

Abstract
An intussusception due to colonic adenocarcinoma has sometimes been reported. However, to the best of our knowledge, reports of intussusception due to rectal adenocarcinoma are extremely rare. In this report, the case of a young man with rectal adenocarcinoma causing intussusception is described. A 24-year-old man visited a hospital complaining of abdominal pain, and an upper rectal cancer was diagnosed by colonoscopy. Computed tomography showed intussusception caused by a large tumor in the pelvis and absence of distant metastases. Locally advanced rectal cancer causing intussusception was diagnosed, and a low anterior resection was performed. Intraoperatively, repair of the invagination could not be accomplished easily; therefore, the repair was abandoned. Instead, the tumor was removed en bloc to avoid dissemination of the cancer. Histopathologically, the tumor was diagnosed as a poorly differentiated adenocarcinoma, pStage IIA. The patient has no evidence of recurrence at 10 mo after the operation.
Keywords: Adult intussusception, En bloc resection, Low anterior resection, Rectal adenocarcinoma, Young cancer
Core tip: Intussusception is uncommon in adults compared with children, and colonic tumors have sometimes been reported as causes of adult intussusception. On the other hand, there have been only a few reports of intussusception due to rectal adenocarcinoma in the English literature. In this report, an extremely rare case of sporadic rectal adenocarcinoma causing intussusception in a young man who underwent curative resection and has survived is described.
INTRODUCTION
Intussusception is a common disease and one of the leading causes of intestinal obstruction and acute abdominal emergencies in children[1]. On the other hand, adult intussusception is unusual, accounting for only 5% of all cases of intussusception and 1%-5% of all cases of bowel obstruction[2-4]. The cause of intussusception differs between the pediatric and adult populations. In adults, a demonstrable etiology is present in about 70%-90% of all cases with intussusception, whereas about 90% of pediatric cases of intussusception are idiopathic[1,5-8]. Intraluminal lesions form leading edges of most cases of adult intussusception. Malignant tumor is often found as the etiology of adult intussusception, and colonic adenocarcinomas are sometimes reported as causes of intussusception[5,6,9-12]. However, there appear to be only a few reports of intussusception due to rectal adenocarcinoma in the English literature[13]. Therefore, an extremely rare case of a young man with sporadic rectal adenocarcinoma causing intussusception who underwent curative resection and has survived is described.
CASE REPORT
A 24-year-old man was referred for management of rectal cancer. Initially, he had visited another hospital with a complaint of abdominal pain and tenesmus, and an upper rectal tumor measuring 100 mm in diameter, without invagination, was diagnosed by colonoscopy (Figure 1). He had a family history of gastrointestinal cancer; his maternal uncle and grandmother had died of colorectal cancer, and his paternal grandfather had died of gastric cancer. At the time of his transfer to our hospital, laboratory tests were within the normal range, including a carcino-embryonic antigen level of 0.83 ng/mL and a carbohydrate antigen 19-9 (CA19-9) level of 9.2 U/mL. Computed tomography (CT) and magnetic resonance imaging showed intussusception caused by a large tumor in the pelvis and absence of distant metastases (Figure 2). Locally advanced upper rectal cancer causing intussusception was diagnosed, and a low anterior resection with complete removal of all regional lymph nodes and total mesorectal excision was performed. Intraoperatively, the invagination could not be repaired easily; therefore, the repair was abandoned. Instead, the tumor was removed en bloc to avoid dissemination of the cancer. After the proctectomy, coloproctostomy with a temporary diverting ileostomy was performed. Histopathologically, the surgical margin was negative for cancer, and based on the classification of the seventh edition of the Union for International Cancer Control (UICC), the tumor was diagnosed as a poorly differentiated adenocarcinoma, pStage IIA (T3, N0, M0) (Figures 3 and 4)[14]. To exclude Lynch syndrome, microsatellite status and immunohistochemistry of four deoxyribonucleic acid (DNA) mismatch repair proteins, including mutL homolog 1, postmeiotic segregation increased 2, mutS homologue 2 and mutS homologue 6, were checked; the tumor was microsatellite stable and retained expression of all mismatch repair proteins on immunohistochemistry.
Figure 1.
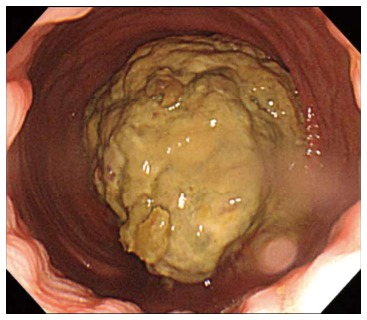
Colonoscopy showing a huge tumor at the upper rectum. The tumor, measuring 100 mm in diameter, does not show invagination on colonoscopy.
Figure 2.
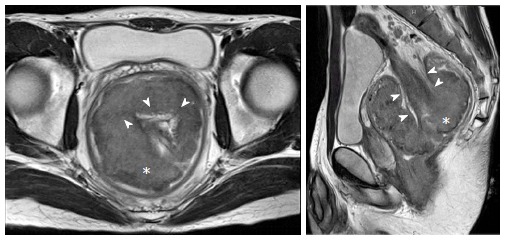
Magnetic resonance imaging showing intussusception caused by a tumor in the pelvis. The upper rectal tumor (asterisk) causes intussusception (arrowheads) as a leading edge.
Figure 3.

Specimen resected in en bloc fashion. The tumor is located at the upper rectum, and the margin is negative for cancer. Pathological staging is pStage IIA (T3, N0, M0).
Figure 4.
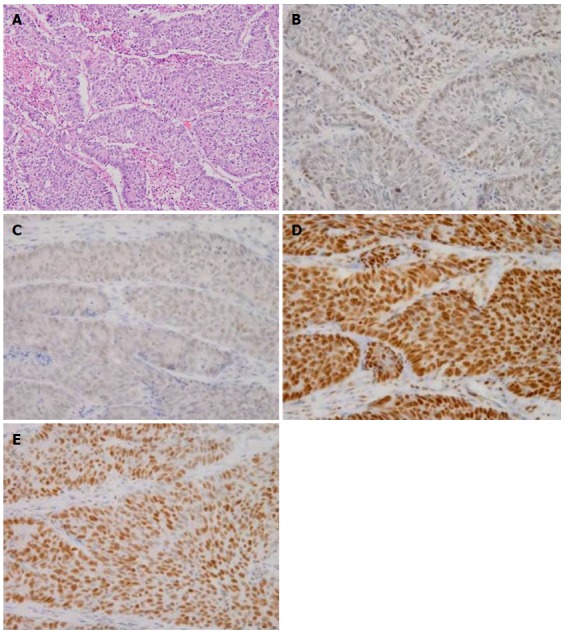
Microscopic findings and immunohistochemistry for deoxyribonucleic acid mismatch repaire proteins (× 200). The tumor is a poorly differentiated adenocarcinoma. Immunohistochemical expression of mutL homolog 1 (MLH1), postmeiotic segregation increased 2 (PMS2), mutS homologue 2 (MSH2) and mutS homologue 6 (MSH6) is retained. HE: Hematoxylin and eosin stain. A: HE; B: MLH1, C: PMS2; D: MSH2, E: MSH6.
The patient underwent adjuvant XELOX (capecitabine plus oxaliplatin) for 6 mo, and 9 mo after the low anterior resection, he was alive without evidence of recurrence.
DISCUSSION
Adult intussusception is uncommon and has some different characteristics from pediatric intussusception. Pediatric patients with intussusception often show acute symptoms of abdominal pain, bloody stools and a palpable abdominal mass, the so-called classic presentation triad[1]. On the other hand, adult patients with intussusception rarely show the complete triad[9]. They have subacute or chronic symptoms caused by intestinal obstruction, including abdominal pain, nausea and vomiting[5,9-12]. According to some previous retrospective institutional reviews of 20-60 cases of adult intussusception treated surgically[5,9-12], colonic intussusception is minor (15.0%-35.0%) compared with enteric intussusception. Most cases of adult intussusception are caused by intraluminal lesions, and malignant tumors are responsible for 22.2%-46.6% of adult intussusception cases[5,9-12]. With regard to colonic adenocarcinoma, it accounted for 33.3%-80.0% of cases of colonic intussusception and 7.3%-25% of all adult intussusception cases[5,9-12]. A literature search was conducted, and it identified only a few English manuscripts, including case reports, about rectal intussusception caused by rectal adenocarcinoma[13]. In this case, a preoperative diagnosis of intussusception was made by computed tomography, but colonoscopy did not show the intussusception. It is sometimes difficult to diagnose adult intussusception preoperatively; the rate of preoperative diagnosis is reported to range from 32% to 70%[5,9-12]. The accuracy of computed tomography for preoperative diagnosis of adult intussusception is better than that of other examinations, including abdominal ultrasonography, barium enema study, and colonoscopy[5,9-12].
In the present case, the patient was diagnosed as having rectal cancer at a young age. Young patients with colorectal cancers are sometimes encountered, and they more frequently have Lynch syndrome, which is caused by germline mutations of DNA mismatch repair genes[15]. Microsatellite status and immunohistochemistry for DNA mismatch repair proteins were examined for the present tumor, but the patient did not have Lynch syndrome.
In conclusion, an extremely rare case of a young man with a sporadic rectal adenocarcinoma causing intussusception was reported.
ACKNOWLEDGMENTS
The authors would like to thank Dr Hiroko Toda and Hiroyuki Yanai for help in making the pathological diagnosis.
COMMENTS
Case characteristics
A 24-year-old man with a family history of gastroenterological cancers.
Clinical diagnosis
Abdominal pain and tenesmus.
Differential diagnosis
Infectious enteritis and inflammatory bowel disease.
Laboratory diagnosis
Carcino-embryonic antigen 0.83 ng/mL, carbohydrate antigen 19-9 9.2 U/mL and other laboratory date were within normal limits.
Imaging diagnosis
Colonoscopy showed an upper rectal tumor, and computed tomography showed intussusception caused by a large tumor in the pelvis and absence of distant metastases.
Pathological diagnosis
The tumor was diagnosed as a poorly differentiated adenocarcinoma, pStage IIA.
Treatment
The patient underwent a low anterior resection with complete removal of all regional lymph nodes and total mesorectal excision and adjuvant XELOX (capecitabine plus oxaliplatin).
Related reports
Reports of intussusception due to rectal adenocarcinoma are extremely rare.
Term explanation
Microsatellite status and immunohistochemistry for deoxyribonucleic acid mismatch repair proteins used for diagnosis of Lynch syndrome and sporadic microsatellite instability cancers.
Experiences and lessons
If the invagination cannot be repaired easily, we should abandon the repair and remove the tumor en bloc to avoid dissemination of the cancer.
Peer review
The authors described an extremely rare case of a young man with a sporadic rectal adenocarcinoma causing intussusception in this manuscript.
Footnotes
P- Reviewer: Rekhi B S- Editor: Nan J L- Editor: O’Neill M E- Editor: Du P
References
- 1.Jiang J, Jiang B, Parashar U, Nguyen T, Bines J, Patel MM. Childhood intussusception: a literature review. PLoS One. 2013;8:e68482. doi: 10.1371/journal.pone.0068482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Laws HL, Aldrete JS. Small-bowel obstruction: a review of 465 cases. South Med J. 1976;69:733–734. doi: 10.1097/00007611-197606000-00021. [DOI] [PubMed] [Google Scholar]
- 3.Stewardson RH, Bombeck CT, Nyhus LM. Critical operative management of small bowel obstruction. Ann Surg. 1978;187:189–193. doi: 10.1097/00000658-197802000-00017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Donhauser JL, Kelly EC. Intussusception in the adult. Am J Surg. 1950;79:673–677. doi: 10.1016/0002-9610(50)90333-3. [DOI] [PubMed] [Google Scholar]
- 5.Azar T, Berger DL. Adult intussusception. Ann Surg. 1997;226:134–138. doi: 10.1097/00000658-199708000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sanders GB, Hagan WH, Kinnaird DW. Adult intussusception and carcinoma of the colon. Ann Surg. 1958;147:796–804. [PMC free article] [PubMed] [Google Scholar]
- 7.Nagorney DM, Sarr MG, McIlrath DC. Surgical management of intussusception in the adult. Ann Surg. 1981;193:230–236. doi: 10.1097/00000658-198102000-00019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Begos DG, Sandor A, Modlin IM. The diagnosis and management of adult intussusception. Am J Surg. 1997;173:88–94. doi: 10.1016/S0002-9610(96)00419-9. [DOI] [PubMed] [Google Scholar]
- 9.Wang N, Cui XY, Liu Y, Long J, Xu YH, Guo RX, Guo KJ. Adult intussusception: a retrospective review of 41 cases. World J Gastroenterol. 2009;15:3303–3308. doi: 10.3748/wjg.15.3303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yakan S, Caliskan C, Makay O, Denecli AG, Korkut MA. Intussusception in adults: clinical characteristics, diagnosis and operative strategies. World J Gastroenterol. 2009;15:1985–1989. doi: 10.3748/wjg.15.1985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Eisen LK, Cunningham JD, Aufses AH. Intussusception in adults: institutional review. J Am Coll Surg. 1999;188:390–395. doi: 10.1016/s1072-7515(98)00331-7. [DOI] [PubMed] [Google Scholar]
- 12.Goh BK, Quah HM, Chow PK, Tan KY, Tay KH, Eu KW, Ooi LL, Wong WK. Predictive factors of malignancy in adults with intussusception. World J Surg. 2006;30:1300–1304. doi: 10.1007/s00268-005-0491-1. [DOI] [PubMed] [Google Scholar]
- 13.Mussack T, Szeimies U. Sigmoidorectal intussusception caused by rectal carcinoma: multislice CT findings. Abdom Imaging. 2002;27:566–569. doi: 10.1007/s00261-001-0105-9. [DOI] [PubMed] [Google Scholar]
- 14.Sobin LH, Gospodarowicz MK, Wittekind C. TNM Classification of Malignant Tumours, 7th Edition. UK, Chichester: Wiley-Blackwell; 2009. [Google Scholar]
- 15.Boland CR, Thibodeau SN, Hamilton SR, Sidransky D, Eshleman JR, Burt RW, Meltzer SJ, Rodriguez-Bigas MA, Fodde R, Ranzani GN, et al. A National Cancer Institute Workshop on Microsatellite Instability for cancer detection and familial predisposition: development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res. 1998;58:5248–5257. [PubMed] [Google Scholar]