

Abstract
Lean soft tissue (LST), a surrogate of skeletal muscle mass, is largely limited to appendicular body regions. Simple and accurate methods to estimate lower limbs LST are often used in attempts to partition out the influence of body size on performance outputs. The aim of the current study was to develop and cross-validate a new model to predict lower limbs LST in boys aged 10–13 years, using dual-energy X-ray absorptiometry (DXA) as the reference method. Total body and segmental (lower limbs) composition were assessed with a Hologic Explorer-W QDR DXA scanner in a cross-sectional sample of 75 Portuguese boys (144.8±6.4 cm; 40.2±9.0 kg). Skinfolds were measured at the anterior and posterior mid-thigh, and medial calf. Circumferences were measured at the proximal, mid and distal thigh. Leg length was estimated as stature minus sitting height. Current stature expressed as a percentage of attained predicted mature stature (PMS) was used as an estimate of biological maturity status. Backward proportional allometric models were used to identify the model with the best statistical fit: ln (lower limbs LST) = 0.838× ln (body mass) +0.476× ln (leg length) – 0.135× ln (mid-thigh circumference) – 0.053× ln (anterior mid-thigh skinfold) – 0.098× ln (medial calf skinfold) – 2.680+0.010× (percentage of attained PMS) (R = 0.95). The obtained equation was cross-validated using the predicted residuals sum of squares statistics (PRESS) method (R 2 PRESS = 0.90). Deming repression analysis between predicted and current lower limbs LST showed a standard error of estimation of 0.52 kg (95% limits of agreement: 0.77 to −1.27 kg). The new model accurately predicts lower limbs LST in circumpubertal boys.
Introduction
Skeletal muscle mass in the lower extremities is well correlated with a variety of fitness measures in pediatric physiology and health and exercise research [1]–[6]. Oxygen uptake is probably the most frequently reported physical capacity measurement in children and, for example, is not clear what the pattern of change with age or maturation is once values are dimensionally scaled [7], [8]. In heterogeneous samples of boys and men, it has been demonstrated that estimates of lower leg muscle [3] or thigh muscle [6] volume are more relevant allometric scaling denominators for partitioning out the influence of body size on peak oxygen uptake than either body mass or fat-free mass.
Early dissection studies have indicated that the muscles in the lower extremities increase their relative contribution to total muscle mass from about 40% at birth to 55% at maturity [9]. Other studies of regional variation in skeletal muscle were based on radiography and limited largely to the arm and calf [10]. Boys gain about 30% in calf muscle mass width during adolescence [10], but more recent imaging techniques have not yet been used systematically to address this issue in youth.
Multi-scan magnetic resonance imaging (MRI) and computerized axial tomography (CT) are considered the “criterion” methods for evaluating skeletal muscle mass [11]. MRI is not widely available for use in research and clinical practice while CT includes exposure to radiation which limits its application in children and adolescents [12]. Other approaches to estimate skeletal muscle mass, include total-body potassium [13] and bioelectrical impedance [14]. Densitometric techniques rely on specific assumptions concerning the density of fat-free mass (1.1 g/mL) which is assumed to be stable in adults but may vary considerably in children by age, gender, maturity status and perhaps ethnicity [15], [16]. The estimated density of fat-free mass increases from 1.0826 to 1.1013 g/mL in boys from 4 to 23 years [17]. Dual-energy X-ray absorptiometry (DXA) is a non-invasive protocol with a minimal radiation dose (1 mSv or 1/100th of the equivalent radiation exposure of a chest x-ray) [18]. The DXA method provides total and lean soft tissue (LST) estimates of the extremities, and a large portion of total-body skeletal muscle is within the fat-free appendicular compartment [19]. DXA-determined appendicular LST has also been validated against criterion methods such as CT [20], [21].
Though useful, the availability of DXA in field settings is limited. Estimates of LST based on anthropometry are thus potentially useful, especially among youth. A popular anthropometric method [22] characterizes the lower limb as the sum of six truncated cones based on lengths, circumferences and skinfold thicknesses. The method was originally developed among young adults (with 32 male and 15 female) and has been applied in children and adolescents [4], [23], [24]. Anthropometric models for appendicular LST (upper and lower limbs combined) in young athletes of both sexes have also been developed and cross-validated [25]. A recent attempt [26] to cross-validate the regression equation of Jones and Pearson [22] in youth (83 girls, 85 boys, 11.0±0.7 years) noted a significantly higher thigh volume with DXA (4.43±1.23 L) than with the anthropometric estimate (4.39±1.22 L). Addition of body mass and the sum of anterior and posterior thigh skinfolds to the model resulted in a new predictive equation (R 2 = 0.95). The available research has not systematically considered the potential contribution of biological maturation to inter-individual variability in total and lean soft tissues. Correlations between skeletal age and radiographic widths of upper arm and calf muscle increased from childhood (7–10 years, r = 0.16–0.18) to adolescence (11–16 years, r = 0.51–0.61) in boys; corresponding correlations in girls, on the other hand, increased with age for arm musculature (7–8 years, r = 0.27; 9–14 years, r = 0.45) but not for calf musculature (7–8 years, r = 0.41; 9–14 years, r = 0.39) [27]. The direction of correlations between skeletal age and arm and calf muscle widths in boys across chronological age (CA) groups suggests a need to consider inter-individual differences in maturity status in estimates of lower limbs LST in circumpubertal children. Allowing for the limited data on youth, the present study attempted to develop a non-invasive estimate of lower limbs LST in circumpubertal boys and to cross-validate the new model using DXA measures as the reference.
Materials and Methods
Ethics Statement
The study was approved by the Portuguese Foundation for Science and Technology [PTDC/DTP-DES/1178/2012] and by the scientific board of the Faculty of Human Kinetics at the Technical University of Lisbon. The study was conducted in accordance with the Declaration of Helsinki for human studies by the World Medical Association [28]. All participants, parents or legal guardians were informed about the objectives of the study and provided appropriate informed assent and written informed consent.
Participants
The present study is limited to healthy boys of European ancestry (n = 75), 10–13 years of age. Participants were recruited voluntarily from the school population in the Lisbon metropolitan area (Portugal).
Chronological Age and Anthropometry
Chronological age was calculated as the difference between date of birth and date of measurement. Anthropometry was performed by a single experienced observer following standard procedures [29]. Stature and sitting height were measured to the nearest 0.1 cm with a Harpenden stadiometer (model 98.603, Holtain Ltd, Crosswell, UK and Harpenden sitting height table, model 98.607, Holtain Ltd, Crosswell, UK, respectively) and body mass was measured to the nearest 0.1 kg using an electronic scale (Seca, Hamburg, Germany). Leg length was estimated as stature minus sitting height. Circumference at the gluteal furrow (highest possible horizontal circumference), mid-thigh (largest mid-thigh circumference) and distal thigh (minimum circumference above the knee) were measured on the right site of the body. Lengths between each circumference level were also measured to estimate total thigh length. Anterior and posterior mid-thigh and medial calf skinfolds were measured to the nearest mm using a Lange Caliper (Beta Technology, Ann Arbor, MI, USA). Technical errors of measurement were previously reported for the anthropometric dimensions [26] and all were well within the range of several health surveys in the United States and a variety of field surveys [30]. Mid-thigh circumference (C m-t) was corrected for subcutaneous adipose tissue thickness [31]. The corrected mid-thigh circumference (CC m-t) was calculated as CC m-t = C m-t – πS, where S stands for the skinfold measurement, which is assumed to be twice the subcutaneous adipose tissue thickness.
Biological Maturity
Chronological age, stature, and body mass of each boy and midparent stature were used to predict mature (adult) stature using the Khamis–Roche protocol [32]. Parent heights were extracted from national identification cards which included height measured to the nearest centimeter. Measurements were taken by experienced, but not necessarily trained observers. A similar protocol was used in previous studies [33], [34]. The median error bound (median absolute deviation) between actual and predicted mature stature (PMS) at 18 years of age is 2.2 cm in boys [32]. Ages at attaining specific percentages of mature stature are related to ages at attaining specific skeletal ages and stages of puberty in boys followed longitudinally from late childhood through adolescence [35]. Percentage of attained PMS (% PMS) is also related to skeletal age in youth football (American) and soccer players of the same age range as the study sample [33], [36]. Percentage of attained PMS was expressed as a z-score relative to age-specific (half-year intervals) means and standard deviations from the Berkeley Guidance Study [37]; the z-score (z PMS) was used as the indicator of maturity status for each boy.
Dual energy X-ray absorptiometry
A Hologic Explorer-W, fan-bean densitometer, software QDR for Windows version 12.4 (Hologic, Waltham, MA, USA) was used to perform whole body scans. The procedure also allows measurement of segmental composition: arm, leg and trunk. Daily calibration of the scanner was performed using a phantom spine containing composites of bone, fat and LST. Participants were positioned on the scanner bed according to manufacturer recommendations. A single lab technician positioned the participants and performed the scans according to the manual provided by the manufacturer. The lower limbs on each image were sectioned as follows: all tissue distal to a line drawn through and perpendicular to the axis of the femoral neck and angled with the pelvic brim to the phalange tips. Total lower limb composition was estimated by adding the mass of the left and right legs. Mean variation between measured and reconstructed absolute whole-body mass with DXA software was 0.9%. Based on test-retest in 10 individuals, the coefficients of variation for percent body fat and LST were 1.6% and 0.8%, respectively.
Statistical analyses
Visual inspections of data were made using stem-and-leaf diagram and box-and-whisker plots to examine central tendency, variability, distributions and potential outliers. Subsequently, Gaussian distribution of variables was confirmed with normal Q-Q plots, de-trended normal Q-Q plots and Kolmogorov-Smirnov (K-S) test with Lilliefors significance correction. Descriptive statistics were calculated for the total sample (mean, standard deviation and range).
A backward multiple linear regression on ln y, based on proportional allometric models [4], [38], was used to fit the unknown parameters that best predict lower limb LST determined with DXA. Based on analytical [i.e., Pearson's product moment correlation coefficients (ry,x) between lower limbs LSTDXA (y) with CA, maturity status and body descriptors (x)] and biological assumptions, the new model (NM) considered CA, CA2, % PMS or z PMS as exponential terms in addition to body mass, leg length, C m-t, stature × CC m-t 2, anterior and posterior mid-thigh and medial calf skinfolds:
 |
(1) |
A tolerance >0.10 and a variance inflation factor <10 was set to avoid collinearity between the explanatory variables [39].
The new model was internally cross-validated by using the predicted residuals sum of squares (PRESS) statistics method [40]. PRESS statistics uses all cases and is considered a statistical jackknife procedure [41]. The technique produces as many models as the number of cases. An independent model is obtained based on n-1 data subsets for each participant and this permits the determination of individual residuals. A PRESS residual for a given participant is the difference between the actual response of the left-out case and the predicted response. Prediction of the respective case involves a different prediction equation for a statistical fit that excludes the case [40]. Overall, the PRESS statistic is a function of the sum of squares (SS) of all residuals. The PRESS statistic is always higher than the error (i.e., SS) from MANOVA results. Alternative measures of model adequacy (R 2 PRESS) and standard error of estimation (SEEPRESS) were also calculated [40].
Agreement between the reference method (lower limbs LSTDXA) and the estimation (lower limbs LSTNM) was assessed using Deming regression (i.e., least products regression method which accounts for the error of both x and y variables) and standard error of estimation (Sy·x) [42]. Data were then visually inspected by plotting residuals (prediction errors) against predicted values. This plot is similar to the plot suggested by Bland and Altman [43], except that predicted values of lower limbs LST (using the new developed equation) are plotted on the x-axis rather than the average of predicted and measures of lower limbs LST [25]. To test for proportional bias, Bland and Altman [43] have recommended plotting error against the average of two the methods. Although they have demonstrated that this is correct when considering the agreement of two existing methods, Hopkins [44] has demonstrated that in criterion/reference validity studies this method will indicate positive proportional bias when no proportional bias exists. This is due to the mathematical relation that occurs when a method is calibrated against a reference using least-squares regression; only vertical error (error in predicting the criterion) is minimized around the regression slope [45]. If errors were associated with the magnitude of the values, heteroscedasticity was examined by calculating the correlation coefficients between the absolute differences and the predicted values of lower limbs LST. Constant error variance (homoscedasticity) can be assumed if the correlations approach zero [46], [47]. Correlation coefficients were interpreted as follows: trivial (r<0.1), small (0.1<r<0.3) moderate (0.3<r<0.5), large (0.5<r<0.7), very large (0.7<r<0.9), nearly perfect (r>0.9) and perfect (r = 1) [48]. Finally, if measurement differences were normally distributed, reliability was assessed on the original scale using the standard error of measurement and 95% limits of agreement [43].
Statistical analyses were performed using IBM SPSS version 19.0 software (SPSS, Inc., IBM Company; NY, USA), GraphPad Prism version 5.03 software (GraphPad Software, Inc.; La Jolla, CA, USA) and MedCalc version 12.2.1 software (MedCalc; Mariakerke, Belgium). Alpha level was set at 0.05.
Results
Descriptive statistics for CA, estimated maturity status and DXA body composition are summarized in Table 1. All variables fitted a normal distribution (K-S = 0.37 to 1.18; p>0.05). Mean percentage of attained PMS (81.5±2.3%) for the present sample was equivalent of that of the sample on which the physical maturity-prediction protocol was based (81.6±1.2% at 11.0 years) [49]. The means and standard deviations for percent of total body fatDXA, LSTDXA, lower limbs fat percentageDXA and lower limbs LSTDXA were 26.4 (±8.1%), 29.0 (±4.2 kg), 31.7 (±8.3%) and 10.0 (±1.7 kg), respectively.
Table 1. Descriptive statistics (n = 75) for chronological age, maturity status and body composition, and results of the Kolmogorov–Smirnov test for checking the normality of the distribution.
| Mean ± SD | Range (min – max) | Kolmogorov–Smirnov | ||
| Value | p | |||
| Chronological age (years) | 11.12±0.69 | 10.27 to 13.08 | 1.18 | 0.12 |
| Percentage of PMS (%) | 81.5±2.3 | 77.3 to 90.3 | 0.70 | 0.72 |
| z-score for PMS (z PMS) | 0.04±0.92 | −2.07 to 2.40 | 0.74 | 0.65 |
| DXA total body | ||||
| BMD (g•cm−2) | 0.84±0.06 | 0.69 to 0.96 | 0.37 | 0.99 |
| BMC (kg) | 1.22±0.17 | 0.86 to 1.66 | 0.55 | 0.93 |
| Fat (%) | 26.4±8.1 | 14.0 to 44.6 | 0.77 | 0.60 |
| Fat (kg) | 11.2±5.8 | 3.6 to 27.6 | 1.03 | 0.24 |
| Lean soft tissue (kg) | 29.0±4.2 | 20.7 to 39.8 | 0.73 | 0.66 |
| DXA lower limbs | ||||
| BMD (g•cm−2) | 0.84±0.07 | 0.68 to 1.04 | 0.51 | 0.96 |
| BMC (kg) | 0.44±0.08 | 0.30 to 0.68 | 0.87 | 0.43 |
| Fat (%) | 31.7±8.3 | 16.0 to 50.2 | 0.56 | 0.92 |
| Fat (kg) | 4.9±2.3 | 1.3 to 10.9 | 1.16 | 0.13 |
| Lean soft tissue (kg) | 10.0±1.7 | 6.9 to 13.9 | 0.74 | 0.64 |
Abbreviations: PMS, predicted mature stature; DXA, dual x-ray absorptiometry; BMD, bone mineral density; BMC, Bone mineral content.
Relationships between ln lower limbs LSTDXA and the chronovariables [i.e., CA, percent of attained PMS and z-score for age (% attained PMS)] are illustrated in Figure 1 (panels a–c). The relationship between CA and lower limbs LSTDXA is linear, while relationships between % PMS and z PMS with lower limbs LSTDXA are somewhat non-linear. The correlation between CA and lower limbs LSTDXA is 0.30, while the corresponding correlations for % PMS and z PMS are 0.71 and 0.62, respectively (p<0.01).
Figure 1. Relationship of the ln transformed lower limbs lean soft tissue (LSTDXA) with chronological age (CA, panel a), percentage of predicted mature stature attained at the time of study (% PMS, panel b), and z-score for % PMS (z PMS, panel c).

Anthropometric characteristics for the total sample, results of the Kolmogorov–Smirnov test, and bivariate correlations of anthropometry with CA and estimated maturity status are shown in Table 2. The current sample has a mean stature and mean body mass which approximate, respectively, the 56th and 60th age-specific percentiles for U.S. boys [50]. Correlations between CA and maturity status and anthropometric variables ranged from trivial (r = 0.01) to very large (r = 0.73), suggesting the possibility of collinearity occurrence between some exponential terms and body size descriptors.
Table 2. Descriptive statistics (n = 75) for anthropometric variables, results of the Kolmogorov–Smirnov test for checking the normality of the distribution, and bivariate correlations of anthropometry with chronological age and maturity status.
| Mean ± SD | Range (min – max) | Kolmogorov–Smirnov | Correlation | |||||||
| CA | % PMS | z PMS | ||||||||
| Value | p | r | 95% CI | r | 95% CI | r | 95% CI | |||
| Stature (cm) | 144.8±6.4 | 127.9 to 163.5 | 0.52 | 0.95 | 0.36 | 0.15 to 0.55 | 0.73 | 0.60 to 0.82 | 0.58 | 0.41 to 0.71 |
| Body mass (kg) | 40.2±9.0 | 24.4 to 66.5 | 1.17 | 0.13 | 0.15 | −0.01 to 0.37 | 0.64 | 0.48 to 0.76 | 0.71 | 0.57 to 0.81 |
| Lengths (cm) | ||||||||||
| Leg | 69.6±4.2 | 60.2 to 78.5 | 0.43 | 0.99 | 0.34 | 0.13 to 0.53 | 0.63 | 0.47 to 0.75 | 0.49 | 0.30 to 0.65 |
| Thigh | 27.8±3.9 | 17.3 to 36.2 | 0.58 | 0.89 | 0.12 | −0.11 to 0.34 | 0.15 | −0.08 to 0.36 | 0.06 | −0.17 to 0.29 |
| Circumferences (cm) | ||||||||||
| Proximal thigh | 46.8±6.2 | 36.5 to 66.7 | 0.97 | 0.30 | 0.05 | −0.18 to 0.27 | 0.54 | 0.35 to 0.68 | 0.68 | 0.54 to 0.79 |
| Mid-thigh | 41.3±5.4 | 26.0 to 54.0 | 0.85 | 0.47 | 0.16 | −0.08 to 0.37 | 0.52 | 0.33 to 0.67 | 0.54 | 0.35 to 0.68 |
| Distal thigh | 34.3±4.4 | 27.5 to 47.0 | 1.19 | 0.12 | 0.01 | −0.22 to 0.23 | 0.47 | 0.27 to 0.63 | 0.64 | 0.49 to 0.76 |
| Skinfold thickness (mm) | ||||||||||
| Anterior mid-thigh | 21±8 | 7 to 42 | 0.85 | 0.47 | −0.19 | −0.40 to 0.04 | 0.21 | −0.02 to 0.41 | 0.51 | 0.32 to 0.66 |
| Posterior mid-thigh | 18±8 | 6 to 37 | 1.09 | 0.19 | −0.07 | −0.30 to 0.16 | 0.31 | 0.09 to 0.50 | 0.53 | 0.34 to 0.68 |
| Medial calf | 14±6 | 4 to 28 | 1.11 | 0.17 | −0.04 | −0.27 to 0.19 | 0.41 | 0.20 to 0.58 | 0.62 | 0.46 to 0.74 |
Abbreviations: CA, Chronological age; PMS, predicted mature stature; r, Pearson's product moment correlation coefficient; 95% CI, 95% confidence interval.
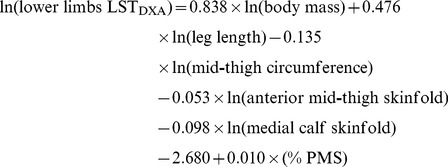
The allometric regression model for the prediction of lower limbs LST is given in Table 3. The new model included ln body mass, ln leg length, ln mid-thigh circumference, ln anterior mid-thigh skinfold, ln medial calf skinfold and percent of attained PMS. Its association with lower limbs LSTDXA was nearly perfect (R = 0.95). The prediction equation was:
 |
(2) |
Table 3. Proportional multiplicative allometric regression model and internal cross-validation for the prediction of DXA-measured lower limbs lean soft tissue*.
| Predictors | Model summary | ||||||||
| y | x i | β Unstandardized | 95% CI | Tolerance | VIF | R | SEE | Cross-validation | |
| R2 PRESS | SEEPRESS | ||||||||
| ln (lower limbs LSTDXA) | Constant | −2.680 | −4.308 to −1.052 | ||||||
| ln (body mass) | 0.838 | 0.616 to 1.061 | 0.231 | 4.332 | |||||
| ln (leg length) | 0.476 | 0.067 to 0.884 | 0.540 | 1.853 | |||||
| ln (mid-thigh circumference) | −0.135 | −0.412 to 0.143 | 0.219 | 4.568 | |||||
| ln (anterior mid-thigh skinfold) | −0.053 | −0.129 to 0.024 | 0.306 | 3.264 | |||||
| ln (medial calf skinfold) | −0.098 | −0.176 to 0.020 | 0.347 | 2.878 | |||||
| % PMS | 0.010 | −0.002 to 0.021 | 0.480 | 2.084 | |||||
| 0.95 | 0.07 | 0.90 | 0.27 | ||||||
Abbreviations: 95% CI, 95% confidence intervals; VIF, variance inflation factors; LST, lean soft tissue; DXA, dual x-ray absorptiometry; % PMS, percentage of attained predicted mature stature.
*ln (lower limbs LSTDXA) = k 1 × ln (body mass) +k 2 × ln (leg length) +k 3 × ln (mid-thigh circumference) +k 4 × ln (anterior mid-thigh skinfold) +k 5 × ln (medial calf skinfold) +a+b × (% PMS) +ln ε.
Equation (2) (new model) was validated using PRESS statistics (Table 3). The high R 2 (0.90) and low SEE (0.27) emphasize the accuracy of the model.
Deming repression analysis between predicted and measured lower limbs LST showed that the new model had an R 2 = 0.91 and a Sy·x of 0.52 kg (Figure 2, panel a). The intercept (−0.62, 95% CI −1.40 to 0.17) and slope (1.04, 95% CI 0.96 to 1.11) of the equation did not significantly differ (p>0.05) from the identity line (i.e., y-intercept = 0 when x = 0 and slope = 1). Therefore, the possibility of systematic or proportional bias was rejected [51]. The relation between residuals and predicted lower limbs LST values is illustrated in Figure 2 (panel b). No significant mean differences between predicted and measured values and small limits of agreement were found (bias ±1.96 SD = −0.25±1.02 kg, p>0.05). The measurement differences (error) relative to predicted lower limbs LST were homoscedastic [46], [47], which was confirmed by the correlation (r = 0.09, p = 0.398) between the absolute differences and the predicted lower limbs LST values [52].
Figure 2. Deming regression analysis between the new anthropometric model (NM) and lower limbs lean soft tissue (LST) measured by dual-energy X-ray absorptiometry (panel a).

The reference line from the equation, standard error of estimation (Sy ·x), correlation (r) and coefficient of determination (R2), are also presented. The right panel (panel b) illustrate the relation between residuals (mean differences between lower limbs LST measured by DXA and predicted by the derived equation) and lower limbs LSTNM (heteroscedasticity diagnostic). The dashed lines represent 95% limits of agreement (±1.96 SD).
Discussion
The data detailed total body and segmental (lower limbs) LST in healthy circumpubertal boys in the context of developing and cross-validating a model that included anthropometric dimensions and a non-invasive estimate of maturity status among predictors of lower limbs LST relative to DXA as the reference method. Allometric modeling identified biological maturity status, anterior mid-thigh and medial calf skinfolds, mid-thigh circumference, leg length and body mass among significant predictors of lower limbs LST. The new model showed was valid and non-biased, and accurately predicted lower limbs LST as evident in a nearly perfect correlation between the new model and DXA, an intercept and slope that did not differ from the identity line, small limits of agreement, and errors independent of the magnitude of the values. The equation also had a high R 2 PRESS and low SEEPRESS. To our knowledge, this is the first study that obtained and cross-validated an equation to estimate lower limbs LST based on anthropometry and estimated maturity status in circumpubertal boys.
Appendicular skeletal muscle mass can be obtained from DXA [25], [53]–[55] by assuming that all non-bone and non-fat tissue is muscle mass [19]. This assumption is likely to be valid in the legs [56], [57] and is most likely to be valid at the regions between the joints such as the mid-thigh and the calf, where the amount of tendons and cartilage is small [20]. Nearly perfect correlations (r = 0.98–0.99) between appendicular LST assessed by DXA and skeletal muscle mass determined by MRI were noted in a multi-ethnic adolescents and children, consistent with these assumptions [58]. Total body LST of the present sample of boys 11.0±0.5 years was less (29.0±4.2 kg) than that of young boys 13.7±3.0 years (38.1±12.7 kg) [59], reflecting age and body size variation (stature: 144.8±6.4 kg vs. 158.1±17.7 cm; body mass: 40.2±9.0 kg vs. 50.2±17.4 kg, respectively).
DXA measurements of LST, body fat and bone mineral content were made independently, each with potential measurement error. In the present sample, the difference between whole body DXA mass and scale mass was 0.4 kg (0.9%). Although hydration was not controlled, minimal effects are expected since it has been shown that a subtraction or addition to the Reference Man of 1 kg in extracellular fluid would result in roughly a 0.6% over- or underestimation to total body fat mass using DXA [60]. Errors in the lower limbs LST prediction equation may be attributed in part to the use of skinfolds as predictor variables. The use of skinfold thickness measurements to estimate human body composition is based on two assumptions [61]: the thickness of the subcutaneous adipose tissue reflects a constant proportion of total body fat, and that the sites selected for measurement represent the average thickness of the subcutaneous adipose. Neither assumption, however, has been shown to be consistently generalized [62]. Skinfolds were performed by a single experienced observer following standard procedures [29], in the present study, and intra-observer technical errors of measurement (∼0.7 mm) and coefficients of variation (3.7–4.7%) were small [26].
There is no direct measure of leg length [63]. Jones and Pearson [22] measured leg as the length from the ground to the gluteal furrow. In the present study, leg length was estimated as the difference between stature and sitting height. In the DXA protocol, the leg length was defined as the mass of tissue distal to an oblique line passing through the neck of the femur, excluding gluteal muscles.
Leg circumferences were identified as suitable predictor variables. Although the correlation between stature × CC m-t 2 with lower limbs LSTDXA was relatively high (r = 0.72, p<0.001), the interaction term was not a significant predictor of lower limbs LSTNM. On the other hand, two studies [25], [31] suggested that the square of each corrected muscle girth multiplied by stature is the anthropometric parameter that contributed most to appendicular LST and skeletal muscle mass variance. The discrepancy among results and contribution of corrected muscle circumferences and stature (components of the cylinder's dimensions of the skeletal muscle mass of the human body) may be due to the considerably larger appendicular LST of young athletes [25] and non-obese adults [31] compared to this circumpubertal sample.
The adolescent growth spurt in stature starts, on average, at about 10–11 years of age in boys and reaches peak velocity (age at peak height velocity, PHV) at about 14 years [27]. Predicted time from PHV (erroneously labeled PHV), based on sex-specific anthropometric equations [64], was a significant predictor of total body LST in boys 8–18 years of age [59]. Note, however, predicted years from PHV and in turn age at PHV in boys is dependent on CA at prediction and actual age at PHV in an independent longitudinal sample of boys followed from 8 to 18 years; predicted age at PHV also has a reduced range of variation compared to actual age at PHV [65]. Identical results have been reported for an independent longitudinal sample of girls, highlighting the limitations of the prediction protocol [66]. Given the confounding effect of CA per se on the estimate of maturity timing, it is likely the effect attributed to years from PHV is due largely to CA.
Sexual maturation, based on a five stage scale using the criteria described by Tanner [67], have been considered in studies of skeletal muscle mass in boys 5–17 years [58] and appendicular LST in adolescent athletes 14–17 years [25]. Stages of secondary sex characteristics, though valuable, have limitations analytically. They indicate stage at the time of observation and do not indicate when the stage was entered or how long the individual has been in a stage. Moreover, stages of pubic hair and genital development in boys (or pubic hair and breast stages in girls) are not equivalent [27]. The present study used a non-invasive indicator of maturity status, percentage of predicted mature (adult) stature (% PMS) attained at the time of observation. Results indicated a significant and positive contribution of individual differences in % PMS to the prediction of lower limbs LST.
Although advances in technology permit accurate assessments of segmental tissue mass in vivo, assessments are limited largely to clinical or laboratory settings and are expensive. There is an interest for methods that provide information in a safe, cost-effective and non-invasive manner, and in a non-laboratory setting. The present study offers an equation that compares favorably with those reported in the literature for similar purposes [6], [25], [26], [31], [68]. No significant mean differences between measured and predicted lower limbs LST were observed, and the robustness of the model was not compromised by multicollinearity between independent variables. Tolerance (0.22–0.54) and a variance inflation factors (1.85–4.57) were well within the normal ranges (>0.10, <10, respectively) [39]. The adopted method of cross-validation [40] confirmed the effectiveness of the model to predict lower limbs LST with a high internal validity (R 2 PRESS = 0.90) and low proportional errors of estimation (SEEPRESS = 0.27). The PRESS method avoids data-splitting difficulties and provides similar unbiased estimates of future prediction equation performance.
It was deemed important to maintain an appropriate participant-to-variable ratio. In multiple regressions, that ratio was recommended to be higher than 5∶1 and preferably 20∶1 [69]. The present ratio was ∼13∶1. Moreover, it is established that PRESS statistics usually generates less confident estimates of an equation's potential [40]. The least products regression (Deming regression), where random errors in both dependent and independent variables are accommodated in the regression model [42], was used as an alternative to the ordinary least squares method. The new model (R 2 = 0.91 and a Sy·x of 0.52 kg) did not presented systematic or proportional bias as the equation did not differ significantly from the identity line [51]. Lastly, the measurement differences (error) against the predicted lower limbs LST values were homoscedastic (r = 0.09, p = 0.398) [46], [47], allowing the use of this equation with constant error variance.
Although the current investigation has a number of strengths (e.g., objective measures, analytical procedures), it is not without limitations. First, the method for estimating maturity status was non-invasive, but the prediction equation was based on middle socio-economic class American youth of White/European ancestry in the Fels Longitudinal Study [32]. Validation of the equations in Portuguese youth is needed. Second, the study was limited to a cross-sectional sample of healthy circumpubertal Portuguese boys 10–13 years of age and prediction equations tend to be age and population specific. Additional validation studies are needed to critically validate this model in other samples (e.g., mid- and late-adolescents, youth of other ethnic groups, or specific populations with varying anthropometric characteristics).
Conclusions
In summary, a new model derived from anthropometric variables and maturity status was proposed for assessing lower limbs LST in research dealing with circumpubertal boys. The equation was satisfactorily cross-validated at group and individual basis, ensuring its applicability to similar samples. However, it is important to note that when an equation is applied to groups the associated errors will be always smaller than those for individuals. This equation will allow accurate lower limbs-specific mass information, thus offering a valid alternative to scan participants with technologies such as DXA.
Acknowledgments
The authors gratefully acknowledge the effort of the participants and their parents. The early contribution of Filipe Simões († 2013) in the current project is remembered.
Data Availability
The authors confirm that, for approved reasons, some access restrictions apply to the data underlying the findings. Data underlying the findings of the present study are available upon request. Data are from the project PTDC/DTP-DES/1178/2012, which is protected by ethical and legal restrictions of the Portuguese Government (Foundation for Science and Technology). Data are from the Exercise and Health Laboratory and are considered available for researchers who meet the criteria to access confidential data. The Head of the unit is Luís Bettencourt Sardinha and may be contacted at lsardinha@fmh.utl.pt.
Funding Statement
Authors were partially supported by the Portuguese Foundation for Science and Technology (SFRH/BD/64648/2009; PTDC/DTP-DES/1178/2012) and CAPES (BEX0951/10-2). No other current funding sources for this study. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Davies CT, Barnes C, Godfrey S (1972) Body composition and maximal exercise performance in children. Hum Biol 44: 195–214. [PubMed] [Google Scholar]
- 2. Docherty D, Gaul CA (1991) Relationship of body size, physique, and composition to physical performance in young boys and girls. Int J Sports Med 12: 525–532. [DOI] [PubMed] [Google Scholar]
- 3. Tolfrey K, Barker A, Thom JM, Morse CI, Narici MV, et al. (2006) Scaling of maximal oxygen uptake by lower leg muscle volume in boys and men. J Appl Physiol 100: 1851–1856. [DOI] [PubMed] [Google Scholar]
- 4. Valente-Dos-Santos J, Sherar L, Coelho-e-Silva MJ, Pereira JR, Vaz V, et al. (2013) Allometric scaling of peak oxygen uptake in male roller hockey players under 17 years old. Appl Physiol Nutr Metab 38: 390–395. [DOI] [PubMed] [Google Scholar]
- 5. Van Praagh E, Fellmann N, Bedu M, Falgairette G, Coudert J (1990) Gender difference in the relationship of anaerobic power output to body composition in children. Pediatr Exerc Sci 2: 336–348. [DOI] [PubMed] [Google Scholar]
- 6. Welsman JR, Armstrong N, Kirby BJ, Winsley RJ, Parsons G, et al. (1997) Exercise performance and magnetic resonance imaging-determined thigh muscle volume in children. Eur J Appl Physiol O 76: 92–97. [DOI] [PubMed] [Google Scholar]
- 7. Armstrong N (2013) Aerobic fitness and physical activity in children. Pediatr Exerc Sci 25: 548–560. [DOI] [PubMed] [Google Scholar]
- 8. Kemper HC, Twisk JW, Van Mechelen W (2013) Changes in aerobic fitness in boys and girls over a period of 25 years: data from the Amsterdam Growth and Health Longitudinal Study revisited and extended. Pediatr Exerc Sci 25: 524–535. [DOI] [PubMed] [Google Scholar]
- 9.Scammon RE (1923) A summary of the anatomy of the infant and child. In: Abt IA, editor. Pediatrics. Philadelphia: Saunders. 257–444.
- 10.Malina RM (1996) Regional body composition: age, sex, and ethnic variation. In: Roche AF, Heymsfield SB, Lohman TG, editors. Human body composition. Champaign, IL: Human Kinetics. 217–255.
- 11. Lee SY, Gallagher D (2008) Assessment methods in human body composition. Curr Opin Clin Nutr Metab Care 11: 566–572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Lee RC, Wang ZM, Heymsfield SB (2001) Skeletal muscle mass and aging: regional and whole-body measurement methods. Can J Appl Physiol 26: 102–122. [DOI] [PubMed] [Google Scholar]
- 13. Wang Z, Zhu S, Wang J, Pierson RN, Heymsfield SB (2003) Whole-body skeletal muscle mass: development and validation of total-body potassium prediction models. Am J Clin Nutr 77: 76–82. [DOI] [PubMed] [Google Scholar]
- 14. Salinari S, Bertuzzi A, Mingrone G, Capristo E, Pietrobelli A, et al. (2002) New bioimpedance model accurately predicts lower limb muscle volume: validation by magnetic resonance imaging. Am J Physiol Endocrinol Metab 282: E960–966. [DOI] [PubMed] [Google Scholar]
- 15. Wells JC, Fuller NJ, Dewit O, Fewtrell MS, Elia M, et al. (1999) Four-component model of body composition in children: density and hydration of fat-free mass and comparison with simpler models. Am J Clin Nutr 69: 904–912. [DOI] [PubMed] [Google Scholar]
- 16. Lohman TG (1986) Applicability of body composition techniques and constants for children and youths. Exerc Sport Sci Rev 14: 325–357. [PubMed] [Google Scholar]
- 17. Wells JC, Williams JE, Chomtho S, Darch T, Grijalva-Eternod C, et al. (2010) Pediatric reference data for lean tissue properties: density and hydration from age 5 to 20 y. Am J Clin Nutr 91: 610–618. [DOI] [PubMed] [Google Scholar]
- 18. Goran MI (1998) Measurement issues related to studies of childhood obesity: assessment of body composition, body fat distribution, physical activity, and food intake. Pediatrics 101: 505–518. [PubMed] [Google Scholar]
- 19. Heymsfield SB, Smith R, Aulet M, Bensen B, Lichtman S, et al. (1990) Appendicular skeletal muscle mass: measurement by dual-photon absorptiometry. Am J Clin Nutr 52: 214–218. [DOI] [PubMed] [Google Scholar]
- 20. Visser M, Fuerst T, Lang T, Salamone L, Harris TB (1999) Validity of fan-beam dual-energy X-ray absorptiometry for measuring fat-free mass and leg muscle mass. Health, aging, and body composition study-dual-energy x-ray absorptiometry and body composition working group. J Appl Physiol 87: 1513–1520. [DOI] [PubMed] [Google Scholar]
- 21. Wang ZM, Visser M, Ma R, Baumgartner RN, Kotler D, et al. (1996) Skeletal muscle mass: evaluation of neutron activation and dual-energy X-ray absorptiometry methods. J Appl Physiol 80: 824–831. [DOI] [PubMed] [Google Scholar]
- 22. Jones PR, Pearson J (1969) Anthropometric determination of leg fat and muscle plus bone volumes in young male and female adults. J Physiol 204: 63–66. [PubMed] [Google Scholar]
- 23. Dore E, Bedu M, Franca NM, Van Praagh E (2001) Anaerobic cycling performance characteristics in prepubescent, adolescent and young adult females. Eur J Appl Physiol 84: 476–481. [DOI] [PubMed] [Google Scholar]
- 24. Martin RJ, Dore E, Twisk J, van Praagh E, Hautier CA, et al. (2004) Longitudinal changes of maximal short-term peak power in girls and boys during growth. Med Sci Sport Exer 36: 498–503. [DOI] [PubMed] [Google Scholar]
- 25. Quiterio AL, Carnero EA, Silva AM, Bright BC, Sardinha LB (2009) Anthropometric models to predict appendicular lean soft tissue in adolescent athletes. Med Sci Sport Exer 41: 828–836. [DOI] [PubMed] [Google Scholar]
- 26. Coelho-e-Silva MJ, Malina RM, Simoes F, Valente-Dos-Santos J, Martins RA, et al. (2013) Determination of thigh volume in youth with anthropometry and DXA: Agreement between estimates. Eur J Appl Physiol 13: 527–533. [DOI] [PubMed] [Google Scholar]
- 27.Malina R, Bouchard C, Bar-Or O (2004) Growth, maturation, and physical activity. Champaign, IL: Human Kinetics. 728.
- 28. World Medical Association (2008) Declaration of Helsinki: ethical principles for medical research involving human subjects. WMJ 54: 122–125. [Google Scholar]
- 29.Lohman TG, Roche AF, Martorell R (1988) Anthropometric standardization reference manual. Champaign, IL: Human Kinetics. 177.
- 30.Malina RM (1995) Anthropometry. In: Maud PJ, Foster C, editors. Physiological assessment of human fitness. Champaign, IL: Human Kinetics. 205–219.
- 31. Lee RC, Wang Z, Heo M, Ross R, Janssen I, et al. (2000) Total-body skeletal muscle mass: development and cross-validation of anthropometric prediction models. Am J Clin Nutr 72: 796–803. [DOI] [PubMed] [Google Scholar]
- 32. Khamis HJ, Roche AF (1994) Predicting adult stature without using skeletal age: the Khamis-Roche method. Pediatrics 94: 504–507. [PubMed] [Google Scholar]
- 33. Malina RM, Coelho-E-Silva MJ, Figueiredo AJ, Carling C, Beunen GP (2012) Interrelationships among invasive and non-invasive indicators of biological maturation in adolescent male soccer players. J Sports Sci 30: 1705–1717. [DOI] [PubMed] [Google Scholar]
- 34. Padez C (2003) Secular trend in stature in the Portuguese population (1904–2000). Ann Hum Biol 30: 262–278. [DOI] [PubMed] [Google Scholar]
- 35. Bielicki T, Koniarek J, Malina RM (1984) Interrelationships among certain measures of growth and maturation rate in boys during adolescence. Ann Hum Biol 11: 201–210. [DOI] [PubMed] [Google Scholar]
- 36. Malina RM, Dompier TP, Powell JW, Barron MJ, Moore MT (2007) Validation of a noninvasive maturity estimate relative to skeletal age in youth football players. Clin J Sport Med 17: 362–368. [DOI] [PubMed] [Google Scholar]
- 37. Bayley N, Pinneau SR (1952) Tables for predicting adult height from skeletal age: revised for use with the Greulich-Pyle hand standards. Journal Pediatr 40: 423–441. [DOI] [PubMed] [Google Scholar]
- 38. Nevill A, Holder R (1994) Modelling maximum oxygen uptake: a case study in non-linear regression model formulation and comparison. J Roy Statistical Society 43: 653–666. [Google Scholar]
- 39. Slinker BK, Glantz SA (1985) Multiple regression for physiological data analysis: the problem of multicollinearity. Am J Physiol 249: R1–12. [DOI] [PubMed] [Google Scholar]
- 40. Holiday DB, Ballard JE, McKeown BC (1995) PRESS-related statistics: regression tools for cross-validation and case diagnostics. Med Sci Sport Exer 27: 612–620. [PubMed] [Google Scholar]
- 41. Hinkley DV (1977) Jackknifing in unbalanced situations. Technometrics 19: 285–292. [Google Scholar]
- 42. Ricker WE (1973) Linear regressions in fishery research. J Fish Res Board Can 30: 409–434. [Google Scholar]
- 43. Bland JM, Altman DG (2012) Agreed statistics: measurement method comparison. Anesthesiology 116: 182–185. [DOI] [PubMed] [Google Scholar]
- 44. Hopkins WG (2004) Bias in Bland-Altman but not regression validity analysis. Sportscience 8: 42–46. [Google Scholar]
- 45. Evans EM, Rowe DA, Misic MM, Prior BM, Arngrimsson SA (2005) Skinfold prediction equation for athletes developed using a four-component model. Med Sci Sports Exerc 37: 2006–2011. [DOI] [PubMed] [Google Scholar]
- 46. Batterham AM, George KP, Mullineaux DR (1997) Allometric scaling of left ventricular mass by body dimensions in males and females. Med Sci Sport Exer 29: 181–186. [DOI] [PubMed] [Google Scholar]
- 47. Nevill AM, Ramsbottom R, Williams C (1992) Scaling physiological measurements for individuals of different body size. Eur J Appl Physiol O 65: 110–117. [DOI] [PubMed] [Google Scholar]
- 48. Hopkins WG, Marshall SW, Batterham AM, Hanin J (2009) Progressive statistics for studies in sports medicine and exercise science. Med Sci Sport Exer 41: 3–13. [DOI] [PubMed] [Google Scholar]
- 49. Roche AF, Tyleshevski F, Rogers E (1983) Non-invasive measurement of physical maturity in children. Res Q Exerc Sport 54: 364–361. [Google Scholar]
- 50. Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM, Mei Z, et al. (2002) 2000 CDC growth charts for the United States: methods and development. Vital Health Stat 11: 1–186. [PubMed] [Google Scholar]
- 51. Ludbrook J (2002) Statistical techniques for comparing measurers and methods of measurement: a critical review. Clin Exp Pharmacol Physiol 29: 527–536. [DOI] [PubMed] [Google Scholar]
- 52. Nevill AM, Atkinson G (1997) Assessing agreement between measurements recorded on a ratio scale in sports medicine and sports science. Br J Sports Med 31: 314–318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Ellis KJ (2000) Human body composition: in vivo methods. Physiol Rev 80: 649–680. [DOI] [PubMed] [Google Scholar]
- 54. Kulkarni B, Kuper H, Taylor A, Wells JC, Radhakrishna KV, et al. (2013) Development and validation of anthropometric prediction equations for estimation of lean body mass and appendicular lean soft tissue in Indian men and women. J Appl Physiol 115: 1156–1162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Leahy S, O'Neill C, Sohun R, Jakeman P (2012) A comparison of dual energy X-ray absorptiometry and bioelectrical impedance analysis to measure total and segmental body composition in healthy young adults. Eur J Appl Physiol 112: 589–595. [DOI] [PubMed] [Google Scholar]
- 56. Heymsfield SB, Wang Z, Baumgartner RN, Ross R (1997) Human body composition: advances in models and methods. Annu Rev Nutr 17: 527–558. [DOI] [PubMed] [Google Scholar]
- 57.Snyder WS, Cook MJ, Nasset ES, Karhausen RL, Howells GP, et al. (1975) Report of the Task Group on reference man. ICRP Publication 23. Oxford: Pergamon Press. 40–45.
- 58. Kim J, Shen W, Gallagher D, Jones A, Wang Z, et al. (2006) Total-body skeletal muscle mass: estimation by dual-energy X-ray absorptiometry in children and adolescents. Am J Clin Nutr 84: 1014–1020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Machado D, Oikawa S, Barbanti V (2013) The multicomponent anthropometric model for assessing body composition in a male pediatric population: a simultaneous prediction of fat mass, bone mineral content, and lean soft tissue. J Obes 2013: e428135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Pietrobelli A, Formica C, Wang Z, Heymsfield SB (1996) Dual-energy X-ray absorptiometry body composition model: review of physical concepts. Am J Physiol 271: E941–951. [DOI] [PubMed] [Google Scholar]
- 61. Holmes JD, Andrews DM, Durkin JL, Dowling JJ (2005) Predicting in vivo soft tissue masses of the lower extremity using segment anthropometric measures and DXA. J Appl Biomech 21: 371–382. [DOI] [PubMed] [Google Scholar]
- 62. Lukaski HC (1987) Methods for the assessment of human body composition: traditional and new. Am J Clin Nutr 46: 537–556. [DOI] [PubMed] [Google Scholar]
- 63.Martin AD, Carter JE, Hendy KC, Malina RM (1998) Segment lengths. In: Lohman TG, Roche AF, Martorell R, editors. Anthropometric standardization reference manual. Champaign, IL: Human Kinetics. pp. 9–26.
- 64. Mirwald RL, Baxter-Jones AD, Bailey DA, Beunen GP (2002) An assessment of maturity from anthropometric measurements. Med Sci Sports Exerc 34: 689–694. [DOI] [PubMed] [Google Scholar]
- 65. Malina RM, Kozieł SM (2014) Validation of maturity offset in a longitudinal sample of Polish boys. J Sports Sci 32: 424–437. [DOI] [PubMed] [Google Scholar]
- 66.Malina RM, Kozieł SM (2014) Validation of maturity offset in a longitudinal sample of Polish girls. J Sports Sci. Doi: 10.1080/02640414.2014.889846 [DOI] [PubMed]
- 67.Tanner JM (1962) Growth at adolescence. Oxford: Blackwell. 325.
- 68. Fuller NJ, Fewtrell MS, Dewit O, Elia M, Wells JC (2002) Segmental bioelectrical impedance analysis in children aged 8–12 y: The assessment of regional body composition and muscle mass. Int J Obes Relat Metab Disord 26: 692–700. [DOI] [PubMed] [Google Scholar]
- 69.Vincent WJ (2005) Statistics in Kinesiology. Champaign, IL: Human Kinetics. 511.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The authors confirm that, for approved reasons, some access restrictions apply to the data underlying the findings. Data underlying the findings of the present study are available upon request. Data are from the project PTDC/DTP-DES/1178/2012, which is protected by ethical and legal restrictions of the Portuguese Government (Foundation for Science and Technology). Data are from the Exercise and Health Laboratory and are considered available for researchers who meet the criteria to access confidential data. The Head of the unit is Luís Bettencourt Sardinha and may be contacted at lsardinha@fmh.utl.pt.