

Abstract
Introduction: Increasing the knowledge of women on effectiveness of contraceptive methods can lead to the use of more effective methods and reduce unwanted pregnancies and adverse outcomes. We aimed to compare three different approaches for increasing women’s understanding of effectiveness of contraceptive methods. Methods:We ran-domly assigned 630 eligible women of reproductive age to one of the three groups. Each woman received one of three charts presenting pregnancy risk with each contraceptive method. Participants before and while reviewing the chart, answered to three key ques-tions about the effectiveness of the methods. The data were analyzed using chi-square, ANOVA and McNemar's tests in SPSS version 13. Results: The most important reasons for choosing contraceptive methods were their effectiveness (45%), ease of use (18%) and few side effects (14%). At baseline, the participants' knowledge about the effective-ness of the methods was poor. Correct answers were 44% about comparing the effec-tiveness of the combined pills vs. that of condoms, 50% about intrauterine devices vs. injectables, and 52% about condoms vs. withdrawal. While reviewing the charts, the percentages significantly (p < 0.001) increased to 80%, 84% and 85%, respectively. All the three charts almost equally increased the correct responds to the questions.
Conclusion: The three approaches had considerable and nearly identical effects on the promotion of women's knowledge about effectiveness of the contraceptive methods. Therefore, appropriate use of the charts is required during counseling sessions for contraceptive choice because it is impossible to have informed choice of the method without understanding their effectiveness.
Keywords: Effectiveness, Contraceptives, Informed choice, Decision aids
Introduction
A considerable amount of pregnancies in the world had been unplanned1 and over one-third of pregnancies are unwanted.2 Unwanted (unintended) pregnancies are currently one of the health and social problems worldwide.3 And, mostly would lead to poor pregnancy care, anxious mothers and unsafe abortions.4 In Iran, despite availability of primary health and free family planning services for almost all people at public health care centers , high rate of unwanted pregnancies are of major problems.5 About 18.6 percent of pregnancies in Iran and 12.6 percent of them in Tabriz had been unwanted in 2005.6
Therefore, the necessity of promoting the quality of family planning programs is emphasized.7 Unfortunately, the quality of family planning services in Iran is not appropriate and the greatest deficiency is seen in counseling and education areas.8-10 Appropriate counseling and educational interventions can be effective in promoting the understanding and using effective contraceptives.11 In choosing contraceptive methods, the most important factor is its efficacy.12-17 Correct understanding of clients about the effectiveness of methods can lead to informed and proper choices and consequently, lead to choose more effective methods and lower the rate of unwanted pregnancies and adverse outcomes.17-22
A 2008 Cochrane systematic review found only five trials on communicating contraceptive effectiveness.14 According to one study in U.S. and another one in Jamaica and India, it was indicated that at baseline, the awareness level of women was low about effectiveness of the methods and reviewing the charts related to effectiveness significantly increased the percentage of correct answers.12,13 Since no study was found in this field in Iran, we aimed to compare three different approaches for increasing women’s understanding of effectiveness of contraceptive methods.
Materials and Methods
In this randomized controlled trial, we recruited a convenience sample of 630 women at 16 health care centers and 17 health care posts in Tabriz. We used stratified random sampling to select the centers and posts among all (82) centers/posts in the city using random numbers software (www.random.org). The study size of 210 subjects for each group was determined considering 10 percentage point difference in improvement between groups, power = 0.8 and two-sided α = 0.05 and assuming 50% of the participants at baseline will have correct knowledge about the 3 key questions.
The women were at the reproductive age (15-49 years), Tabriz citizens with at least intermediate school education who were not using permanent contraceptive methods. All the data were collected by the corresponding author of the article.
After obtaining written informed consent from the participants, they completed a questionnaire including the following questions: demographic characteristics, history of contraceptive methods, motivational factors for selecting the methods and three key questions about comparing the effectiveness of contraceptive methods. The key questions related to effectiveness of method had been proposed as “which one of the following two contraceptive methods are more effective” (Pills vs. condom, IUD vs. injectables, and condom vs. withdrawal)? Thereafter, the participants were randomly allocated to one of the three charts communicating effectiveness of currently available contraceptive methods in public health centers in Iran. For group assignment, we used permuted-block randomization with random block size of 3 and 6. To conceal the allocation sequence, opaque and sealed envelopes with consecutive numbers were used.
All the three charts show the name and figures of the methods and are drawn based on typical use rate of pregnancy. The first chart (Figure 1, categories and numbers) shows the percentage of pregnancy with each method in the order of their rate of pregnancy during the first year of usage. Also, the methods are divided into four categories as most effective, very effective, effective and the least effective from top to bottom. The second chart (Figure 2, categories) was divided into the four main effectiveness groups with no pregnancy rate for each method. In the chart of continuum (Figure 3), there is an arrow that the bottom and the top of arrow showed the least and the most effective, respectively. Figure 2 and 3 also include some information about correct use of the methods. The figures were in particular color in a way that each category related to the corresponding efficacy had the same color in all figures. The lowest part illustrated the least effective were in red and the upward categories or more effective methods were in brighter colors (in blue).
Figure 1 .

Categories and numbers extracted from Steiner et al12. (With permission)
Figure 2 .

Categories extracted from Steiner et al13(With permission)
Figure 3 .

Continuum extracted from WHO. (With permission)
Three to five minutes after presenting the charts, the second questionnaire containing the same three key questions related to relative effectiveness of the methods plus one question related to ease of understanding as well as another question related to adequacy of information provided by the charts were given to the subjects and they were asked to answer them while reviewing the charts.
Content validity was used to determine the scientific validity of the questionnaire by seven professors and school members of Tabriz University of Medical Sciences. For reliability, test re-test method was used with reliability coefficient of 0.87. The data were analyzed using chi-square, ANOVA and McNemar’s tests by SPSS software.
Ethical permission for study was obtained from the Ethics Committee of Tabriz University of Medical Sciences (No. 6729).
Results
All recruited persons received allocated intervention and were analyzed (Figure 4). There were less than 7% missing response in some characteristics and less than 3% in the key questions (Table 1). There was no significant difference among the three groups in terms of socio-demographic characteristics including age, educational level, employment, marriage age, number of pregnancies, history of abortion, and current number of live children.
Figure 4 .

Flow diagram of trial
Table 1. Background characteristics of the women by the study groups .
| Characteristics | categories and numbers n = 210* | categories n = 210* | Continuum n = 210* | Total n = 630† |
| Age (year) | ||||
| Under 20 | 10 (4.8) | 13.(6.2) | 13 (6.2) | 36 (5.8) |
| 20-29 | 116 (56.1) | 124 (59.1) | 118 (56.5) | 358 (57.1) |
| 30-39 | 67 (32.4) | 61 (29.1) | 71 (34.0) | 199 (31.8) |
| 40-49 | 14 (6.8) | 12 (5.7) | 7.(3.3) | 33 (5.3) |
| Mean (SD) | 28.8 (7.17) | 28.3 (6.7) | 28.1 (6.3) | 28.4 (6.7) |
| Educational level (year) | ||||
| Intermediate or high-school | 65 (32.0) | 69 (33.8) | 80 (38.6) | 214 (34.9) |
| High-school graduate | 102 (50.2) | 104 (51.0) | 100 (48.3) | 306 (49.8) |
| Academic | 36 (17.8) | 31 (15.2) | 27 (13.0) | 94 (15.3) |
| Employment | ||||
| Housekeeper | 180 (86.5) | 187 (89.0) | 189 (90.4) | 556 (88.7) |
| Indoor working | 6 (2.9) | 8 (3.8) | 5 (2.4) | 19 (3.0) |
| Outdoor working | 22 (10.6) | 15 (7.2) | 15 (7.2) | 52 (8.3) |
| Marriage age (years) Under 19 |
94 (45.2) | 94 (45.2) | 100 (49.0) | 285 (46.2) |
| 19-24 | 83 (39.9) | 86 (41.3) | 47 (40.7) | 252 (40.8) |
| 25 and higher | 31 (14.9) | 28 (13.5) | 21 (10.3) | 80 (12.9) |
| Mean (SD) | 20.4 (3.6) | 20.5 (3.9) | 20.5 (3.4) | 20.4 (3.6) |
| History of abortion | ||||
| No | 163 (78.0) | 157 (75.5) | 168 (80.0) | 488 (77.8) |
| Yes | 46 (22.0) | 51 (24.5) | 42 (20.0) | 139 (22.2) |
| Current number of live children | ||||
| 0 | 30 (14.4) | 27 (12.9) | 23 (11.0) | 80 (12.7) |
| 1 | 102 (48.8) | 118 (56.5) | 119 (56.7) | 339 (54.0) |
| 2 | 68 (32.5) | 57 (27.3) | 58 (27.6) | 183 (29.1) |
| 3 and more | 9 (4.3) | 7 (3.3) | 10 (4.8) | 26 (4.1) |
| Mean (SD) | 1.27 (0.77) | 1.22 (0.71) | 1.27 (0.74) | 1.25 (0.74) |
| Importance of not getting regnant | ||||
| Very important | 143 (69.8) | 158 (76.0) | 150 (73.9) | 451 (73.2) |
| Important | 41 (19.5) | 28 (13.5) | 30 (14.8) | 98 (15.9) |
| No important | 15 (7.3) | 16 (7.7) | 11 (5.4) | 42 (6.8) |
| I am not sure | 6 (4.3) | 6 (2.9) | 12 (5.9) | 24 (4.1) |
The data are given as n (%) unless otherwise is specified.
* 1-7 missing response in some characteristics; † 2-16 missing response in some characteristics.
Almost half of the studied women (51%) announced that they had ever consulted with a health care provider about efficacy of contraceptive methods. The most common current method of contraception was condom (31%) and then, pills (17%). In addition, condom was the most frequent ever used contraceptive method (43%). About three fourth of the women (73%) considered importance of not getting pregnant as very important (Table 1). About one fourth of the women had a history of unwanted pregnancy and at the time of unwanted pregnancy, the method of about half of them (46%) were withdrawal, 18% condom, 11% pill and 18% used no method. The women mentioned that the most important reason for choosing one contraceptive method was its effectiveness (45%), ease of use (18%) and its few side effects (14%) (Table 2).
Table 2. The women’s most important reason for choosing the contraceptive method by study groups .
| Reasons | categories and numbers n = 210* | categories n = 210* | continuum n = 210* | Total n = 630† |
| High effectiveness | 94 (48.0) | 89 (44.7) | 103 (51.5) | 286 (48.1) |
| Few side effects | 29 (14.8) | 29 (14.6) | 30 (15.0) | 88 (14.8) |
| Protection against sexually transmitted diseases | 9 (4.6) | 10 (5.0) | 9 (4.5) | 28 (4.7) |
| Ease of use | 41 (20.9) | 36 (18.1) | 36 (18.0) | 113 (19.0) |
| Prolonged effects | 21 (10.7) | 29 (14.6) | 21 (10.5) | 71 (11.9) |
| Others | 2 (1.0) | 6 (3.0) | 1 (0.5) | 9 (1.5) |
The data are given as n (%); * 10-14 missing response; † 35 missing response
At baseline, the knowledge of the participants about the effectiveness of the methods was poor. Only 44% of the subjects knew that the pills are more effective that male condoms, 50% knew IUDs are more effective than injectables and 52% knew condom are more effective than withdrawal. After looking at the charts, the percentage of the correct answers significantly increased to 80%, 84% and 85%, respectively (Table 3). All the three charts significantly promoted the knowledge of the 3 key questions (p < 0.001), with improvement between 30-40 percentage point; however, no chart promoted knowledge significantly than the other charts (p = 0.96, Figure 5).
Table 3. Frequency of the studied women according to the percentage of correct responses to the questions related to comparison of efficacy before and after the intervention separated by study groups .
| Questions | categories and numbers n = 210* | categories n = 210* | continuum n = 210* | Total n = 630† | comparing the 3 groups | |
| Which one is more effective: Pills or Male condoms? | Before After |
93 (45.1) 169 (80.5) |
97 (46.2) 162 (78.3) |
85 (40.9) 169 (81.3) |
275 (44.1) 500 (80.0) |
P = 0.51 p = 0.73 |
| Which one is more effective: IUD or Injectables? | Before After |
95 (46.3) 174 (83.3) |
108 (51.4) 171 (82.2) |
104 (51.0) 180 (86.5) |
307 (49.6) 525 (84.0) |
p = 0.52 p = 0.45 |
| Which one is more effective: Withdrawal or Male condoms? | Before After |
109 (52.7) 185 (88.1) |
100 (47.8) 167 (79.9) |
115 (55.6) 183 (88) |
324 (52.0) 535 (85.3) |
p = 0.28 p = 0.025 |
The data are given as n (%); *1-6 missing response in somequestions† ; 3-11 missing response in some questions.
Figure 5 .
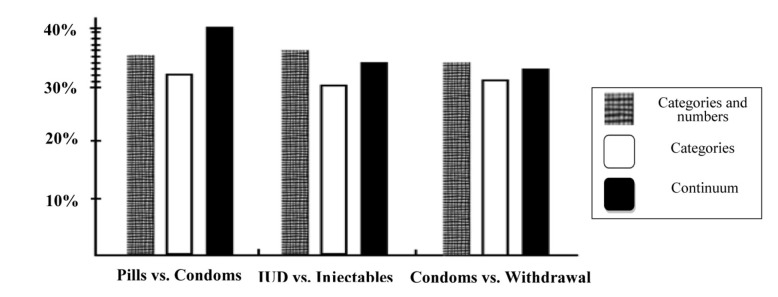
Percentage point improvement in correct knowledge by assigned chart
Majority of the women (93 percent) announced that the assigned charts were easy to understand and provided adequate information to select a contraceptive method. The difference among the study groups in these areas was very small and statistically non-significant.
Discussion
In the present study, the most important reason for choosing a contraceptive method was its efficacy which was in accordance with other studies.12-17 However, at baseline (before looking at the charts), only about half of the participants properly recognized that out of the two current most common contraceptive methods, which one was more effective. This weak baseline knowledge about the relative effectiveness of contraceptive methods almost was in accordance with the study findings done in the U.S. (2003)13 and another study in Jamaica and India in 2006.12
Informed choice for health issues is the absolute right of individuals18 which can be possible only through proper understanding of the current risks. The contraceptive method clients should be appropriately informed of the advantages, side effects and also risks, especially the risk of pregnancy.18
Appropriate information with an understandable and usable way should be transferred to individuals to enable them to make informed choice.23 Studies have shown that in counseling sessions in order to choose the contraceptive method, often much redundancy information is provided while required essential information is not provided for informed choice. Therefore, nowadays using educational aids particularly the visual ones are highly emphasized during the counseling sessions because they are more reliable than memory, will reduce the error possibility by care provider, will decrease the amount of reminding, and will better provide basic information according to the required essential needs for informed choice.25,26
The ultimate objective of this study was to provide the right helpful tools for decision-making of women for an informed choice of contraceptive methods. Three simplified charts of informing the effectiveness of contraceptive methods that had differences in content and appearance were compared and evaluated to each other and it was concluded that all three methods significantly promoted the percentages of correct responses however, there was no significant difference among these three charts in terms of efficacy rate which was in accordance with the results of two other studies.12,13
Proper counseling and education could promote understanding of the use of more effective contraceptive methods11 and reduce the risk of unwanted pregnancy.22 In this study, only about half of the subjects announced that they had ever consulted with a health care provider for effectiveness of contraceptive methods. In the study of Steiner et al. in the U.S.,13 83 percent of women and in their other study in Jamaica and India12, about half of the participated women said they consulted with a health care provider for effectiveness of contraceptive methods.13 Considering that unwanted pregnancy would have many adverse effects on individual and community health, one of the rights of healthy living includes ensuring the efficacy of contraceptive method.24 Nonetheless, counseling on the risk of pregnancy for contraceptive methods using appropriate educational aids, like the charts which their efficacy was shown in this study, is the main task of health staff which should be emphasized.12
The strength points of this study included random allocation of the subjects, allocation concealment, large sample size for detecting a clinical promotion of knowledge and also evaluation of the knowledge before and after the intervention. The limitations of the current study included using available samples from women referred to selected centers. We tried to lessen this limitation through random selection of the health care centers and posts from different geographical regions of Tabriz as well as selection of all eligible clients referred to health care centers for any reason (e.g., diabetes screening and etc.). Subjects in this study were women with educational level of at least intermediate school and its results my not be generalized to individuals with lower education.
Conclusion
Before the intervention, the knowledge level of women on the effectiveness of contraceptive methods was low whereas after the intervention it was significantly increased. All three different charts almost equally improved the knowledge of women; therefore, using such charts during counseling sessions seems necessary for informed choice of contraceptive methods.
Ethical issues
None to be declared.
Conflict of Interest
The authors declare no conflict of interest in this study.
Acknowledgments
This article was based on MSc thesis of the corresponding author. Hereby, thanks go to Research Deputy of Tabriz University of Medical Sciences for their financial support and all the officials of health care centers and posts of Tabriz and also participating women.
References
- 1.World Health Organization. Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality in 2003. 5th ed. Geneva: WHO; 2007. p. 1.
- 2.Guttmacher Institute, World Health Organization. Facts on induced abortion worldwide [Online]. 2007 [cited 2010 Oct 25]; Available from: URL: http://www.who.int/reproductivehealth/publications/unsafe_abortion/abortion_facts/en/index.html
- 3.Hajian K, Asnafi N. Population and family planning. 2nd ed. Babol: Salemi Publication; 2005. (Persian) [Google Scholar]
- 4.UNFPA. Contraception: Reducing risk by offering contraceptive services [Online]. 2010 [cited 2010 Apr 23]; Available from: URL: http://www.unfpa.org/public/cach/offonce/mothers/pid/4382/
- 5.ShojaiiTehrani H, EbadiFardazar F. Population and family planning and fertility health. 3rd ed. Tehran: Samat Publication; 2001. (Persian) [Google Scholar]
- 6.Khosravi A, Najafi F, Rahbar M, Motlag ME, Kabir MJ. Health indicators in the Islamic Republic of Iran. 1st ed. Tehran: Ministry of Health and Medical Education; 2010. p. 36. (Persian) [Google Scholar]
- 7.Abbasi-Shavazi MJ, Hosseini Chavoshi M, Aghajanian A, Delavar B, Mehryar A. Unintended pregnancies in the Islamic Republic of Iran: levels and correlates. Asia-Pacific population journal. 2004;19(1):27–38. [Google Scholar]
- 8.Mohammad-Alizadeh S, Marions L, Vahidi R, Nikniaz A, Johansson A, Wahlstrom R. Quality of family planning services at primary care facilities in an urban area of East Azerbaijan, Iran. Eur J Contracept Reprod Health Care. 2007;12(4):326–34. doi: 10.1080/13625180701475723. [DOI] [PubMed] [Google Scholar]
- 9.Shahidzadeh A, Mir Moeeni ES, Azimian MH, Mani Kashani KH. Quality of family planning services in health centers in Hamadan in 2003. School of Hygiene and Public Health, Hamadan. 2004;2(1):1–10. (Persian) [Google Scholar]
- 10.Simbar M, Ahmadi M, Ahmadi G, Majd HR. Quality assessment of family planning services in urban health centers of Shadid Beheshti Medical Science University, 2004. International Journal of Health Care Quality Assurance. 2006;19(5):430–42. doi: 10.1108/09526860610680076. [DOI] [PubMed] [Google Scholar]
- 11.Nobili MP, Piergrossi S, Brusati V, Moja EA. The effect of patient-centered contraceptive counseling in women who undergo a voluntary termination of pregnancy. Patient Educ Couns. 2007;65(3):361–8. doi: 10.1016/j.pec.2006.09.004. [DOI] [PubMed] [Google Scholar]
- 12.Steiner MJ, Trussell J, Mehta N, Condon S, Subramaniam S, Bourne D. Communicating contraceptive effectiveness: A randomized controlled trial to inform a World Health Organization family planning handbook. Am J Obstet Gynecol. 2006;195(1):85–91. doi: 10.1016/j.ajog.2005.12.053. [DOI] [PubMed] [Google Scholar]
- 13.Steiner MJ, Dalebout S, Condon S, Dominik R, Trussell J. Understanding risk: a randomized controlled trial of communicating contraceptive effectiveness. Obstet. Gynecol. 2003;102(4):709–17. doi: 10.1016/s0029-7844(03)00662-8. [DOI] [PubMed] [Google Scholar]
- 14.Lopez LM, Steiner MJ, Grimes DA, Schulz KF. Strategies for communicating contraceptive effectiveness. Cochrane Database Syst Rev . 2008;(2): CD006964. doi: 10.1002/14651858.CD006964.pub2. [DOI] [PubMed] [Google Scholar]
- 15.Grady WR, Klepinger DH, Nelson-Wally A. Contraceptive characteristics: the perceptions and priorities of men and women. Fam Plann Perspect. 1999;31(4):168–75. [PubMed] [Google Scholar]
- 16.Sadana R, Snow R. Balancing effectiveness, side-effects and work: women's perceptions and experiences with modern contraceptive technology in Cambodia. Soc Sci Med. 1999;49(3):343–58. doi: 10.1016/s0277-9536(98)00444-4. [DOI] [PubMed] [Google Scholar]
- 17.Salem RM. Closing the effectiveness gap [Project]. Baltimore: Johns Hopkins Bloomberg School of Public Health Accsessed. 2007 [cited 2011 Mar 20]; Available from: URL:http://info.k4health.org/inforeports/closingthegap/closingthegap.pdf
- 18.World Health Organization, Division of Family and Reproductive Health. Improving access to quality care in family planning: medical eligibility criteria for initiating and continuing use of contraceptive methods. 2nd ed. Geneva: WHO; 2000.
- 19.Covello VT. Risk Communication: Principles, Tools, and Techniques." Global Health Technical Briefs [Online]. 2009 [cited 2009 Aug 20]; Available from: URL:www.maqweb.org/techbriefs/tb49riskcomn.shtml/
- 20.Woolf SH, Chan EC, Harris R, Sheridan SL, Braddock CH, Kaplan RM. et al. Promoting informed choice: transforming health care to dispense knowledge for decision making. Ann Intern Med. 2005;143(4):293–300. doi: 10.7326/0003-4819-143-4-200508160-00010. [DOI] [PubMed] [Google Scholar]
- 21.Kim YM, Kols A, Mucheke S. Informed choice and decision-making in family planning counseling in Kenya. Int Fam Plann Persp 1998; 24(1): 4-11, 42. [PubMed] [Google Scholar]
- 22.Lowdermilk DL, Perry SE. Maternity and women's health care. 8th ed. Philadelphia: Mosby; 2004. [Google Scholar]
- 23.Rothman AJ, Kiviniemi MT. Treating people with information: an analysis and review of approaches to communicating health risk information. J Natl Cancer Inst Monogr 1999; (25): 44-51. [DOI] [PubMed] [Google Scholar]
- 24.O'Connor AM, Legare F, Stacey D. Risk communication in practice: the contribution of decision aids. BMJ. 2003;327(7417):736–40. doi: 10.1136/bmj.327.7417.736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bruce L, Martin A. Balanced Counseling Strategy: A Toolkit for Family Planning Service Providers. Trainer's Guide. Washington: Population Council; 2008. p. 1 [Google Scholar]
- 26.Ali Mohammad Zadeh KH, Farzadi Z. Population and family planning. 3xxsuprdxysup ed. Tehran: Ferdous Publication; 2002. p. 197, 207, 208. (Persian).