

Abstract
Context
As high school female athletes demonstrate a rate of noncontact anterior cruciate ligament (ACL) injury 3–6 times higher than their male counterparts, research suggests that sagittal-plane hip strength plays a role in factors associated with ACL injuries.
Objective
To determine if gender or age affect hip-abductor strength in a functional standing position in young female and male athletes.
Design
Prospective cohort design.
Setting
Biomechanical laboratory.
Participants
Over a 3-y time period, 852 isokinetic hip-abduction evaluations were conducted on 351 (272 female, 79 male) adolescent soccer and basketball players.
Intervention
Before testing, athletes were secured in a standing position, facing the dynamometer head, with a strap secured from the uninvolved side and extending around the waist just above the iliac crest. The dynamometer head was positioned in line with the body in the coronal plane by aligning the axis of rotation of the dynamometer with the center of hip rotation. Subjects performed 5 maximum-effort repetitions at a speed of 120°/s. The peak torque was recorded and normalized to body mass. All test trials were conducted by a single tester to limit potential interrater test error.
Main Outcome Measure
Standing isokinetic hip-abduction torque.
Results
Hip-abduction torque increased in both males and females with age (P < .001) on both the dominant and nondominant sides. A significant interaction of gender and age was observed (P < .001), which indicated that males experienced greater increases in peak torque relative to body weight than did females as they matured.
Conclusions
Males exhibit a significant increase in normative hip-abduction strength, while females do not. Future study may determine if the absence of similar increased relative hip-abduction strength in adolescent females, as they age, may be related to their increased risk of ACL injury compared with males.
Keywords: biomechanics, hip strength, ACL injury, knee valgus
High school female athletes demonstrate a rate of noncontact anterior cruciate ligament (ACL) injury 3–6 times higher than their male counterparts.1 Female athletes demonstrate increased measures of knee-valgus angles and torques when performing dynamic tasks associated with this increased risk of injury.2–5 These increased measures of dynamic lower extremity valgus increase the risk for ACL injury in adolescent female athletes.6 The major hip abductors (gluteus maximus, gluteus medius, and tensor fasciae latae) assist in controlling the varus–valgus position of the knee joint7–10 and the associated dynamic valgus alignments and torques. A recent analysis of 117 athletes demonstrated that hip-abduction strength was a significant predictor of initial contact and peak knee-valgus angles during a box-drop vertical-jump task.11 Cumulatively, these data indicate that deficits in relative hip-abduction strength may be partially correlated to increased frontal-plane movement of the knee and risk of knee injury in female athletes.
Hip strength is usually assessed with handheld isometric dynamometers or isokinetic dynamometers with the subject lying in non-weight-bearing positions (lying supine or on side).12–16 Cahalan et al17 examined isokinetic hip abduction in a standing position, but that study was not performed on the higher-risk athletic adolescent population. The assessment of hip strength with the previously mentioned techniques (side-lying or supine) may not be ideal for determining the relationship of hip strength to noncontact ACL injuries that occur during dynamic weight bearing. A limitation to isometric-dynamometer measurements is that hip-abduction torque is evaluated at a single discrete angle within the range of motion. In addition, static isometric torque measurements may not be as closely related to injury as dynamic strength measures, typically performed isokinetically at faster, more functional speeds.18 In addition, isokinetic testing in a lying position may not be the most relevant test, as it does not represent a functional position related to the demands of the athlete. Thus, assessment of dynamic hip strength in a position that more closely mimics a more functional position is warranted to better determine potential ACL injury risk factors that may be related to hip-abductor strength.
Recent investigations have indicated the importance of hip-abduction strength to dynamic valgus alignments that increase ACL injury risk.6,8,9,11 Associations of strength deficits to mechanism of ACL injury have typically focused on quadriceps and hamstrings strength, although the association of hip strength to ACL injury risk has not been extensively studied.19 Studies specifically evaluating hip-abduction strength have not reported age differences for adolescents in either normal or patient populations.16,20–22 Several studies have demonstrated that as females mature they tend not to experience a concurrent growth in muscle strength and power to the same degree as males.23,24 This phenomenon has been observed in many different measures such as vertical jump and isokinetic knee-flexion/extension torque.23,24 The lack of a neuromuscular spurt with maturity may also be a risk factor for ACL injury.25,26
The purpose of this study was to perform a hip-abductor strength assessment, in a functional position, on male and female athletes to determine if gender and age differences in hip-abductor strength were present in young athletes. The first hypothesis was that females would have decreased hip-abductor strength normalized to body mass compared with males. The second hypothesis was that as males increased in chronological age they would demonstrate a concomitant increase in relative hip-abduction strength while females would not show a similar increase in hip-abduction strength as they aged.
Methods
Participants
Over a 3-year time period, 852 evaluations were conducted on 351 (272 female, 79 male) adolescent soccer and basketball players. The age (mean ± SD) of the participants was 14.0 ± 2.2 years for the females and 13.65 ± 1.6 for the males. Height and mass means for the subjects were 161.4 ± 7.8 cm and 55.4 ± 11.0 kg, respectively, for the females, and 167.4 ± 13.3 cm and 57.2 ± 14.5 kg for the males. The dominant leg was determined for each subject by the leg the subject used to kick a ball as far as possible.3 This study was approved by the Cincinnati Children’s Hospital Medical Center institutional review board. Parents or guardians signed informed consent before the subjects’ participation in the study. After the informed consent was obtained, height, clothed weight, and dominant leg were determined.
Procedures
The testing was performed on a Biodex System 3 Pro isokinetic dynamometer (Biodex Medical Systems, Shirley, NY). The subjects were instructed to stand facing the dynamometer head. The athletes were secured with a strap originating from the stationary platform on the uninvolved side and extending around the waist above the iliac crest (Figure 1). The dynamometer head was aligned in parallel with the coronal plane of the body, with the axis of rotation of the dynamometer aligned with the center of rotation of the hip (Figure 2). The test limb was secured to the dynamometer head with a custom-made hip attachment with the strap extending from the moving arm positioned immediately superior to the knee. The subjects were instructed to grasp the top of the dynamometer head for support and to minimize movement of the torso (Figures 1–3).
Figure 1.
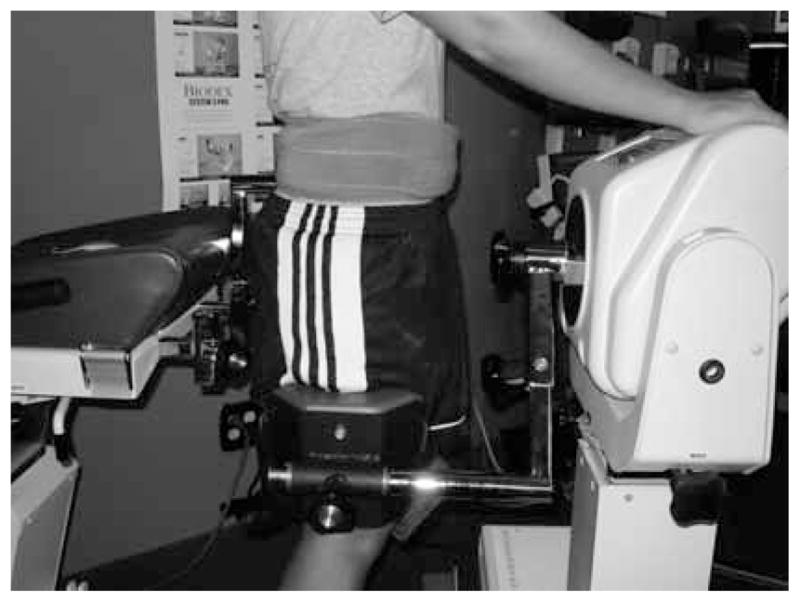
Example of method used to secure subject at the waist.
Figure 2.
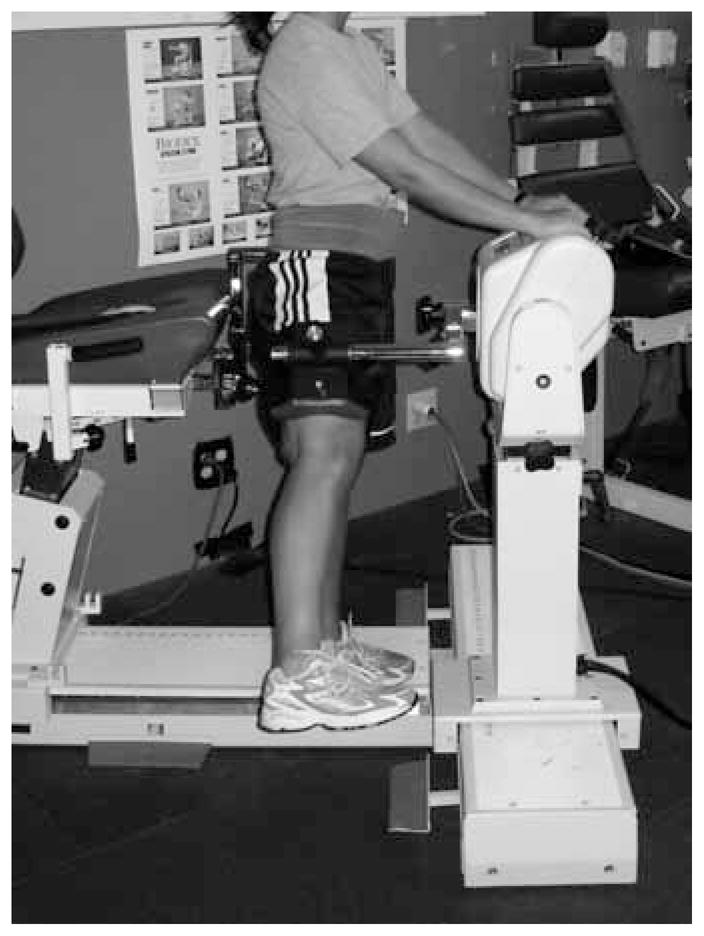
Example of dynamometer-head positioning.
Figure 3.
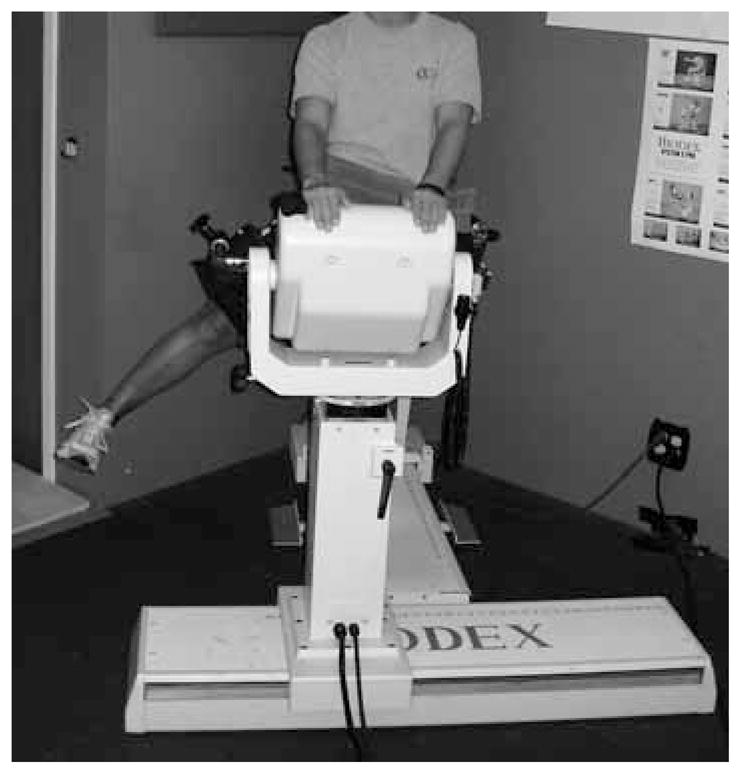
Example of test being executed from frontal view.
Before data collection, subjects were familiarized with how to perform the test and were allowed to perform 5 to 10 submaximal repetitions until they became comfortable with the testing technique and the tester confirmed appropriate technique. The athletes were then asked to perform 5 repetitions with maximum exertion at 120°/s. Previous isokinetic assessments of hip strength have been executed at various speeds, ranging from 30°/s to 210°/s in the side-lying position.14,16,20–22 After pilot testing, we selected 120°/s as a speed that could be comfortably executed in the standing position while remaining more functional than previous hip-abduction-testing methods. These speeds approximate actual hip-abduction/adduction velocities quantified kinematically during high-risk cutting tasks.27
The initial test leg was alternated between subjects to control for a side-learning effect. After each successful test session, the peak torque was recorded for maximum hip abduction from the 5 repetitions. Trials were not accepted if the subject exhibited excessive trunk motion, which may have affected the results. Excessive trunk motion was established in the testing protocol as any motion of the trunk that visually appeared to assist in the development of hip abduction movement. This occurred very infrequently; however, when it did occur, the subject was given approximately 30 to 60 seconds to rest and then was retested. Peak hip-abduction torques were recorded and analyzed by a single investigator. Intra-rater reliability (ICC3,1) for the presented hip-abduction test methods demonstrated good to excellent reliability on the left (ICC = .857; CI .577, .971) and right (ICC = .916; CI .727, .984) sides.28,29
Statistical Analyses
Statistical means and standard deviations for each variable were calculated for each group. All peak torques were normalized to body mass. A mixed-effects regression analysis was used to test the hypothesis regarding the effect of age and gender on normalized hip peak torque. The mixed-effects regression allowed for both a continuous time (age) variable and a dichotomous gender variable. In addition, a key feature of the mixed-effects regression is the appropriate treatment of missing repeated measurements (uneven number of repeated torque measures between subjects).30 Statistical analyses were performed with SAS-PROC MIXED (SAS Institute Inc, Carey, NC).
Results
For both the dominant and nondominant sides, there were significant increases in hip-abduction torque normalized to body mass with increasing age (P < .001) in all subjects. There was also a significant interaction of gender and age (P < .001), indicating that males experienced significantly greater increases in peak torque than females as they aged (Figure 4). Regression equations were generated to estimate normative strength to body weight measures in each age group for both males and females (Table 1). This test demonstrated high reliability on both the left (r = .857) and right (r = .916) sides.
Figure 4.
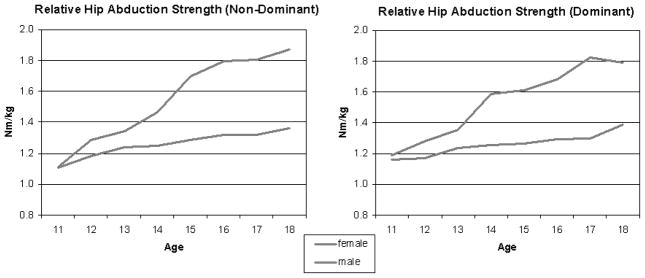
Graphical representation of the relative hip strength of males and females.
Table 1.
Regression-Equation Values for Relative Hip-Abduction Torque (Nm/kg) in Males and Females in Both the Dominant and Nondominant Legs
| Dominant Leg
|
Nondominant Leg
|
||||
|---|---|---|---|---|---|
| Age, y | Males | Females | Age, y | Males | Females |
| 11 | 1.1928 | 1.1481 | 11 | 1.1495 | 1.1379 |
| 12 | 1.2959 | 1.1806 | 12 | 1.2671 | 1.1749 |
| 13 | 1.3990 | 1.2130 | 13 | 1.3847 | 1.2119 |
| 14 | 1.5021 | 1.2455 | 14 | 1.5023 | 1.2489 |
| 15 | 1.6052 | 1.2779 | 15 | 1.6199 | 1.2859 |
| 16 | 1.7083 | 1.3103 | 16 | 1.7375 | 1.3229 |
| 17 | 1.8114 | 1.3428 | 17 | 1.8551 | 1.3599 |
| 18 | 1.9145 | 1.3752 | 18 | 1.9727 | 1.3969 |
Discussion
The purpose of this study was to evaluate the effects of gender and age on hip-abduction strength as assessed in a functional standing position. Recent investigations that have indicated that there may be a potential association of hip-abduction measures to dynamic valgus alignments that increase ACL injury risk and underline the importance of hip-abduction strength.6,8,9,11 Associations of strength deficits to mechanism of ACL injury have typically focused on quadriceps and hamstrings strength, although the association of hip strength to ACL injury risk has not been extensively studied.19 Studies specifically evaluating hip-abduction strength have not reported age differences for adolescents in either healthy or patient populations.16,20–22 However, those studies have historically employed isometric measurements with handheld dynamometers or isokinetic measures in the side-lying position.
The findings of this study support the first hypothesis and demonstrate that females create lower peak hip-abduction torques relative to their body mass than males. Previous studies of strength and power deficits in female athletes also implicated these measures as potential risk factors for ACL injury.23,24,31 Several authors suggested that by improving hip strength and core stability, lower extremity alignment could be improved, such that ACL injury risk would be reduced.9,11,13 The measured deficits in hip strength could potentially contribute to the increased ACL injury risk in female athletes relative to their male counterparts.
The second hypothesis, that males would show increased relative hip-abduction torque with age, while females would not, was partially supported. As males aged, they demonstrated increased isokinetic hip-abduction torque. However, while females did show an increase, it was not of the same magnitude as that of males. The absence of a similar increase in relative hip-abduction torque in females has not previously been reported in the literature, although other measures of lower extremity strength have shown evidence of this lack of neuromuscular spurt with maturation.25
Previous studies reported that females may have certain neuromuscular imbalances in their lower extremities, such as quadriceps dominance, ligament dominance, or side-to-side dominance.3,32,33 This may lead to their inability to prevent their knee joints from collapsing into a dynamic valgus position.4,25,34 Strength and conditioning coaches may prescribe hip-abductor-strengthening exercises to aid in the reduction of this frontal-plane instability of the knee.9,13 This study indicates the need for further exploration of the relationship between hip abductors and their role in controlling the varus–valgus movement of the knee.11 This is especially important when related to the relationship between increased dynamic valgus and ACL injury risk.6
Future research is warranted to investigate the potential relationship between kinematic variables of dynamic lower extremity valgus and isokinetic measures of torque for both hip-abduction musculature and quadriceps and hamstring strength, to determine if strength in the hip and knee region correlates to the ability to control harmful movement in both the sagittal and coronal planes. A longitudinal study, following the subjects as they matured, would help further clarify how the peak torques related to age. In addition, an EMG study could be helpful in comparing strength versus recruitment. In addition, outcome studies that investigate the effectiveness of a training regimen with specialized exercises focused on hip-abduction strength as a means of improving coronal-plane hip strength and, in turn, lower extremity alignment deficits should be conducted. These studies could ultimately demonstrate a decreased risk of lower extremity injury.
The current reported findings have limitations that restrict the interpretation of the results. Although the standing position during hip-abduction-torque assessment is a more functional position than other investigations of hip-abduction strength, it represents an open-chain torque assessment. Often dynamic valgus alignment and ACL injury occur during a closed-chain stance, which may limit the relationship of current measures to valgus alignment and subsequent injury risk.2,3,35,36 With regard to testing velocity, a close approximation was used to mimic the speed quantified during high-risk cutting tasks. Testing at multiple speeds could provide additional, valuable data about the gender difference in hip-abduction torques. In addition, all the athletes assessed in this study were soccer players. Therefore, the generalizability of these results to other populations at high risk for ACL injury, specifically, basketball or volleyball players, may be limited. In addition, ACL injury in female athletes likely has a multifactorial etiology, with several potential elements that determine injury mechanism. In specific, increased knee-abduction motion and torque,6 increased knee-joint laxity,37 and reduced relative hamstring strength26 have a reported relationship to increased ACL injury risk in female athletes. These prior epidemiologic data demonstrate that biomechanical factors may contribute in isolation or combination with other factors, such as anatomical, hormonal, and potentially psychological parameters, to increase relative ACL injury rates in female athletes. Multivariate analysis that incorporates the proposed hip-abduction strength measurement may provide more robust prediction of ACL injury risk.
Conclusions
This longitudinal study demonstrates that hip-abduction strength relative to body mass increases in males as they age. In contrast, hip-abduction strength does not increase with the same magnitude in females across the same age groups. These findings may indicate that strength and conditioning protocols that include hip-abduction strengthening should be implemented for young females beginning at age 12 to 13, when the divergence between females and males occurs. This can be accomplished through a variety of methods including dynamic-balance exercises, as well as resistance-training exercises specifically aimed at strengthening the muscles primarily responsible for hip abduction. While targeted training may not eradicate gender deficits in hip-abduction strength, initial evidence indicates that neuromuscular training results in increased hip-abduction strength, which could be potentially valuable for reducing injuries associated with this deficit.29 Based on the current literature, there are indicators of a link between hip-abduction strength and knee injuries; however, we acknowledge that the determination of hip-abduction strength’s direct relationship to injury risk within the population has yet to be established. As this study did not examine ACL injury rates in this sample or correlate hip-abduction strength to such, future research is needed to determine the direct relationship of hip-abduction strength measures to ACL injury incidence in female athletes. In addition, further investigation is warranted to evaluate different normalization procedures (height, limb length, maturational status) to determine if the current normative hip-abduction values are robust in more generalized populations.
Acknowledgments
The authors would like to acknowledge funding support from National Institutes of Health Grant R01-AR049735-01A1. They would like to thank Boone County School District, Kentucky, especially School Superintendent Dr. Brian Blavatt, for participation in this study.
Contributor Information
Jensen L. Brent, Academy of Sports Performance, Cincinnati, OH
Gregory D. Myer, Sports Medicine Biodynamics Center and Human Performance Laboratory, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH
Kevin R. Ford, Dept of Physical Therapy, High Point University, NC
Mark V. Paterno, Sports Medicine Biodynamics Center and Human Performance Laboratory, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH
Timothy E. Hewett, Sports Medicine Biodynamics Center and Human Performance Laboratory, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH
References
- 1.Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes: a prospective study. Am J Sports Med. 1999;27(6):699–706. doi: 10.1177/03635465990270060301. [DOI] [PubMed] [Google Scholar]
- 2.Ford KR, Myer GD, Toms HE, Hewett TE. Gender differences in the kinematics of unanticipated cutting in young athletes. Med Sci Sports Exerc. 2005;37(1):124–129. doi: 10.1249/00005768-200505001-00628. [DOI] [PubMed] [Google Scholar]
- 3.Ford KR, Myer GD, Hewett TE. Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exerc. 2003;35(10):1745–1750. doi: 10.1249/01.MSS.0000089346.85744.D9. [DOI] [PubMed] [Google Scholar]
- 4.Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes: decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24(6):765–773. doi: 10.1177/036354659602400611. [DOI] [PubMed] [Google Scholar]
- 5.Kernozek TW, Torry MR, Van Hoof H, Cowley H, Tanner S. Gender differences in frontal and sagittal plane biomechanics during drop landings. Med Sci Sports Exerc. 2005;37(6):1003–1012. disc 1013. [PubMed] [Google Scholar]
- 6.Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501. doi: 10.1177/0363546504269591. [DOI] [PubMed] [Google Scholar]
- 7.Brindle TJ, Mattacola C, McCrory J. Electromyographic changes in the gluteus medius during stair ascent and descent in subjects with anterior knee pain. Knee Surg Sports Traumatol Arthrosc. 2003;11(4):244–251. doi: 10.1007/s00167-003-0353-z. [DOI] [PubMed] [Google Scholar]
- 8.Nyland J, Kuzemchek S, Parks M, Caborn DN. Femoral anteversion influences vastus medialis and gluteus medius EMG amplitude: composite hip abductor EMG amplitude ratios during isometric combined hip abduction-external rotation. J Electromyogr Kinesiol. 2004;14(2):255–261. doi: 10.1016/S1050-6411(03)00078-6. [DOI] [PubMed] [Google Scholar]
- 9.Powers CM. The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther. 2003;33(11):639–646. doi: 10.2519/jospt.2003.33.11.639. [DOI] [PubMed] [Google Scholar]
- 10.Neumann DA. Kinesiology of the hip: a focus on muscular actions. J Orthop Sports Phys Ther. 2010;40(2):82–94. doi: 10.2519/jospt.2010.3025. [DOI] [PubMed] [Google Scholar]
- 11.Padua DA, Marshall SW, Beutler AI, et al. Predictors of knee valgus angle during a jump-landing task. Med Sci Sports Exerc. 2005;37(5):S398. doi: 10.1097/00005768-200505001-02048. [DOI] [Google Scholar]
- 12.Click Fenter P, Bellew JW, Pitts TA, Kay RE. Reliability of stabilised commercial dynamometers for measuring hip abduction strength: a pilot study. Br J Sports Med. 2003;37(4):331–334. doi: 10.1136/bjsm.37.4.331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ireland ML, Willson JD, Ballantyne BT, Davis IM. Hip strength in females with and without patellofemoral pain. J Orthop Sports Phys Ther. 2003;33(11):671–676. doi: 10.2519/jospt.2003.33.11.671. [DOI] [PubMed] [Google Scholar]
- 14.Kea J, Kramer J, Forwell L, Birmingham T. Hip abduction-adduction strength and one-leg hop tests: test–retest reliability and relationship to function in elite ice hockey players. J Orthop Sports Phys Ther. 2001;31(8):446–455. doi: 10.2519/jospt.2001.31.8.446. [DOI] [PubMed] [Google Scholar]
- 15.Tyler TF, Nicholas SJ, Hershman EB, Glace BW, Mullaney MJ, McHugh MP. The effect of creatine supplementation on strength recovery after anterior cruciate ligament (ACL) reconstruction: a randomized, placebo-controlled, double-blind trial. Am J Sports Med. 2004;32(2):383–388. doi: 10.1177/0363546503261731. [DOI] [PubMed] [Google Scholar]
- 16.Bertocci GE, Munin MC, Frost KL, Burdett R, Wassinger CA, Fitzgerald SG. Isokinetic performance after total hip replacement. Am J Phys Med Rehabil. 2004;83(1):1–9. doi: 10.1097/01.PHM.0000098047.26314.93. [DOI] [PubMed] [Google Scholar]
- 17.Cahalan TD, Johnson ME, Liu S, Chao EY. Quantitative measurements of hip strength in different age groups. Clin Orthop Relat Res. 1989;(246):136–145. [PubMed] [Google Scholar]
- 18.Knapik JJ, Wright JE, Mawdsley RH, Braun JM. Iso-kinetic, isometric and isotonic strength relationships. Arch Phys Med Rehabil. 1983;64(2):77–80. [PubMed] [Google Scholar]
- 19.Leetun DT, Ireland ML, Willson JD, Ballantyne BT, Davis IM. Core stability measures as risk factors for lower extremity injury in athletes. Med Sci Sports Exerc. 2004;36(6):926–934. doi: 10.1249/01.MSS.0000128145.75199.C3. [DOI] [PubMed] [Google Scholar]
- 20.Johnson ME, Mille ML, Martinez KM, Crombie G, Rogers MW. Age-related changes in hip abductor and adductor joint torques. Arch Phys Med Rehabil. 2004;85(4):593–597. doi: 10.1016/j.apmr.2003.07.022. [DOI] [PubMed] [Google Scholar]
- 21.Masuda K, Kikuhara N, Takahashi H, Yamanaka K. The relationship between muscle cross-sectional area and strength in various isokinetic movements among soccer players. J Sports Sci. 2003;21(10):851–858. doi: 10.1080/0264041031000102042. [DOI] [PubMed] [Google Scholar]
- 22.O’Connor D. Groin injuries in professional rugby league players: a prospective study. J Sports Sci. 2004;22(7):629–636. doi: 10.1080/02640410310001655804. [DOI] [PubMed] [Google Scholar]
- 23.Ahmad CS, Clark AM, Heilmann N, Schoeb JS, Gardner TR, Levine WN. Effect of gender and maturity on quadriceps-to-hamstring strength ratio and anterior cruciate ligament laxity. Am J Sports Med. 2006;34(3):370–374. doi: 10.1177/0363546505280426. [DOI] [PubMed] [Google Scholar]
- 24.Beunen G, Malina RM. Growth and physical performance relative to the timing of the adolescent spurt. Exerc Sport Sci Rev. 1988;16:503–540. doi: 10.1249/00003677-198800160-00018. [DOI] [PubMed] [Google Scholar]
- 25.Hewett TE, Myer GD, Ford KR. Decrease in neuromuscular control about the knee with maturation in female athletes. J Bone Joint Surg Am. 2004;86-A(8):1601–1608. doi: 10.2106/00004623-200408000-00001. [DOI] [PubMed] [Google Scholar]
- 26.Myer GD, Ford KR, Barber Foss KD, Liu C, Nick TG, Hewett TE. The relationship of hamstrings and quadriceps strength to anterior cruciate ligament injury in female athletes. Clin J Sport Med. 2009;19(1):3–8. doi: 10.1097/JSM.0b013e318190bddb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.McLean SG, Huang X, Su A, van den Bogert AJ. Transactions of the Orthopaedic Research Society, Washington DC. Feb 2, 2005. Neuromuscular control contributions to non-contact ACL injury. [Google Scholar]
- 28.Brent JL, Myer GD, Ford KR, Hewett TE. A longitudinal examination of hip abduction strength in adolescent males and females. Med Sci Sports Exerc. 2008;39(5):S290–S291. [Google Scholar]
- 29.Myer GD, Brent JL, Ford KR, Hewett TE. A pilot study to determine the effect of trunk and hip focused neuromuscular training on hip and knee isokinetic strength. Br J Sports Med. 2008;42(7):614–619. doi: 10.1136/bjsm.2007.046086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hedeker D. An introduction to growth modeling. In: Kaplan D, editor. Quantitative Methodology for the Social Sciences. Thousand Oaks, CA: Sage; 2004. pp. 32–49. [Google Scholar]
- 31.Hewett TE, Paterno MV, Myer GD. Strategies for enhancing proprioception and neuromuscular control of the knee. Clin Orthop Relat Res. 2002;402:76–94. doi: 10.1097/00003086-200209000-00008. [DOI] [PubMed] [Google Scholar]
- 32.Sell T, Ferris CM, Abt JP, et al. Predictors of anterior tibia shear force during a vertical stop-jump. J Orthop Sports Phys Ther. 2004;34(1-PL 14):1589–1597. doi: 10.1002/jor.20459. [DOI] [PubMed] [Google Scholar]
- 33.White KK, Lee SS, Cutuk A, Hargens AR, Pedowitz RA. EMG power spectra of intercollegiate athletes and anterior cruciate ligament injury risk in females. Med Sci Sports Exerc. 2003;35(3):371–376. doi: 10.1249/01.MSS.0000053703.65057.31. [DOI] [PubMed] [Google Scholar]
- 34.Hewett TE. Neuromuscular and hormonal factors associated with knee injuries in female athletes: strategies for intervention. Sports Med. 2000;29(5):313–327. doi: 10.2165/00007256-200029050-00003. [DOI] [PubMed] [Google Scholar]
- 35.Boden BP, Dean GS, Feagin JA, Garrett WE. Mechanisms of anterior cruciate ligament injury. Orthopedics. 2000;23(6):573–578. doi: 10.3928/0147-7447-20000601-15. [DOI] [PubMed] [Google Scholar]
- 36.Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004;32(4):1002–1012. doi: 10.1177/0363546503261724. [DOI] [PubMed] [Google Scholar]
- 37.Myer GD, Ford KR, Paterno MV, Nick TG, Hewett TE. The effects of generalized joint laxity on risk of anterior cruciate ligament injury in young female athletes. Am J Sports Med. 2008;36(6):1073–1080. doi: 10.1177/0363546507313572. [DOI] [PMC free article] [PubMed] [Google Scholar]