

Abstract
The escalating use of khat (Catha edulis) in East Africa and Arabia is a major concern for public health. Yet little is known about the impact of khat on behaviour. To that end, there has been no study in the region to assess the extent to which dependence syndrome is associated with khat use in this population. We examined in this study was psychometric properties of the Severity of Dependence Scale-Khat (SDS-khat), gender differences in patterns of khat use and dependence, and the extent to which age moderated the link between gender and khat dependence. Two-hundred and ninety-two khat chewers recruited in two Yemeni cities completed face-to-face interviews asking about demographics and patterns of khat use. Validity of SDS-khat was examined by the principle component analysis and reliability of the scale was tested by the Cronbach's alpha. A series of chi-square tests and analysis of variances (ANOVAs) were conducted to examine gender differences in khat use variables. The results indicated that the mean age of khat chewers was 30.52 years (95% CI: 29.34, 31.70) years, and 52% of them were males. The SDS-khat was found to have two factors with moderate reliability. This pattern was consistent when the analysis was conducted in the entire sample and in each gender. Male khat chewers reported more symptoms related to khat dependence than female chewers. A significant gender by age interaction in SDS-khat levels (p =0.013) revealed a positive association between age and khat dependence in women only. These results provide initial support for the use of SDS-khat in the assessment of khat dependence in Yemen. Gender differences in khat use patterns and dependence observed in this study call the need for more studies carefully examining the role of gender in khat research.
Keywords: khat dependence, SDS-khat, psychometric properties, Yemen, gender
1. Introduction
Khat chewing is widely prevailed in countries of East Africa and Middle East, and is growing rapidly. The distribution of khat also is growing; it has expanded to other parts of African countries such as Rwanda, Uganda and Burundi in Africa (Numan, 2012) as well as countries and immigrant communities in Europe and Northern America (Kelly, 2011).
In Yemen, khat chewing is a habit that is integrated into social and daily living, including work, marriage ceremonies (Cox and Rampes, 2003), and social interaction (Cox and Rampes, 2003; Kassim et al., 2010). Reported motivators for using khat includes enhancing alertness during studying in students (Zein, 1988) and relief of physical and mental stress among women (Nabuzoka and Badhadhe, 2000; Wedegaertner et al., 2010). On the other hand, public health impacts of khat chewing (Cox and Rampes, 2003; Al-Motarreb et al., 2010; El-Wajeh and Thornhill, 2009) including khat dependence (Kassim et al., 2013; Kassim et al., 2010) have been reported (al'Absi and Grabowski, 2012). Cathinone, a chemical whose structure is similar to amphetamine (Kalix, 1992), and other indigents such as cathedulins and other alkaloids (Hougton et al., 2012) have been suggested to be responsible for addictive properties of khat. Khat dependence has been tested in immigrant communities of Yemen and Somalia (Kassim et al., 2010; Griffiths et al., 1997) using the Severity of Dependence Scale (Gossop et al., 1995), and these studies found physical and psychological symptoms related to dependence. Surprisingly, however, no systematic attempt has been made to address this question in countries where khat is cultivated, legal, and socially accepted. This was one of the main goals of this study in Yemen.
We also examined gender difference in khat dependence in light of a few studies showing its role in patterns of khat use. Men tend to chew khat more often and intense than women (Nakajima et al., 2013). Women are more likely to start chewing later in their life (Ali et al., 2004; Bongard et al., 2011) to be introduced to khat chewing by their partners when married (Griffiths, 1998). Findings of these studies suggest that men and women have different trajectory of dependence to khat. However, this has never been directly tested among khat chewers in Yemen.
The purpose of this study was to assess khat dependence among adult khat chewers in Yemen. A modified version of SDS (Gossop et al., 1995) which was focused on measuring khat dependence was used (SDS-khat: Kassim et al., 2010). As this questionnaire has not been examined in Yemen, we examined psychometric properties of the scale. Another aim of this study was to examine gender differences in patterns of khat dependence. Finally, we examined the role of age in the link between gender differences and khat dependence. Based on previous research, we hypothesized that (a) SDS-khat would have one dimension; (b) male and female chewers would differ in aspects of khat chewing (e.g. SDS-khat levels); and (c) age would be positively linked with SDS-khat in women but not in men.
2. Materials and Methods
2.1 Subjects and Study design
A total of 401 participants were recruited in two Yemeni cities, Taiz and Sana'a, to this cross sectional study. Participant recruitment was completed in markets and shopping centers around the two cities. Eligibility criteria were: aged 18 years and above and Yemeni, chewing khat at least once a week over the last 12 months, able to speak Arabic or English, and free from any major medical and psychiatric conditions.
This study was approved by the Institutional Review Board in Taiz and Sana'a Universities, Yemen. Potential participants were informed about the volunteer nature of the study and is free to withdraw at any point from the study without consequences. Furthermore, participants were assured that their responses would be kept strictly confidential. Informed written consent was obtained from all participants prior to the interviews. The interviews that took place between September and November 2012 were conducted by trained, culturally competent interviewers. Data was collected via face-to-face interviews that lasted 30 to 45 minutes.
2.2 Measures
The Severity of Dependence Scale (Gossop et al., 1995) is a widely used scale which was developed to assess psychological dependence in illicit drug users (Ferri et al., 2000; Gossop et al., 1995; Swift et al., 1998; Bastiani et al., 2013; Tsai et al., 2012). The SDS consists of five items with each response measured on a Likert-like scale between 0-3, giving a total score out of 15. It focuses on the impaired loss of control over drug use, and preoccupation and anxiety about drug use (Gossop et al., 1995). While the scale has been found to have one underlying dimension (Lawrinson et al., 2007; Kaye and Darke, 2002; Topp and Mattick, 1997; Gossop et al., 1995), this has been questioned particularly when the scale was used in community samples (Swift et al., 1998; Ferri et al., 2000; Tsai et al., 2012). The predictive validity was demonstrated in relation to the need for treatment amongst drug users (Gossop et al., 1995). The bilingual (Arabic and English) version of the Severity of khat dependence (SDS-khat) (Kassim et al., 2010) was used in this study. In addition, questionnaires on demographic (age, gender and marital status), socio-economic status (level of education completed), employment status (employed or unemployed), khat chewing behaviours (number of hours' chewing per khat session, number of days of chewing per week, and types of khat chewed) were collected.
2.3 Data analysis
Data was entered into Excel and managed in the Statistical Package for the Social Sciences (Version 20.0 IBM SPSS Inc. Chicago, IL, USA). Descriptive statistics was conducted to check for data adherence to assumptions of the relevant tests as well as to report sample characteristics. Psychometric properties (construct reliability and validity) of the SDS-khat were evaluated using Cronbach's alpha coefficient, the Kaiser-Meyer-Olkin (KMO) Test for the adequacy of samples to undergo explanatory factor analysis (EFA) (Kaiser, 1974), and the principle component analysis with varimax rotation to identify potential factor(s). We set the loading criterion for the factor(s) at ≥0.50 to facilitate interpretation of the results of EFA (Norman and Streiner, 2003). These analyses were conducted using the entire sample and in each gender. Chi-squared tests were used to examine gender differences in demographic, socioeconomic and behavioural characteristics, and responses to SDS-khat items. To ease the interpretations, the responses for SDS-khat items were collapsed into ‘Not at all’ and ‘Sometimes/Often/Always’. Gender differences in continuous variables (e.g. number of hours of chewing) were tested using parametric unpaired T-tests. The statistical significance test (p-values) was two tailed and set at p<0.05. To examine the moderating role of gender and age on khat dependence, we first classified age into three groups (Group 1: 18-29 years; Group 2: 30-44 years; Group 3: 45 years and above). This categorization was based on the observation that women start khat chewing in their early twenties while men start chewing in their teens (Ali et al., 2004). Then a 2 gender (women, men) × 3 age group analysis of variance (ANOVA) was conducted to test main and interactive effects of gender and age on SDS-khat levels. If a gender by age interaction was statistically significant, a follow-up analysis with Bonferroni correction was conducted. That is, one-way ANOVAs using age category as an independent variable was conducted in SDS-khat in each gender.
3. Results
3.1 Demographic, socio-economic and behavioural characteristics
A total of 401 individuals complete the study. Two-hundred and ninety-two identified themselves as khat chewers but 22 of them did not complete the SDS-khat. These individuals were excluded from the analysis, which lead the final sample of 270 khat chewers (male=141, female=129). The mean age was 30.52 years (95% CI: 29.34, 31.70) with a range of 18-65 years. The majority (57%) of them were married and 66% were daily chewers (see Table 1). On visualization, the distribution of the SDS-khat scores approximated normality (mean 5.17 (95% CI: 4.80, 5.53); median=mode=5.00 (range 0-15)). Twenty-one percent of chewers said that they do not have specific preference for type of khat they chew while 37% mentioned that they chew Mawia khat. Men reported higher scores on SDS-khat (p= 0.0005), more days of khat chewing per week (p=0.001), and longer hours of chewing per day session (p=0.001) than women.
Table 1. Demographic, socio-economic and behavioural characteristics of the whole sample (n=270) and Chi squared test results of observed differences between male (n= 141) and female (n= 129) khat chewers.
| Explanatory variable | Whole sample N (%) or mean±SDa | Males N (%) or mean±SD | Females N (%) or mean±SD | p-value | |
|---|---|---|---|---|---|
|
|
|||||
| Demographic & socio-economic characteristics | Age | ||||
| Mean/SD | 30.52±9.84 | 29.60±9.10 | 31.51±10.55 | 0.133 | |
|
| |||||
| Marital status | |||||
| Married | 155 (57.4) | 75 (53.2) | 80 (62.0) | ||
| Other status | 115 (42.6) | 66 (46.8) | 49 (38.0) | 0.143 | |
|
| |||||
| Education | |||||
| High | 113 (41.9) | 74 (52.5) | 39 (30.2) | ||
| Intermediate | 87 (32.2) | 52 (36.9) | 35 (27.1) | ||
| Basic | 70 (25.9) | 15 (10.6) | 55 (42.6) | 0.0005 | |
|
| |||||
| Employment status | |||||
| Employed | 113 (41.9) | 81 (57.4) | 32 (24.8) | ||
| Unemployed | 157 (58.1) | 60 (42.6) | 97 (75.2) | 0.0005 | |
|
| |||||
| Khat chewing & tobacco smoking behaviours | Number of days chewing | ||||
| Mean/SD | 5.69±2.02 | 6.06±1.80 | 5.28±2.16 | 0.001 | |
|
| |||||
| Number of hours chewing | |||||
| Mean/SD | 5.17±2.27 | 5.82 ±2.14 | 4.45±2.19 | 0.001 | |
|
| |||||
| Type of khat chewed | |||||
| Specific | 213 (78.9) | 121 (85.8) | 92 (71.3) | ||
| Non specific | 57 (21.1) | 20 (14.2%) | 37 (28.7) | 0.004 | |
|
| |||||
| SDS-khat | |||||
| Mean/SD | 5.17±3.06 | 5.94±3.07 | 4.32±2.84 | 0.0005 | |
|
| |||||
| Cessation mood changesb | |||||
| No | 135 (50.0) | 55 (39.0) | 80 (62.0) | ||
| Yes | 135 (50.0) | 86 (61.0) | 49 (38.0) | 0.0005 | |
|
| |||||
| Ever smoking tobacco | |||||
| No | 128 (47.4) | 46 (32.6) | 96 (74.4) | ||
| Yes | 142 (52.6) | 95 (67.4) | 33 (25.6) | 0.0005 | |
|
| |||||
| Current tobacco smoking status | |||||
| Smokersc | 140 (51.9) | 76 (53.9) | 64(49.6) | ||
| Non smokers | 130 (48.1) | 65 (46.1) | 65(50.4) | 0.481 | |
SD, Standard deviation;
khat chewing cessation mood changes;
Smokers with or without khat chewing
3.2 Responses for SDS-khat items
Items 1 and 2 of the SDS-khat were more likely to be anchored to the denial (Not at all) when analysis was conducted in the entire sample and in women only (see Table 2). In contrast, items 3-5 tended to be anchored to the acceptance (Sometimes/Often/Always) when analysed using the entire sample and men only. Fifty-seven percent to 80% of men responded positively (‘Sometimes/Often/Always’ versus ‘Not at all’) to all SDS-khat items while 33 to 65% of women responded positively to the items.
Table 2. Responses of whole sample and both males (n= 141) and females (n= 129) for SDS-khat items.
| SDS-khat items | Not at all (N%) | Sometimes (N%) | Often (N%) | Always (N%) | |
|---|---|---|---|---|---|
| 1. Did you ever think that your khat chewing (altakzeen)a was out of control? | Whole sample | 141 (52.2) | 81 (30.0) | 26 (9.6) | 22 (8.1) |
| Male | 60 (42.6) | 49 (34.8) | 16 (11.3) | 16 (11.3) | |
| Female | 81 (62.8) | 32 (24.8) | 10 (7.8) | 6 (4.7) | |
| 2. Did the prospect of not chewing (takzeen)a any khat make you anxious or worried? | Whole sample | 123 (45.6) | 67 (24.8) | 46 (17.0) | 34 (12.6) |
| Male | 56 (39.7) | 42(29.8) | 24 (17.0) | 19 (13.5) | |
| Female | 67 (51.9) | 25 (19.4) | 22 (17.1) | 15 (11.6) | |
| 3. Did you worry about your khat chewing (altakzeen)? | Whole sample | 106 (39.3) | 113 (41.9) | 36 (13.3) | 15 (5.6) |
| Male | 42 (29.8) | 64 (45.4) | 23 (16.3) | 12 (8.5) | |
| Female | 64 (49.6) | 49 (38.0) | 13 (10.1) | 3 (2.3) | |
| 4. Did you wish you could stop chewing khat (altakzeen)? | Whole sample | 82 (30.4) | 70 (25.9) | 41(15.2) | 77 (28.5) |
| Male | 27 (19.1) | 39 (27.7) | 26 (18.4) | 49 (34.8) | |
| Female | 55 (42.6) | 31 (24.0) | 15 (11.6) | 28 (21.7) | |
| 5. How difficult would you find it to stop or go without khat chewing (altakzeen) for the whole week? | Not difficult | Quite difficult | Very difficult | Impossible | |
| Whole sample | 74 (27.4) | 106 (39.3) | 54 (20.0) | 36 (13.3) | |
| Male | 29 (20.6) | 61 (43.3) | 36 (25.5) | 15 (10.6) | |
| Female | 45 (34.9) | 45 (34.9) | 18 (14.0) | 21 (16.3) |
Note: The values in italic face are responses for the whole sample; in bold face responses for male khat chewers; in normal face responses for female khat chewers;
altakzeen and takzeen=process of chewing and storing khat leaves in the buccal bouch among Yemeni chewers
A series of chi-square tests further found that, in each item, gender was associated with response patterns (p<0.05; see Table 3). For example, 81% of male chewers and 57% of female chewers reported that they wish to stop khat chewing (p=0.0001), and 79% of men versus 65% of women mentioned difficulty in going without chewing for the whole week (p=0.008).
Table 3. Comparisons of responses of males (n= 141) and females (n= 129) for SDS-khat items.
| SDS-khat items | Gender | Noa (%) | Yesb (%) | p-value |
|---|---|---|---|---|
|
| ||||
| 1. Did you ever think that your khat chewing (altakzeen)c was out of control? | Male | 60 (42.6) | 81 (57.4) | |
| Female | 81 (62.8) | 48 (37.2) | 0.001 | |
|
| ||||
| 2. Did the prospect of not chewing (takzeen)c any khat make you anxious or worried? | Male | 56 (39.7) | 85 (60.3) | |
| Female | 67 (51.9) | 62 (48.1) | 0.044 | |
|
| ||||
| 3. Did you worry about your khat chewing (altakzeen)? | Male | 42 (29.8) | 99 (70.2) | |
| Female | 64 (49.6) | 65 (50.4) | 0.001 | |
|
| ||||
| 4. Did you wish you could stop chewing khat (altakzeen)? | Male | 27 (19.1) | 114 (80.9) | |
| Female | 55 (42.6) | 74 (57.4) | 0.0001 | |
|
| ||||
| 5. How difficult would you find it to stop or go without khat chewing (altakzeen) for the whole week? | Not difficult | Difficultd | ||
|
| ||||
| Male | 29 (20.6) | 112 (79.4) | ||
| Female | 45 (34.9) | 84 (65.1) | 0.008 | |
Note:
No=Not at all;
Yes=Sometimes/Often/Always;
altakzeen and takzeen =process of chewing and storing khat leaves in the buccal bouch among Yemeni chewers;
Difficult=Difficult/Very difficult/Impossible
3.3 Psychometric properties of SDS-khat
The factor analyses conducted in the whole sample and in each gender (men, women) revealed that the KMO Tests were 0.7, 0.6 and 0.7, respectively. Bartlett's Test of Sphericity was significant in all three tests (p≤0.00005). The correlational analysis indicated many coefficients at 0.30 and above. Items 3 and 4 correlated poorly with other items, although they correlated with each other in the whole sample and per gender. The eigenvalues of the components exceeding 1, and Catell's Scree test (Cattell, 1966)-plotting each of the factors against its associated eigenvalue - demonstrated two domains for the SDS-khat, which included ‘potential for dependence’ (item 1, item 2, item 5) and ‘desire to stop’ (item 3 and item 4). This pattern was found using the entire sample as well as in each gender. Reliability of the scale was 0.60 in the whole sample, 0.54 in men, and 0.57 in women (see Table 4).
Table 4. Psychometric characteristics for the SDS-khat for the whole sample and separated per gender.
| SDS-khat items | Whole sample | Males sample | Females sample | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Corrected item-total correlation |
Cronbach's Alpha if item deleted |
Factors loadings | Corrected item-total correlation |
Cronbach's Alpha if item deleted |
Factors loadings | Corrected item-total correlation |
Cronbach's Alpha if item deleted |
Factors loadings | ||||
| Factor 1 | Factor 2 | Factor 1 | Factor 2 | Factor 1 | Factor 2 | |||||||
| Item 1 | 0.47 | 0.50 | 0.69 | 0.43 | 0.40 | 0.74 | 0.45 | 0.44 | 0.61 | |||
| Item 2 | 0.40 | 0.52 | 0.82 | 0.45 | 0.39 | 0.81 | 0.32 | 0.52 | 0.84 | |||
| Item 3 | 0.26 | 0.59 | 0.73 | 0.23 | 0.53 | 0.77 | 0.20 | 0.58 | 0.74 | |||
| Item 4 | 0.25 | 0.59 | 0.79 | 0.12 | 0.58 | 0.75 | 0.26 | 0.55 | 0.70 | |||
| Item 5 | 0.39 | 0.52 | 0.75 | 0.30 | 0.49 | 0.73 | 0.42 | 0.46 | 0.74 | |||
| Cronbach's alpha | 0.60 | 0.54 | 0.57 | |||||||||
| Variance explained (%) | 38.96% | 20.84% | 36.69% | 22.98% | 37.77% | 20.43% | ||||||
Item 1: Did you ever think that your khat chewing (altakzeen) was out of control?. Item 2: Did the prospect of not chewing (takzeen) any khat make you anxious or worried? Item 3: Did you worry about your khat chewing (altakzeen)? Item 4: Did you wish you could stop chewing khat (altakzeen)? Item 5: How difficult would you find it to stop or go without khat chewing (altakzeen)?
3.4 Impact of age and gender on levels of SDS-khat
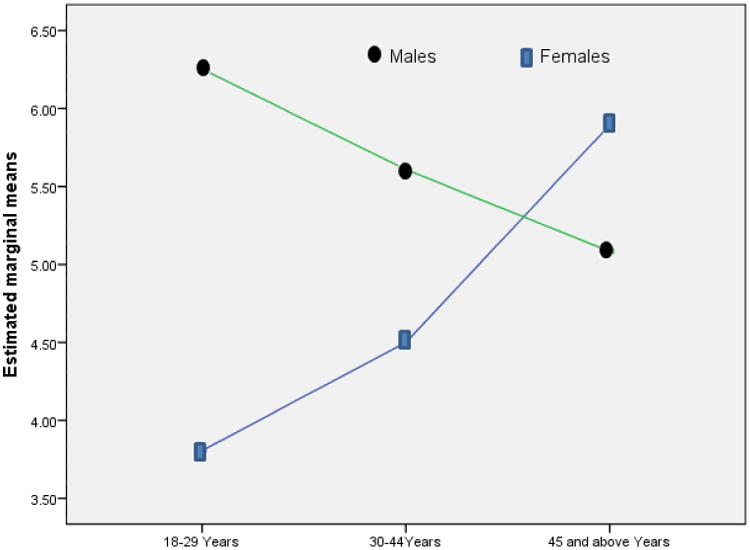
A two-way ANOVA conducted on SDS-khat found a significant main effect of gender [F (2,264)=4.19, p=0.042], which was further qualified by a significant group by age category interaction [F (2,264)=4.39, p=0.013; see Figure 1]. Post-hoc analysis conducted in each gender found a significant main effect of age category on SDS-khat (P=0.012), indicating higher levels of khat dependence in the group of 45 years and above relative to the group 18-29 years old in women. This was not found in men.
Figure 1. Estimated marginal means of SDS-khat for age and gender interaction.
4. Discussion
To our best knowledge, this is the first study to assess khat dependence in male and female khat chewers. Male and female chewers had different patterns of khat use as well as symptoms related to dependence. The SDS-khat was found to have two dimensions in this sample, and this pattern was consistently observed when the test was conducted in each gender. The interaction of gender and age category found in SDS-khat levels supported the moderating influence of age in the association of gender with SDS-khat levels, particularly for female chewers.
The rate of daily khat use in the current sample was higher than that in immigrants from Somalia and Yemen living in the UK (Griffiths et al., 1997; Patel et al., 2005; Kassim et al., 2010; Nabuzoka and Badhadhe, 2000), and a considerable number of chewers reported chewing any type of khat compared to chewers in the immigrant communities (Patel et al., 2005; Kassim et al., 2010). The finding of gender differences in correlates and patterns of khat use and dependence is consistent with previous studies (Brady et al., 1993; Nakajima et al 2013). Reported frequency and intensity of khat chewing as well as mood changes following khat abstinence were higher in men than in women. The gender by age interaction with a positive linkage between age and khat dependence in women only also supported our hypothesis, which is consistent with prior work (Khawaja et al., 2008; Bongard et al., 2011; Ali et al., 2004).
While the current finding of bi-dimensionality of the SDS-khat was consistent with studies testing dependence in cannabis users (Swift et al., 1998; Ferri et al., 2000), it was somewhat inconsistent with findings of other studies examining khat dependence in immigrant communities (Kassim et al., 2010) as well as studies focused on other drugs (Kaye and Darke, 2002; Lawrinson et al., 2007). In our study, items 3 and 4 collapsed into one domain which reflected desire to stop khat. This suggest a possibility that familial, cultural, and social dimension of khat chewing influenced the results. It is possible that khat users in our sample had not yet contemplated their dependence because khat chewing is highly prevalent and socially accepted (Cox and Rampes, 2003). As such, there may be a low level of self-awareness to make khat dependence as a serious concern (Sussman and Ames, 2001). This explanation may in part explain the modest reliability of the SDS-khat found in this study. The reliability of the scale was not altered when the item “Did you wish you could stop chewing khat?” (one of the items classified in the apathy factor) was removed (Cronbach's Alpha if item deleted, Table 3). Future study should elucidate differences in underlying mechanisms of cultural and psychosocial (Nabuzoka and Badhadhe, 2000) influences on khat chewing and dependence. The use of quantitative and qualitative approaches could be helpful in improving the conceptualization of khat dependence.
The strengths of this study includes the use of a validated measure to assess khat dependence (SDS-khat (Kassim et al., 2010), questionnaires to measure patterns of khat use, and a relatively large sample that included both male and female khat chewers. The results of this study is limited by using a cross-sectional method, self-selection bias, and a lack of examining the test-retest reliability of the SDS-khat. It is also possible that social desirability associated with face- to-face interviews influenced the results although we note this approach is reliable in a population with low literacy. However, it is possible that results on patterns of khat use and dependence in women were influenced by social desirability because khat chewing is viewed as unfavourable behaviour in this population.
In conclusion, this study demonstrated sound psychometric properties of SDS-khat in adult khat users in Yemen. Results also supported our hypothesis regarding gender differences in khat use patterns. The frequency, intensity, and symptoms associated with khat abstinence were higher in men than in women. Men reported higher levels of khat dependence symptoms than women. Older age was positively associated with khat dependence in women but not in men. Uni-dimensionality of the SDS-khat was not replicated. Implications of these findings warrant further investigation taking into account gender-specific patterns and correlates of khat use and dependence.
Acknowledgments
Role of funding sources: This study was supported by a FIRCA grant from the National Institutes of Health/Fogarty International Center (R03TW007219), an R21 National Institute for Drug Abuse grant (DA024626), and a grant from the Office of International Programs at the University of Minnesota. Funders have no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Footnotes
Contributors: Motohiro Nakajima helped in designing the study, organizing the data base and writing of the manuscript. Mohamed Alsoofi, Anisa Dokam, Najat Saem, and Abed Alsameai coordinated the data collection in Yemen. Mustafa al'Absi conceived the study, provided assistance with designing the study, provided advice regarding analysing and interpreting the results, and in writing of the manuscript.
Conflict of interest: None of the authors has conflict of interest
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Motohiro Nakajima, Email: mnakajim@umn.edu.
Anisa Dokam, Email: anisa_dokm@yahoo.com.
Abed Alsameai, Email: abednaji123@gmail.com.
Mohammed AlSoofi, Email: m_alsoofi@yahoo.com.
Najat Khalil, Email: najatsayem@gmail.com.
References
- al'Absi M, Grabowski J. Concurrent use of tobacco and khat: added burden on chronic disease epidemic. Addiction. 2012;107:451–452. doi: 10.1111/j.1360-0443.2011.03684.x. [DOI] [PubMed] [Google Scholar]
- Al-Motarreb A, Al-Habori M, Broadley KJ. Khat chewing, cardiovascular diseases and other internal medical problems: the current situation and directions for future research. J Ethnopharmacol. 2010;132:540–548. doi: 10.1016/j.jep.2010.07.001. [DOI] [PubMed] [Google Scholar]
- Ali AA, Al-Sharabi AK, Aguirre JM, Nahas R. A study of 342 oral keratotic white lesions induced by qat chewing among 2500 Yemeni. J Oral Pathol Med. 2004;33:368–372. doi: 10.1111/j.1600-0714.2004.00145.x. [DOI] [PubMed] [Google Scholar]
- Bastiani L, Siciliano V, Curzio O, Luppi C, Gori M, Grassi M, Molinaro S. Optimal scaling of the CAST and of SDS Scale in a national sample of adolescents. Addict Behav. 2013;38:2060–2067. doi: 10.1016/j.addbeh.2012.12.016. [DOI] [PubMed] [Google Scholar]
- Bongard S, al'Absi M, Khalil NS, Al Habori M. Khat use and trait anger: effects on affect regulation during an acute stressful challenge. Eur Addict Res. 2011;17:285–291. doi: 10.1159/000330317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brady KT, Grice DE, Dustan L, Randall C. Gender differences in substance use disorders. Am J Psychiatry. 1993;150:1707–1711. doi: 10.1176/ajp.150.11.1707. [DOI] [PubMed] [Google Scholar]
- Cattell RB. The scree test for the number of factors. Multivariate behavioral research. 1966;1:245–276. doi: 10.1207/s15327906mbr0102_10. [DOI] [PubMed] [Google Scholar]
- Cox G, Rampes H. Adverse effects of khat: a review. Adv Psychiatr Treat. 2003;9:456–463. [Google Scholar]
- El-Wajeh YA, Thornhill MH. Qat and its health effects. Br Dent J. 2009;206:17–21. doi: 10.1038/sj.bdj.2008.1122. [DOI] [PubMed] [Google Scholar]
- Ferri CP, Marsden J, De Araujo M, Laranjeira RR, Gossop M. Validity and reliability of the Severity of Dependence Scale (SDS) in a Brazilian sample of drug users. Drug and Alcohol Review. 2000;19:451–455. doi: 10.1080/713659418. [DOI] [PubMed] [Google Scholar]
- Gossop M, Darke S, Griffiths P, Hando J, Powis B, Hall W, Strang J. The Severity of Dependence Scale (SDS): psychometric properties of the SDS in English and Australian samples of heroin, cocaine and amphetamine users. Addiction. 1995;90:607–614. doi: 10.1046/j.1360-0443.1995.9056072.x. [DOI] [PubMed] [Google Scholar]
- Griffiths P. Qat use in London: a study of qat use among a sample of Somalis living in London. London: Home Office; 1998. Bd. Paper 26. [Google Scholar]
- Griffiths P, Gossop M, Wickenden S, Dunworth J, Harris K, Lloyd C. A transcultural pattern of drug use: qat (khat) in the UK. Br J Psychiatry. 1997;170:281–284. doi: 10.1192/bjp.170.3.281. [DOI] [PubMed] [Google Scholar]
- Hougton P, Ismail M, Salvage S. Not cathinone alone – dopamine, khat constituents and brain tissue; 2011. [Accessed 29 March 2014];Middlesex university: Khat Symposium. 2012 at http://darckhat.middlesex.wikispaces.net/file/view/Not+cathinone+alone+_dopamine+khat+constituents+and+brain+tissue_+Houghton+et+al.pdf.
- Kaiser HF. An index of factorial simplicity. Psychometrika. 1974;39:31–36. [Google Scholar]
- Kalix P. Cathinone, a natural amphetamine. Pharmacol Toxicol. 1992;70:77–86. doi: 10.1111/j.1600-0773.1992.tb00434.x. [DOI] [PubMed] [Google Scholar]
- Kassim S, Croucher R, Al'absi M. Khat dependence syndrome: A cross sectional preliminary evaluation amongst UK-resident Yemeni khat chewers. J Ethnopharmacol. 2013;146:835–841. doi: 10.1016/j.jep.2013.02.011. [DOI] [PubMed] [Google Scholar]
- Kassim S, Islam S, Croucher R. Validity and reliability of a Severity of Dependence Scale for khat (SDS-khat) J Ethnopharmacol. 2010;132:570–577. doi: 10.1016/j.jep.2010.09.009. [DOI] [PubMed] [Google Scholar]
- Kaye S, Darke S. Determining a diagnostic cut-off on the Severity of Dependence Scale (SDS) for cocaine dependence. Addiction. 2002;97:727–731. doi: 10.1046/j.1360-0443.2002.00121.x. [DOI] [PubMed] [Google Scholar]
- Kelly JP. Cathinone derivatives: a review of their chemistry, pharmacology and toxicology. Drug Test Anal. 2011;3:439–453. doi: 10.1002/dta.313. [DOI] [PubMed] [Google Scholar]
- Khawaja M, Al-Nsour M, Saad G. Khat (Catha edulis) Chewing during Pregnancy in Yemen: Findings from a National Population Survey. Matern Child Health J. 2008;12:308–312. doi: 10.1007/s10995-007-0231-2. [DOI] [PubMed] [Google Scholar]
- Lawrinson P, Copeland J, Gerber S, Gilmour S. Determining a cut-off on the Severity of Dependence Scale (SDS) for alcohol dependence. Addict Behav. 2007;32:1474–1479. doi: 10.1016/j.addbeh.2006.09.005. [DOI] [PubMed] [Google Scholar]
- Nabuzoka D, Badhadhe F. Use and perception of khat among young Somalis in a UK city. Addiction Research. 2000;8:5–26. [Google Scholar]
- Nakajima M, al'Absi M, Dokam A, Alsoofi M, Khalil NS, Al Habori M. Gender differences in patterns and correlates of khat and tobacco use. Nicotine Tob Res. 2013;15:1130–1135. doi: 10.1093/ntr/nts257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Norman GR, Streiner DL. PDQ statistics. PMPH-USA; 2003. At http://f3.tiera.ru/2/M_Mathematics/MV_Probability/MVsa_Statistics%20and%20applications/Norman%20G.R.,%20Streiner%20D.L.%20PDQ%20Statistics%20(3ed.,%20B.C.%20Decker,%202003)(ISBN%201550092073)(O)(230s)_MVsa_.pdf. [Google Scholar]
- Numan N. The Green Leaf: Khat. World Journal of Medical Sciences. 2012;7:210–223. [Google Scholar]
- Patel SL, Murray R, Britain G. Home Office London; 2005. [Acessed 12/2/2014]. Khat use among Somalis in four English cities. http://collection.europarchive.org/tna/20080205132101/homeoffice.gov.uk/rds/pdfs05/rdsolr4705.pdf. [Google Scholar]
- Sussman SY, Ames SL. The social psychology of drug abuse. Open University Press; Buckingham, GB: 2001. [Google Scholar]
- Swift W, Hall W, Didcott P, Reilly D. Patterns and correlates of cannabis dependence among long-term users in an Australian rural area. Addiction. 1998;93:1149–1160. doi: 10.1046/j.1360-0443.1998.93811493.x. [DOI] [PubMed] [Google Scholar]
- Topp L, Mattick RP. Choosing a cut-off on the Severity of Dependence Scale (SDS) for amphetamine users. Addiction. 1997;92:839–845. [PubMed] [Google Scholar]
- Tsai JH, Tang TC, Yeh YC, Yang YH, Yeung TH, Wang SY, Chen CC. The Chinese version of the Severity of Dependence Scale as a screening tool for benzodiazepine dependence in Taiwan. Kaohsiung J Med Sci. 2012;28:225–230. doi: 10.1016/j.kjms.2011.06.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wedegaertner F, al-Warith H, Hillemacher T, te Wildt B, Schneider U, Bleich S, Breitmeier D. Motives for khat use and abstinence in Yemen--a gender perspective. BMC Public Health. 2010;10:735. doi: 10.1186/1471-2458-10-735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zein ZA. Polydrug abuse among Ethiopian university students with particular reference to khat (Catha edulis) J Trop Med Hyg. 1988;91:71–75. [PubMed] [Google Scholar]