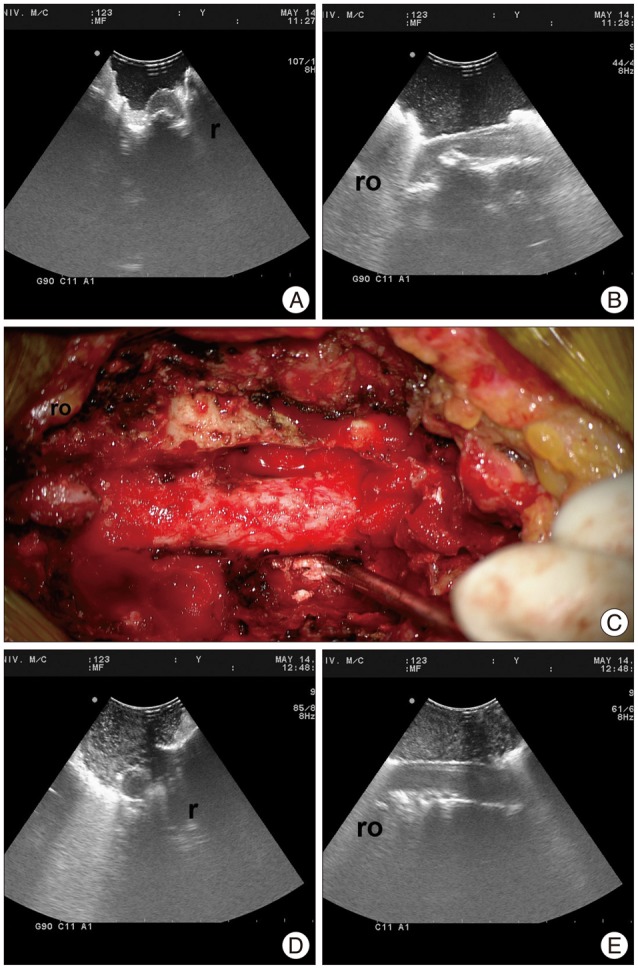
Intraoperative coronal (A) and sagittal (B) US images demonstrate a large anterior disc herniation causing cord deformation. Fragments of the calcified thoracic disc herniation (C) are pushed down into the vertebral body cavity and removed piecemeal through a left transpedicular approach without contacting the dura until US guidance (D and E) demonstrate effective cord decompression. r : right side, ro : rostral, US : ultrasound.
A transpedicular approach was then performed as described by Patterson and Arbit23). The left T7 inferior articular process, T8 superior articular process and pedicle were removed with a high-speed bur thus completely exposing the left T8 nerve root and T7-8 disc (Fig. 2C). Ligation of the T8 nerve root was not necessary as it was found in its typical location, on the rostral part of the foramen. The T7-8 disc was incised with a #11 blade and, as expected, little material could be obtained. The calcified, midline TDH could be palpated and delimited with a variety of angled curettes and instruments. We thus proceeded to create a cavity in the T8 vertebral body as described by Jefferson and utilized a combination of angled instruments to dissect the calcified mass from the anterior dura; as this plane was delimited, the calcified mass was pushed anterior into the crevice and then removed piecemeal13). Alternatively, an angled instrument was also inserted from the opposite side and used to push the mass towards the left, where it could be manipulated; this did not require any additional removal of the right articular processes beyond a standard laminectomy (Fig. 2C). The US probe was frequently brought into the field to assess cord decompression progress until the calcified TDH had been completely resected (Fig. 2D, E).
No objective instability was observed; as the right T7-8 zygapophysial joint was rendered almost intact and the vertebral body cavity was estimated at less than 10% of the vertebral body, an instrumented fusion was not considered necessary. Estimated blood loss (EBL) was 150 mL and the procedure lasted 2 hours. SSEP and MEP monitoring remained unchanged and the patient woke up from surgery at her neurological baseline. She was discharged home on postoperative day 3 and gait improved steadily over the first few days. Satisfactory cord decompression was confirmed on a postoperative CT study (Fig. 3). Three months after surgery, she is able to walk unassisted, though her gait has not returned to normal (Nurick 2).
Fig. 3.

Postoperative sagittal (A) and axial (B) CT with ample decompression of the spinal cord. T8 vertebral body defect is estimated at 10% of its total volume.
DISCUSSION
Surgical approaches for TDH have evolved dramatically since the first surgical report by Adson in 19224,13). While laminectomy alone has been abandoned due to dismal neurological outcomes, the time-honored open transthoracic, transpleural approach still poses considerable challenges-an access surgeon, double-lumen endotracheal intubation, ipsilateral lung deflation and a chest tube are typically required. In a recent series of open transthoracic cases, Ayhan et al. report good neurological outcomes (90% improved or stabilized myelopathy) but some of the reported figures are concerning that this approach may not be applicable to the sickest patients : 605 mL mean EBL, four days of chest drainage and seven days in-hospital stay on average3). Pulmonary complications and post-thoracotomy pain are other concerns as well10). Anterior alternatives have then evolved in order to obviate some of these problems. VATS was described by Mack et al. for TDHs and though less invasive than the open alternative, still requires an access surgeon, lung deflation and a chest tube while some additional training in utilizing 2D optics is required3,19). The latest development in anterior approaches for TDH has been the minimally-invasive (MIS) lateral approach through a tubular channel. These may be performed retro- or transpleural but have been described without the assistance of the access surgeon, double lumen intubation or lung deflation7,28,29). A chest tube may or may not be required depending on the surgeon's preference; neurological outcomes have been very good and EBL better or equivalent to VATS3,28,29). Long working distances also pose less of a challenge today since special retractors have been made available, though they may still be a concern for surgeons unfamiliar with tubular techniques-in the reported patient, working distances would be in the order of 140 mm. Regardless of the type of anterior approach, the risk of injury to chest wall vessels exists and instances of such episodes are inferred from major report quoted above-maximum EBL in each series ranged from 1500 to 3000 mL1,3,29).
Posterolateral approaches to TDHs were developed in the 1960s and their applications have been greatly expanded. They are preferable, when feasible, to any of the anterior approaches and have been reported in a minimally-invasive variation as well5,8,10,14). However, visualization of the anterior dura is limited and posterolateral approaches have created a set of complications of their own, especially inadequate anterior decompression of the spinal cord9). Posterolateral approaches are therefore typically reserved for those "soft" TDHs located off the midline8,9,10). In order to circumvent this visualization problem, we applied ultrasound guidance to the transpedicular approach previously described by Patterson and Arbit23). Intraoperative US guidance in spine surgery was first reported in 1978 by Reid for intrinsic cord lesions but has been since applied to both anterior and posterior approaches for degenerative disease across all vertebral segments11,22,24,25). It is an inexpensive and accurate method to supply the surgical team with real-time imaging without the use of ionizing radiation. When compared to intraoperative CT, minimal training and equipment is required and probe utilization is intuitive to any surgeon familiar with spine anatomy27). US guidance has been applied once to TDH by Stone et al. to localize an intradural disc herniation during a different posterolateral approach26). This is, however, the first time it is applied to a transpedicular approach to assess cord decompression in a midline calcified TDH; as such, it is applicable to any open posterolateral approach and should be considered an important surgical adjunct.
Surgical management of a midline, calcified TDH can be a daunting task for even the most experienced surgeons. Posterolateral approaches, especially the transpedicular approaches, have become the procedure of choice for off-midline TDHs. The utilization of intraoperative US further expands its application to encompass midline, calcified TDHs while enabling the surgeon to avoid cord manipulation. It is still unclear to us if this technique could be applied to every midline TDH, particularly those suspected of having an intradural component; only continued utilization will answer this question. This is a viable alternative of midline TDHs especially for surgeons unfamiliar with tubular techniques or patients who cannot risk the potential complications of an anterior approach.
CONCLUSION
Intraoperative ultrasound is a simple yet valuable tool that can provide real-time visualization of the dura-disc interface, objective assessment of spinal cord decompression and disc removal during transpedicular thoracic discectomy when direct visualization is limited. Spine surgeons should take this valuable tool into consideration when choosing surgical approaches for thoracic disc herniations. The real-time visualization provided by intraoperative US increases the safety profile of posterior approaches and may make thoracotomy unnecessary in a selected group of patients, especially when a patient has existing pulmonary disease or is otherwise not medically fit for the transthoracic approach.
References
- 1.Anand N, Regan JJ. Video-assisted thoracoscopic surgery for thoracic disc disease : Classification and outcome study of 100 consecutive cases with a 2-year minimum follow-up period. Spine (Phila Pa 1976) 2002;27:871–879. doi: 10.1097/00007632-200204150-00018. [DOI] [PubMed] [Google Scholar]
- 2.Arce CA, Dohrmann GJ. Thoracic disc herniation. Improved diagnosis with computed tomographic scanning and a review of the literature. Surg Neurol. 1985;23:356–361. doi: 10.1016/0090-3019(85)90206-x. [DOI] [PubMed] [Google Scholar]
- 3.Ayhan S, Nelson C, Gok B, Petteys RJ, Wolinsky JP, Witham TF, et al. Transthoracic surgical treatment for centrally located thoracic disc herniations presenting with myelopathy : a 5-year institutional experience. J Spinal Disord Tech. 2010;23:79–88. doi: 10.1097/BSD.0b013e318198cd4d. [DOI] [PubMed] [Google Scholar]
- 4.Benson MK, Byrnes DP. The clinical syndromes and surgical treatment of thoracic intervertebral disc prolapse. J Bone Joint Surg Br. 1975;57:471–477. [PubMed] [Google Scholar]
- 5.Bilsky MH. Transpedicular approach for thoracic disc herniations. Neurosurg Focus. 2000;9:e3. doi: 10.3171/foc.2000.9.4.4. [DOI] [PubMed] [Google Scholar]
- 6.Carson J, Gumpert J, Jefferson A. Diagnosis and treatment of thoracic intervertebral disc protrusions. J Neurol Neurosurg Psychiatry. 1971;34:68–77. doi: 10.1136/jnnp.34.1.68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chi JH, Dhall SS, Kanter AS, Mummaneni PV. The Mini-Open transpedicular thoracic discectomy : surgical technique and assessment. Neurosurg Focus. 2008;25:E5. doi: 10.3171/FOC/2008/25/8/E5. [DOI] [PubMed] [Google Scholar]
- 8.Deviren V, Kuelling FA, Poulter G, Pekmezci M. Minimal invasive anterolateral transthoracic transpleural approach : a novel technique for thoracic disc herniation. A review of the literature, description of a new surgical technique and experience with first 12 consecutive patients. J Spinal Disord Tech. 2011;24:E40–E48. doi: 10.1097/BSD.0b013e318220af6f. [DOI] [PubMed] [Google Scholar]
- 9.Dickman CA, Rosenthal D, Regan JJ. Reoperation for herniated thoracic discs. J Neurosurg. 1999;91(2 Suppl):157–162. doi: 10.3171/spi.1999.91.2.0157. [DOI] [PubMed] [Google Scholar]
- 10.Fessler RG, Sturgill M. Review : complications of surgery for thoracic disc disease. Surg Neurol. 1998;49:609–618. doi: 10.1016/s0090-3019(97)00434-5. [DOI] [PubMed] [Google Scholar]
- 11.Gooding GA, Boggan JE, Weinstein PR. Intraoperative sonography during lumbar laminectomy : work in progress. AJNR Am J Neuroradiol. 1984;5:751–753. [PMC free article] [PubMed] [Google Scholar]
- 12.Hulme A. The surgical approach to thoracic intervertebral disc protrusions. J Neurol Neurosurg Psychiatry. 1960;23:133–137. doi: 10.1136/jnnp.23.2.133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jefferson A. The treatment of thoracic intervertebral disc protrusions. Clin Neurol Neurosurg. 1975;78:1–9. doi: 10.1016/s0303-8467(75)80002-3. [DOI] [PubMed] [Google Scholar]
- 14.Jho HD. Endoscopic microscopic transpedicular thoracic discectomy. Technical note. J Neurosurg. 1997;87:125–129. doi: 10.3171/jns.1997.87.1.0125. [DOI] [PubMed] [Google Scholar]
- 15.Kasliwal MK, Deutsch H. Minimally invasive retropleural approach for central thoracic disc herniation. Minim Invasive Neurosurg. 2011;54:167–171. doi: 10.1055/s-0031-1284400. [DOI] [PubMed] [Google Scholar]
- 16.Lesoin F, Rousseaux M, Autricque A, Reesaul Y, Villette L, Clarisse J, et al. Thoracic disc herniations : evolution in the approach and indications. Acta Neurochir (Wien) 1986;80:30–34. doi: 10.1007/BF01809554. [DOI] [PubMed] [Google Scholar]
- 17.Logue V. Thoracic intervertebral disc prolapse with spinal cord compression. J Neurol Neurosurg Psychiatry. 1952;15:227–241. doi: 10.1136/jnnp.15.4.227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Love JG, Kiefer EJ. Root pain and paraplegia due to protrusions of thoracic intervertebral disks. J Neurosurg. 1950;7:62–69. illust. doi: 10.3171/jns.1950.7.1.0062. [DOI] [PubMed] [Google Scholar]
- 19.Mack MJ, Regan JJ, Bobechko WP, Acuff TE. Application of thoracoscopy for diseases of the spine. Ann Thorac Surg. 1993;56:736–738. doi: 10.1016/0003-4975(93)90966-l. [DOI] [PubMed] [Google Scholar]
- 20.McCormick PC. Retropleural approach to the thoracic and thoracolumbar spine. Neurosurgery. 1995;37:908–914. doi: 10.1227/00006123-199511000-00009. [DOI] [PubMed] [Google Scholar]
- 21.Mixter WJ, Barr JS. Rupture of the intervertebral disc with involvement of the spinal canal. N Engl J Med. 1934;211:210–215. [Google Scholar]
- 22.Montalvo BM, Quencer RM, Brown MD, Sklar E, Post MJ, Eismont F, et al. Lumbar disk herniation and canal stenosis : value of intraoperative sonography in diagnosis and surgical management. AJR Am J Roentgenol. 1990;154:821–830. doi: 10.2214/ajr.154.4.2107683. [DOI] [PubMed] [Google Scholar]
- 23.Patterson RH, Jr, Arbit E. A surgical approach through the pedicle to protruded thoracic discs. J Neurosurg. 1978;48:768–772. doi: 10.3171/jns.1978.48.5.0768. [DOI] [PubMed] [Google Scholar]
- 24.Raynor RB. Intraoperative ultrasound for immediate evaluation of anterior cervical decompression and discectomy. Spine (Phila Pa 1976) 1997;22:389–395. doi: 10.1097/00007632-199702150-00006. [DOI] [PubMed] [Google Scholar]
- 25.Reid MH. Ultrasonic visualization of a cervical cord cystic astrocytoma. AJR Am J Roentgenol. 1978;131:907–908. doi: 10.2214/ajr.131.5.907. [DOI] [PubMed] [Google Scholar]
- 26.Stone JL, Lichtor T, Banerjee S. Intradural thoracic disc herniation. Spine (Phila Pa 1976) 1994;19:1281–1284. doi: 10.1097/00007632-199405310-00016. [DOI] [PubMed] [Google Scholar]
- 27.Tian W, Weng C, Liu B, Li Q, Sun YQ, Yuan Q, et al. Intraoperative 3-dimensional navigation and ultrasonography during posterior decompression with instrumented fusion for ossification of the posterior longitudinal ligament in the thoracic spine. J Spinal Disord Tech. 2013;26:E227–E234. doi: 10.1097/BSD.0b013e318286ba39. [DOI] [PubMed] [Google Scholar]
- 28.Tovi D, Strang RR. Thoracic intervertebral disk protrusions. Acta Chir Scand Suppl. 1960;Suppl 267:1–41. [PubMed] [Google Scholar]
- 29.Uribe JS, Smith WD, Pimenta L, Härtl R, Dakwar E, Modhia UM, et al. Minimally invasive lateral approach for symptomatic thoracic disc herniation : initial multicenter clinical experience. J Neurosurg Spine. 2012;16:264–279. doi: 10.3171/2011.10.SPINE11291. [DOI] [PubMed] [Google Scholar]