

Abstract
Trigonocephaly is the premature fusion of the metopic suture leading to deformation of anterior calvarium causing keel shaped deformity of forehead. In most cases, surgical correction is for aesthetic and psychosocial reasons. Various techniques have been described. Here we describe a technique, which is simple to perform with good postoperative results. Metopic suture is excised, one side is reconstructed in finger clasping manner to fit in an expanded area, and the other side is transected and simply molded, and all these fixed with nonabsorbable suture. Supraorbital horizontal bar is mobilized on either side anteriorly and fixed with titanium plate and screws.
Keywords: Craniofacial surgery, craniosynostosis, metopic suture, trigonocephaly
Introduction
Trigonocephaly, coined by Welcker 1862, is an entity characterized by premature fusion of metopic suture.[1] It is a rare form of craniosynostosis, reported in 0.3/1000 live births.[2] Frontal bone grows in the transverse direction, perpendicular to the fused metopic sutures leading to arrested development of frontal area with compensatory expansion of other areas resulting in trigonocephaly. It is characterized by keel shaped deformity of forehead with midline ridge, bilateral fronto temporal constriction with compensatory biparietal expansion, supra orbital and lateral orbital retrusion and hypotelorism.[3,4,5,6]
Surgery is performed predominantly for aesthetic and psychosocial considerations. Various techniques have been described for the surgical treatment of trigonocephaly ranging from simple suturectomy to calvarial bone remodeling, minimally invasive procedures to distraction osteogenesis.[2,7,8,9,10,11,12,13,14,15,16,17,18]
We describe a new surgical technique in which in addition to excision of the metopic suture, the remaining frontal cranial free bone flaps are differently fashioned, and the supraorbital bar is advanced on both sides and fixed.
Case Report
A 3-year-old child presented with a complaint of triangular forehead since birth [Figures 1 and 2]. There were no other complaints, like features of raised intracranial pressure or another associated deformity of the craniofacial area. Patient was evaluated and diagnosed as a case of nonsyndromic trigonocephaly, Noncontrast computed tomography head was done with three-dimensional reconstruction to rule out another intracranial pathology as well as to study the bony anatomy of the craniofacial area. Then the patient was taken up for surgery.
Figure 1.
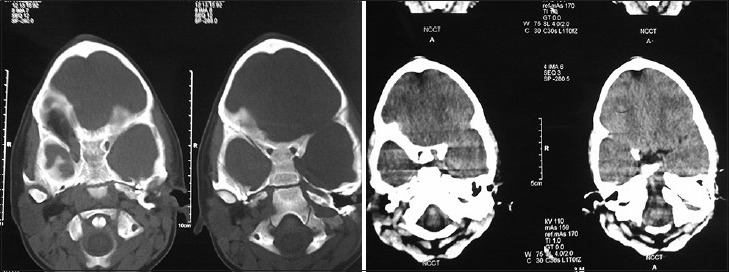
Preoperative noncontrast computed tomography showing small anterior cranial fossa (ACF) and conical shape of ACF with keel shaped ridge
Figure 2.

Photograph showing conical shape fore head with ridge
Surgical Technique
After induction patient is placed supine on a head ring holder in a neutral position with a slight extension. After scrubbing bicoronal skin incision marking done starting from one ear lobule to the other ear lobule and running posterior to the coronal suture in a zig zag fashion and infiltrated with xylocain with adrenalin 0.5%. The incision site was painted with betadine and draping done. The scalp flap was raised until temporal muscles and borders of both orbital rims were visible bilaterally. Periorbita was gently separated from the superior medial and lateral orbital walls. Supraorbital neurovascular bundles released with a fine chisel and then retracted, along with periorbita. Dissection around both orbital rim is done to expose nasofrontal suture medially and both frontozygomatic suture bilaterally. Temporal muscle is dissected and retracted posteriorly to expose the area of pterion and squamous part of the temporal bone. Aggressive use of cautery and dissection is avoided because this will cause temporal muscle atrophy and postoperative temporal hollowing. Bilateral pterional burr hole made, two para saggital burr hole behind the coronal suture and one midline frontal burr hole 2 cm above frontonasal suture is made. With the help of craniotome bone flap is raised. This frontal craniotomy extends behind the coronal suture. Inferior limit of craniotomy is nearly 1.5 cm above the superior orbital rim thus leaving a thick fronto orbital bandeau for remodeling. Frontal bone is separated from dura all around and removed. Superior sagittal sinus is covered with gel foam to prevent air embolism and oozing. Dura is freed from lesser wing of the sphenoid bone laterally and foramen caecum medially. Supraorbital horizontal bar is mobilized on either side anteriorly and fixed with titanium plate and screws.
Frontal reconstruction is made by excising the metopic suture and fashioning the residual two pieces as shown in Figures 3 and 4. On one side it was simply transected and molded and on the other side, it was fashioned in finger clasping shape. The reconstruction in finger clasping manner covers expanded area without significant bony defect. Moreover, space between the parts of the bone will be filled by the growth of bone. Also, there is widening of anterior cranial fossa in the transverse direction. These pieces of calvarium were fixed with nonabsorbable suture as shown in Figures 3 and 4. After hemostasis suturing of bilateral temporalis muscles was done. Scalp flap sutured in layers. Intraoperative total blood loss is 200 ml, 100 ml blood transfusion was given intraoperatively, and patient was discharged after 4 days with good cosmetic result [Figures 5 and 6], improving further over 1 year.
Figure 3.
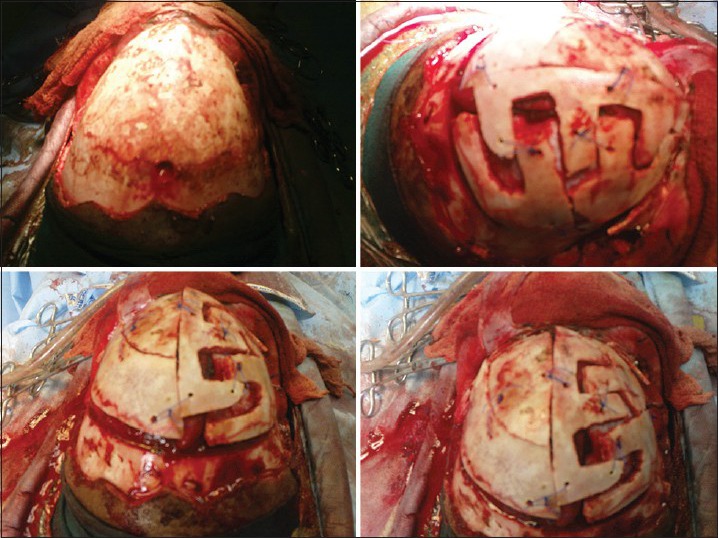
Intraoperative photograph showing the manner in which bone has been cut
Figure 4.
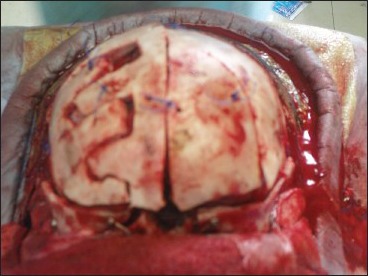
Intraoperative photograph showing the manner in which bone has been cut from frontal side
Figure 5.

Postoperative photograph showing improved contour of fore head
Figure 6.
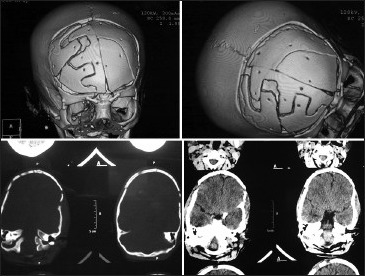
Postoperative noncontrast computed tomography head with three-dimensional reconstruction showing increased volume of anterior cranial fossa as well as improved contour of fore head
Discussion
Trigonocephaly is a post-neurulation defect causing premature fusion of the metopic suture usually occurring before birth.[19,20] Normally it fuses at 1 year of age or may remain patent up to the age of 2 years.[19] Reason for premature fusion of the metopic suture may be one or combination of following-Intrauterine compression; from the subjacent dura mater supplying osteoinductive growth factors and cellular elements to the suture mesenchyme; exposure to high level of thyroxine resulting from maternal, juvenile, or neonatal hyperthyroidism; deficient brain growth; primary abnormality of mesenchyme; rickets; hypercalcemia; and or gene mutation.[21,22,23,24,25,26,27,28]
Trigonocephaly is a rare form of craniosynostosis with an incidence of about 7/2500 live births, and accounts for 7-23% of the largest series. More common in males, accounting for 65-85% cases.[3,29] Spectrum of disease ranges from mild to very severe degree deformity. In severe forms, brain growth is largely restricted between the frontal bones in the coronal plane, with obvious secondary cranial vault deformities.[4,30,31,32] Characteristic keel shaped forehead can be seen, with bifrontal retrusion, bifronto temporal narrowing, and compensatory biparietal expansion. Hypotelorism develops due to restricted forward and lateral expansion of the anterior skull base and changes in the orbital shape and volume, with or without epicanthal folds.[4,17,33]
Various techniques have been described for the correction of deformity at the various stages of operation. Range is from simple suturectomy to calvarial bone remodeling. Distraction osteogenesis which is based on Elizarovs principle is also tested.[2,7,8,9,10,11,12,13,14,15,16,17,18]
Correction of trigonocephaly requires mainly work at two levels one is at the level of frontal bandeau and another is at the level of calvarial part of the frontal bone.[22] Supraorbital bar is usually advanced and fixed with titanium plates and screws. Green stick fractures are made at lateral orbital walls to correct the bitemporal constriction and to normalize contour. In the calvarial part of the frontal bone, multiple fingers like osteotomy done toward its center so that it can expand in the lateral direction to provide space for growing brain, this maneuver creates the round shape of head.[2,34,35] There are multiple ways of doing osteotomy of the frontal bone like zig zag, finger like fashion. We had excised metopic suture, and the residual two halves were refashioned. One-half is cut in a step ladder manner in the anteroposterior direction, and the other half is remodeled in finger clasping shape to fill the gap of the metopic suture, as shown in Figures 3 and 4. As the growth of bone occurs perpendicular to the suture line and in case of metopic suture fusion which lies in the anteroposterior direction the growth will be restricted in the transverse direction and doing surgery in such a manner that is cutting the bone in step ladder pattern with suturectomy of the metopic suture and creating a space between bone fragments, we can give a space for the growth of the bone in the transverse direction and this direction is most physiological for the frontal bone growth. Hence, we believe that this may result in better cosmetic appearance.
Treatment of metopic synostosis is multidisciplinary, plastic and reconstructive surgeon, neurosurgeon, pediatrician and ophthalmologist are necessary. Timing of surgery is controversial. Aim is best long-term cosmetic results and minimal risk. While patients are usually operated at around 1 year of age, patients in few other series were operated at the age of 3-9 months.[30,36,37]
Conclusion
This technique seems to be a simple and cost-effective technique for correction of trigonocephaly with good results. The finger clasping reconstruction provides better molding with expanded coverage. The avoidance of miniplates and screws for the calvarial reconstruction brings down the cost of surgery while allowing for natural molding.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Welcker H. Leipzig: Engelmann; 1862. Untersuchungenüber Wachstum und Bau des Menschlichen Schädels (Investigation over growth and formation of the human skull) [Google Scholar]
- 2.Fearon JA, Kolar JC, Munro IR. Trigonocephaly-associated hypotelorism: Is treatment necessary? Plast Reconstr Surg. 1996;97:503–9. doi: 10.1097/00006534-199603000-00001. [DOI] [PubMed] [Google Scholar]
- 3.Aryan HE, Jandial R, Ozgur BM, Hughes SA, Meltzer HS, Park MS, et al. Surgical correction of metopic synostosis. Childs Nerv Syst. 2005;21:392–8. doi: 10.1007/s00381-004-1108-y. [DOI] [PubMed] [Google Scholar]
- 4.Havlik RJ, Azurin DJ, Bartlett SP, Whitaker LA. Analysis and treatment of severe trigonocephaly. Plast Reconstr Surg. 1999;103:381–90. doi: 10.1097/00006534-199902000-00004. [DOI] [PubMed] [Google Scholar]
- 5.Selber J, Reid RR, Gershman B, Sonnad SS, Sutton LN, Whitaker LA, et al. Evolution of operative techniques for the treatment of single-suture metopic synostosis. Ann Plast Surg. 2007;59:6–13. doi: 10.1097/01.sap.0000264836.54760.32. [DOI] [PubMed] [Google Scholar]
- 6.Warschausky S, Angobaldo J, Kewman D, Buchman S, Muraszko KM, Azengart A. Early development of infants with untreated metopic craniosynostosis. Plast Reconstr Surg. 2005;115:1518–23. doi: 10.1097/01.prs.0000160270.27558.64. [DOI] [PubMed] [Google Scholar]
- 7.Albin RE, Hendee RW, Jr, O’Donnell RS, Majure JA. Trigonocephaly: Refinements in reconstruction. Experience with 33 patients. Plast Reconstr Surg. 1985;76:202–11. [PubMed] [Google Scholar]
- 8.Barone CM, Jimenez DF. Endoscopic approach to coronal craniosynostosis. Clin Plast Surg. 2004;31:415–22. doi: 10.1016/j.cps.2004.03.005. [DOI] [PubMed] [Google Scholar]
- 9.Delashaw JB, Persing JA, Park TS, Jane JA. Surgical approaches for the correction of metopic synostosis. Neurosurgery. 1986;19:228–34. doi: 10.1227/00006123-198608000-00008. [DOI] [PubMed] [Google Scholar]
- 10.Jimenez DF, Barone CM. Endoscopic craniectomy for early surgical correction of sagittal craniosynostosis. J Neurosurg. 1998;88:77–81. doi: 10.3171/jns.1998.88.1.0077. [DOI] [PubMed] [Google Scholar]
- 11.Jimenez DF, Barone CM, McGee ME, Cartwright CC, Baker CL. Endoscopy-assisted wide-vertex craniectomy, barrel stave osteotomies, and postoperative helmet molding therapy in the management of sagittal suture craniosynostosis. J Neurosurg. 2004;100:407–17. doi: 10.3171/ped.2004.100.5.0407. [DOI] [PubMed] [Google Scholar]
- 12.Kovács AF, Sauer SN, Stefenelli U, Klein C. Growth of the orbit after frontoorbital advancement using nonrigid suture vs rigid plate fixation technique. J Pediatr Surg. 2008;43:2075–81. doi: 10.1016/j.jpedsurg.2008.03.057. [DOI] [PubMed] [Google Scholar]
- 13.Marchac D. Radical forehead remodeling for craniostenosis. Plast Reconstr Surg. 1978;61:823–35. [PubMed] [Google Scholar]
- 14.Marsh JL, Schwartz HG. The surgical correction of coronal and metopic craniosynostoses. J Neurosurg. 1983;59:245–51. doi: 10.3171/jns.1983.59.2.0245. [DOI] [PubMed] [Google Scholar]
- 15.Matson DD. Surgical treatment of congenital anomalies of the coronal and metopic sutures. Technical note. J Neurosurg. 1960;17:413–5. [Google Scholar]
- 16.Murad GJ, Clayman M, Seagle MB, White S, Perkins LA, Pincus DW. Endoscopic-assisted repair of craniosynostosis. Neurosurg Focus. 2005;19:E6. doi: 10.3171/foc.2005.19.6.7. [DOI] [PubMed] [Google Scholar]
- 17.Sadove AM, Kalsbeck JE, Eppley BL, Javed T. Modifications in the surgical correction of trigonocephaly. Plast Reconstr Surg. 1990;85:853–8. doi: 10.1097/00006534-199006000-00003. [DOI] [PubMed] [Google Scholar]
- 18.Yano H, Tanaka K, Sueyoshi O, Takahashi K, Hirata R, Hirano A. Cranial vault distraction: Its illusionary effect and limitation. Plast Reconstr Surg. 2006;117:193–200. doi: 10.1097/01.prs.0000194903.45939.b8. [DOI] [PubMed] [Google Scholar]
- 19.Hayward R, Jones B, Evans R. Functional outcome after surgery for trigonocephaly. Plast Reconstr Surg. 1999;104:582–3. doi: 10.1097/00006534-199908000-00054. [DOI] [PubMed] [Google Scholar]
- 20.Dhandapani S, Mehta VS, Sharma BS. “Horseshoe cord terminus” sans filum around a bone spur: A rare composite of faulty gastrulation with agenesis of secondary neurulation: Case report. J Neurosurg Pediatr. 2013;12:411–3. doi: 10.3171/2013.7.PEDS13221. [DOI] [PubMed] [Google Scholar]
- 21.Cohen MM Jr, MacLean RE, editors. 2nd ed. New York: Oxford University Press; 2000. Craniosynostosis: Diagnosis, Evaluation, and Management. [Google Scholar]
- 22.Drake DB, Persing JA, Berman DE, Ogle RC. Calvarial deformity regeneration following subtotal craniectomy for craniosynostosis: A case report and theoretical implications. J Craniofac Surg. 1993;4:85–9. [PubMed] [Google Scholar]
- 23.Hirano A, Akita S, Fujii T. Craniofacial deformities associated with juvenile hyperthyroidism. Cleft Palate Craniofac J. 1995;32:328–33. doi: 10.1597/1545-1569_1995_032_0328_cdawjh_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 24.Leonard CO, Ralston C, Carey JC, Morales L. Craniosynostosis and facial dysmorphism due to maternal Graves disease. Clin Res. 1987;35:225A. Abstract. [Google Scholar]
- 25.Manzanares MC, Goret-Nicaise M, Dhem A. Metopic sutural closure in the human skull. J Anat. 1988;161:203–15. [PMC free article] [PubMed] [Google Scholar]
- 26.Shuper A, Merlob P, Grunebaum M, Reisner SH. The incidence of isolated craniosynostosis in the newborn infant. Am J Dis Child. 1985;139:85–6. doi: 10.1001/archpedi.1985.02140030091038. [DOI] [PubMed] [Google Scholar]
- 27.van der Meulen JJ, Nazir PR, Mathijssen IM, van Adrichem LN, Ongkosuwito E, Stolk-Liefferink SA, et al. Bitemporal depressions after cranioplasty for trigonocephaly: A long-term evaluation of (supra) orbital growth in 92 patients. J Craniofac Surg. 2008;19:72–9. doi: 10.1097/scs.0b013e31815c8a68. [DOI] [PubMed] [Google Scholar]
- 28.Zakarija M, McKenzie JM, Hoffman WH. Prediction and therapy of intrauterine and late-onset neonatal hyperthyroidism. J Clin Endocrinol Metab. 1986;62:368–71. doi: 10.1210/jcem-62-2-368. [DOI] [PubMed] [Google Scholar]
- 29.Lajeunie E, Le Merrer M, Arnaud E, Marchac D, Renier D. Trigonocephaly: Isolated, associated and syndromic forms. Genetic study in a series of 278 patients. Arch Pediatr. 1998;5:873–9. doi: 10.1016/s0929-693x(98)80130-9. [DOI] [PubMed] [Google Scholar]
- 30.Collmann H, Sörensen N, Krauss J. Consensus: Trigonocephaly. Childs Nerv Syst. 1996;12:664–8. doi: 10.1007/BF00366148. [DOI] [PubMed] [Google Scholar]
- 31.Hinojosa J, Esparza J, Muñoz MJ, Salván R, Romance A, Alén JF, et al. Surgical treatment of trigonocephalies and associated hypoteleorbitism. Neurocirugia (Astur) 2002;13:437–45. doi: 10.1016/s1130-1473(02)70568-x. [DOI] [PubMed] [Google Scholar]
- 32.Shimoji T, Shimabukuro S, Sugama S, Ochiai Y. Mild trigonocephaly with clinical symptoms: Analysis of surgical results in 65 patients. Childs Nerv Syst. 2002;18:215–24. doi: 10.1007/s00381-002-0568-1. [DOI] [PubMed] [Google Scholar]
- 33.Eppley BL, Sadove AM. Surgical correction of metopic suture synostosis. Clin Plast Surg. 1994;21:555–62. [PubMed] [Google Scholar]
- 34.Oh DY, Byeon JH. Right angled Z-osteotomy in total cranial vault remodeling in sagittal synostosis. J Korean Soc Plast Reconstr Surg. 2002;29:348–51. [Google Scholar]
- 35.Smartt JM, Jr, Karmacharya J, Gannon FH, Ong G, Jackson O, Bartlett SP, et al. Repair of the immature and mature craniofacial skeleton with a carbonated calcium phosphate cement: Assessment of biocompatibility, osteoconductivity, and remodeling capacity. Plast Reconstr Surg. 2005;115:1642–50. doi: 10.1097/01.prs.0000161466.74294.1e. [DOI] [PubMed] [Google Scholar]
- 36.Di Rocco C, Velardi F, Ferrario A, Marchese E. Metopic synostosis: in favour of a “simplified” surgical treatment. Childs Nerv Syst. 1996;12:654–63. doi: 10.1007/BF00366147. [DOI] [PubMed] [Google Scholar]
- 37.Ferreira MP, Collares MV, Ferreira NP, Kraemer JL, Pereira Filho Ade A, Pereira Filho Gde A. Early surgical treatment of nonsyndromic craniosynostosis. Surg Neurol. 2006;65(Suppl 1):S1:22–1:26. doi: 10.1016/j.surneu.2005.11.038. [DOI] [PubMed] [Google Scholar]