

Abstract
This study explored the relationship of the subjective socioeconomic position (SEP) as well as the objective SEP with the rate of suicide attempts in 74,186 adolescents from the 2012 Korea Youth Risk Behavior Web-based Survey (KYRBS). The SEP was measured by the Family Affluence Scale (FAS) and the self-rated household economic status. The low perceived SEP for either the high or low FAS score was related to the elevated likelihood of suicide attempts in both genders. As compared with the adolescents in both the high level of perceived SEP and FAS score after adjusting for other confounding factors, the middle school students were more likely to attempt suicide in both low level of perceived SEP and FAS score (OR, 1.81; 95% CI, 1.18-2.78 for boys, OR, 1.46; 95% CI, 1.13-1.90 for girls). The high school students were more likely to attempt suicide in the low perceived SEP and high FAS score (OR, 1.44; 95% CI, 1.14-1.81 for boys, OR, 1.29; 95% CI, 1.07-1.56 for girls). In conclusion, the relationship of subjective SEP is important in suicide attempts as much as objective SEP and far more important in the high school students.
Keywords: Socioeconomic Position, Attempted Suicide, Adolescent
INTRODUCTION
Korea has the highest suicide rate among the Organization of Economic Co-operation and Development (OECD) countries, which is at a rate higher than 2.5 times the OECD average (1). Furthermore, Korea has experienced a sharp increase in the suicides of 280.7% in the last two decades, which contrasts with the general tendency toward a decline in other OECD countries, averaging -7.89% (1).
The probability of death resulting from a suicidal act is 100 times higher in the attempters than in the general population (2). The suicide attempts in adolescence, in particular, have been suggested to be important indicators of suicide in adulthood (3). Therefore, the timely identification of the risk factors for the adolescents which are associated with suicide attempts could contribute to reduce the risk of suicide effectively (4, 5).
A large number of factors possibly influencing suicidal behaviors in adolescents have been identified, including the psychosocial factors, individual health behaviors, and socioeconomic factors (4, 6, 7). Among these factors, the effect of the socioeconomic position (SEP) is currently controversial (8, 9, 10). Although some studies have found that the risk of suicide attempts generally increased with the lower SEP in adolescence (11, 12), the results are varying and even reversed (8, 9, 10). The inconsistent results may be explained by a selection bias due to study subjects with skewed social class attending the hospital as results of suicide attempts (13). As another possibility, the inconsistencies may be partly related to the difficulties in measuring SEP among adolescents (14). As reported, most adolescents may not be able to answer the classical SEP indicators including the parents' occupations, education level, and income (15). To address the difficulty, the Family Affluence Scale (FAS), which is composed of questions on the family material circumstances to which the adolescents are almost certain to know the answers, has been developed and validated in several studies (15).
In addition, some researchers have suggested the SEP differences in youth are negligible when using the objective indicators, including education and income. As adolescents may be less aware of the parental social stratification, the perceived SEP may better reflect how the adolescents actually see their economic circumstances (16, 17). However, the studies exploring the association between the health and perceived SEP have mostly been focused on the adult populations or selected outcomes in adolescents, such as the self-rated health, depressive, and psychosomatic symptoms (15, 17, 18).
Therefore, this study was conducted to identify the relationship of SEP and suicide attempts using both the subjective and objective measures of SEP in the Korean adolescents.
MATERIALS AND METHODS
Study subjects
The subjects were participants in the 2012 Korea Youth Risk Behavior Web-based Survey (KYRBS). The survey has been conducted annually since 2005 by the Korea Centers for Disease Control and Prevention (KCDC) and the Ministry of Education, Science and Technology, in order to monitor the prevalence of the health behaviors among the adolescents. It aims to progress toward the national health objectives with the planning and assessment of the adolescent health promotion policies. The data was collected with an ongoing, web-based survey conducted on a nationally representative sample of middle and high school students with a stratified, clustered, multistage probability sampling design. The survey protected for the privacy and allowed anonymous participation. The students provided written consent for the survey and responded electronically to a questionnaire related to the health behaviors via a computerized program during classroom time (19). The response rate of participants was 96.4% and the reliability and validity of KYRBS have been shown to be good (19, 20). The number of study subjects was 74,186 who were aged between 12 and 18 yr old (38,221 for boys and 35,965 girls).
Variables
The SEP for the adolescents in this study was measured by two indicators. As an objective measure of SEP, the Family Affluence Scale (FAS) was used. The FAS has been developed and used in the European countries as a good predictor of the socioeconomic differentials in health (21). A recent study showed that the FAS appeared to be useful as a measure of SEP for the Korean adolescents (15). The scale consists of four items: 1) Does your family have a car? (no, one, two or more); 2) Do you have your own room? (no, yes); 3) During the past year, how many times did you travel away on holiday with your family? (not at all, once, twice, three times or more); and 4) How many computers do you have in your household? (none, one, two, three or more). Each item was given a score of 0 if the answer was no or not at all; 1 if the answer was yes, one, or once; 2 if the answer was two or more, twice or two; and 3 for the rest of the responses. The composite FAS score was calculated by summing the responses to these four items and the scores were then grouped as low (score of 0-2), middle (score of 3-5), and high (score of 6-9) (22). For the further analysis, the subjects with the low scores of SEP were classified into the low SEP group and others (middle and high) were grouped as the high SEP group. Another indicator reflecting a subjective measure of the adolescent's SEP was assessed to respond to the question, "What do you perceive as your household economic status?" This perceived household economic status was asked on a 5-item scale: highest level, above average, average, below average, and lowest level. The subjects who responded "below average and lowest level" were classified into the low perceived SEP group and others were included in the high perceived SEP group. The four combination groups of the SEP based on the FAS and perceived SEP was created to examine the relationship between their combination pattern and suicide attempts; 1) high perceived SEP and high FAS, 2) high perceived SEP and low FAS, 3) low perceived SEP and high FAS, 4) low perceived SEP and low FAS.
In order to examine the suicide attempts, the subjects were asked to respond in a yes or no fashion to the questions "During the last 12 months, have you attempted suicide?" The psychological health status indicators, such as the stress perception and depression symptom were also examined. The subjects who responded to perceive "very much" or "much" stress were classified into a group with stress. The depression symptoms were assessed by a response in a yes or no fashion to the question "Were you feeling so sad or hopeless for at least two weeks or more that you stopped doing some usual activities during the last 12 months?" The information of the health behaviors including tobacco use, alcohol consumption, drug use and sexual relationship were collected. Subjects who had smoked at least one cigarette or consumed alcohol one or more days during the past 30 days were categorized into the current cigarette smoking or alcohol drinking group, respectively. The drug use and sexual relationship were examined, by asking whether the subjects had experienced any of these at least once.
Statistical analyses
Because the KYRBS was designed as a complex sample, the relevant primary sampling units, stratification, and sample weights were taken into account in the data analysis. The proportion of the general characteristics of the subjects was weighted to the respondent's probability of being selected for the sex-, grade-, and school type-specific distributions for the region, based on the education statistics from the Ministry of Education, Science and Technology. We combined the SEP based on the FAS and perceived SEP to examine the relationship between their combination pattern and factors related to SEP including the suicide attempts. The relationship was assessed by chi-square tests. Then, multivariate-adjusted odds ratios (ORs) and the 95% confidence intervals (95% CIs) were calculated to examine the effect of the FAS, perceived SEP and the combination pattern of SEP on the suicide attempts by logistic regression analysis. The analyses were conducted separately for sex and school grade. All analyses were done using SAS version 9.2 (SAS Inc., Cary, NC, USA).
Ethics statement
The requirement for the ethics approval for the use of the publicly available KYRBS data was waived by the institutional review board (IRB). The students were informed about the purpose of the research, provided written informed consent, and were assured of the right to refuse to participate or to withdraw from the study at any stage (19). Anonymity and confidentiality were guaranteed.
RESULTS
The general characteristics of the study population are shown in Table 1. The proportion of boys was 52.5%, and about half of the subjects were middle school students. In general, the prevalence of the health behaviors for the current cigarette smoking (16.3% of boys vs. 5.9% of girls, P<0.001), alcohol drinking (22.7% of boys vs. 15.8% of girls, P<0.001), and experience of sexual relationship (5.9% of boys vs. 2.6% of girls, P<0.001) was higher in boys than in girls. However, the psychological factors such as the stress perception (34.8% of boys vs. 49.6% of girls, P<0.001), depression symptom (25.5% of boys vs. 36.0% of girls, P<0.001), and suicide attempts (2.8% of boys vs. 5.4% of girls, P<0.001) were more prevalent in girls than in boys. Regarding the perceived economic status, girls showed a greater proportion of the low and mid-low status than boys (21.9% for boys vs. 23.3% for girls, P<0.001). The distribution of the SEP level measured by FAS was similar between sexes. The proportion of the adolescents with high FAS score was 35.8% for boys and 34.8% for girls, and those with low FAS score was 11.7% for boys and 11.8% for girls. The proportion of the adolescents with both the high level of FAS and perceived SEP was 72.3% for boys and 71.5% for girls. The proportion with the low levels in both the FAS and perceived SEP was 5.9% for boys and 6.7% for girls (P<0.001).
Table 1.
General characteristics of the study population
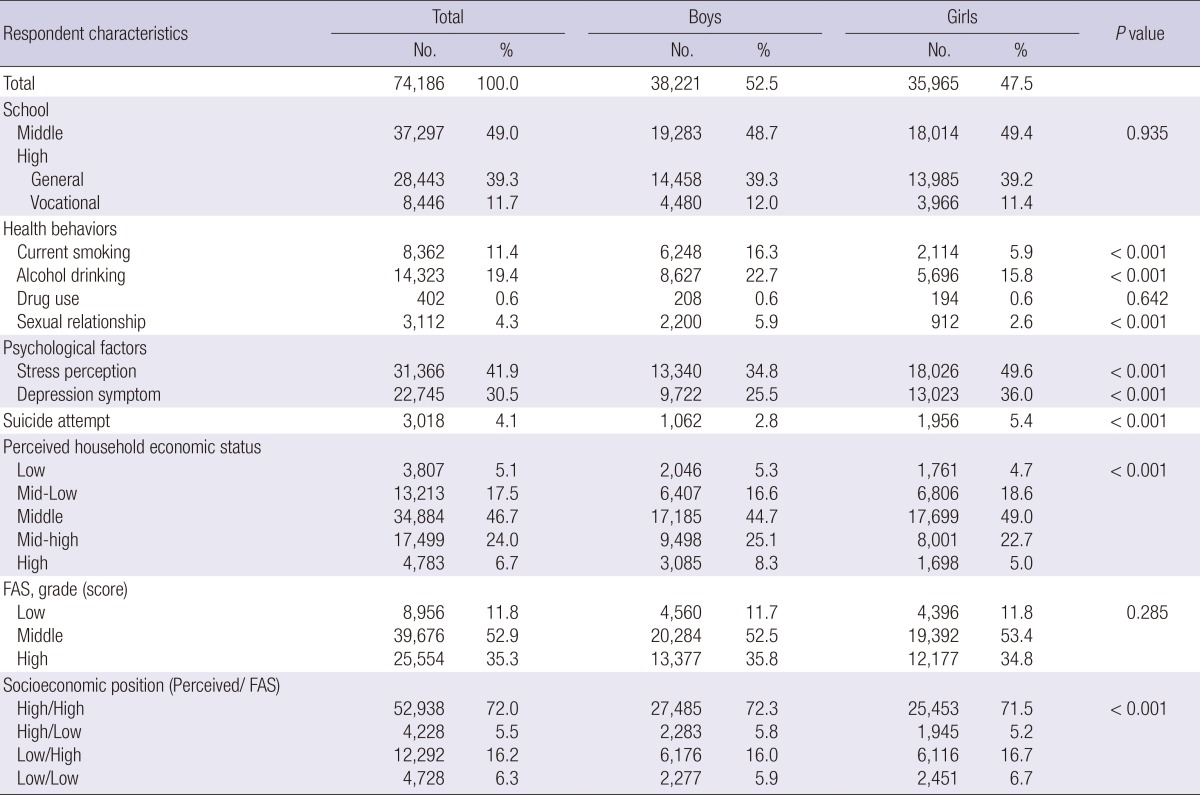
FAS, family affluence scale.
Table 2 shows the relationship between the combination pattern of the socioeconomic position measured by FAS, the perceived household economic status and other factors by gender and school grade. Regardless of the FAS score, adolescents with the low perceived SEP had more smoking, drinking, drug use, experience of sexual relationship, stress perception, and depression symptoms than those with the high perceived SEP, except in the drug use for the high school students. The results were consistent in gender and school grades. For the suicide attempts, adolescents with the low perceived SEP had a higher proportion than those with the high perceived SEP regardless of the FAS score in both boys and girls; and the proportion was higher in middle school students than high school students. Except for the boys in high school, adolescents with both the low perceived SEP and FAS grade had the highest proportion of suicide attempts, showing 5.8% for boys in the middle school, 11.3% for girls in the middle school, and 6.7% for girls in the high school. The boys in high school with the highest proportion of suicide attempts were the group with the low perceived SEP and high FAS score (3.9%).
Table 2.
The distribution of factors related to the combination pattern of socioeconomic position (measured by FAS and perceived household economic status) by gender and school grades
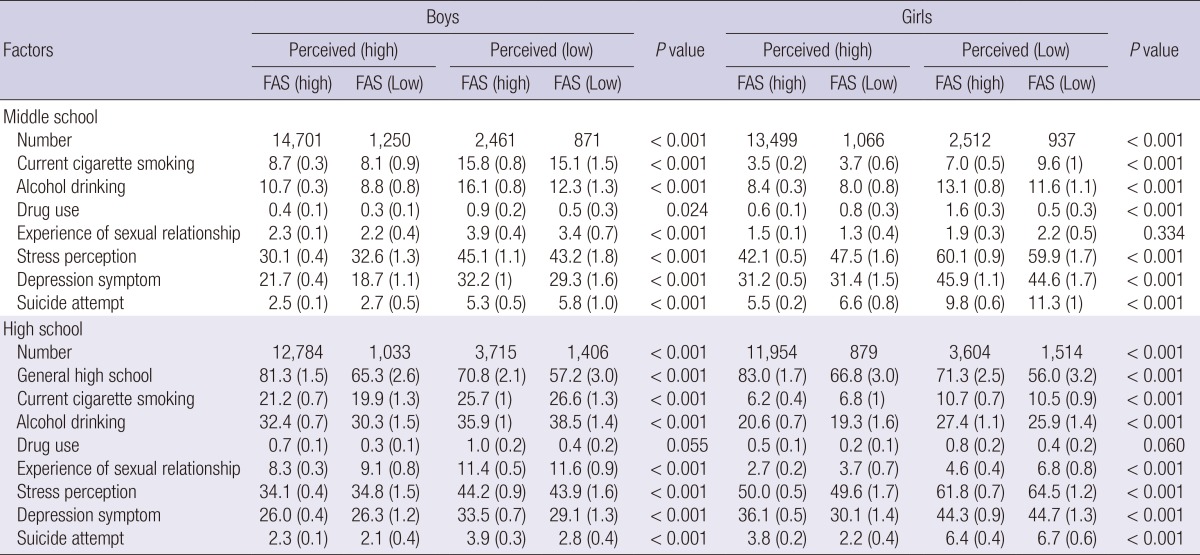
FAS, family affluence scale.
The independent and interaction effects of FAS and perceived SEP on suicide attempts are shown in Table 3. Among the middle school students, FAS was not related to the risk of suicide attempts (P=0.26 for total, P=0.60 for boys, P=0.18 for girls) but perceived SEP was significantly related to the increased risk (P<0.001 for total and boys, P=0.049 for girls) when each variable was simultaneously adjusted in the model. Regarding high school students, both FAS and perceived SEP influenced increased risk of suicide attempts (P=0.007 for FAS, P<0.001 for perceived SEP). In the gender analysis, both SEP variables significantly affected suicide attempts in boys (P=0.02 for FAS, P<0.001 for perceived SEP) but only the effect of perceived SEP was shown in girls (P=0.14 for FAS, P<0.001 for perceived SEP). The interaction effect of FAS and perceived SEP on suicide attempts was not shown.
Table 3.
The independent and interaction effects of family affluence scale (FAS) and perceived socioeconomic position (SEP) on suicide attempts
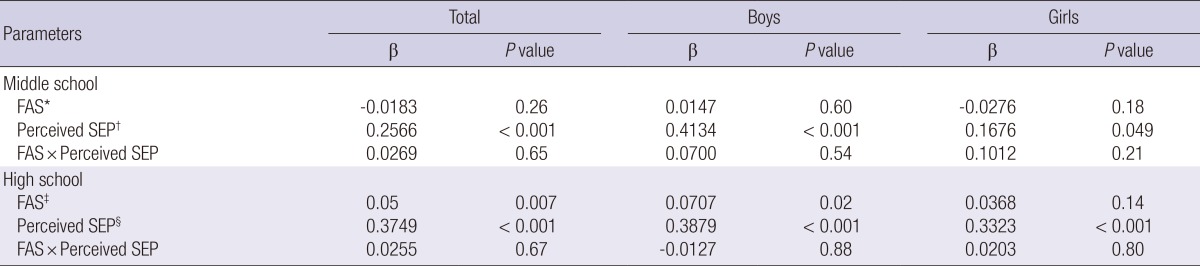
*Model was adjusted for age, smoking, drinking, drug use, experience of sexual relationship, stress perception, depression symptom, and perceived SEP; †Model was adjusted for age, smoking, drinking, drug use, experience of sexual relationship, stress perception, depression symptom, and FAS; ‡Model was adjusted for age, school type, smoking, drinking, drug use, experience of sexual relationship, stress perception, depression symptom, and perceived SEP; §Model was adjusted for age, school type, smoking, drinking, drug use, experience of sexual relationship, stress perception, depression symptom, and FAS.
Table 4 presents the multivariate-adjusted odds ratios (OR) and 95% confidence interval (95% CI) by logistic regression analysis describing the odds for suicide attempts by the combination pattern of SEP among boys and girls in the middle and high school. Overall, the low perceived SEP for either the high or low FAS score was related to the elevated likelihood of suicide attempts (OR, 1.26; 95% CI, 1.10-1.45 for low perceived SEP/high FAS and OR, 1.62; 95% CI, 1.30-2.02 for low perceived SEP/low FAS in the middle school, OR, 1.36; 95% CI, 1.17-1.59 for low perceived SEP/high FAS and OR, 1.27; 95% CI, 1.04-1.56 for low perceived SEP/low FAS in the high school). As compared with the adolescents in both the high level of perceived SEP and FAS score after adjusting for other confounding factors, the middle school students were more likely to attempt suicide in both the low level of perceived SEP and FAS score (OR, 1.81; 95% CI, 1.18-2.78 for boys, OR, 1.46; 95% CI, 1.13-1.90 for girls). The high school students were more likely to attempt suicide in the low perceived SEP and high FAS score (OR, 1.44; 95% CI, 1.14-1.81 for boys, OR, 1.29; 95% CI, 1.07-1.56 for girls).
Table 4.
The relationship between the combination pattern of socioeconomic position and suicide attempt (odds ratios and 95% confidence intervals)
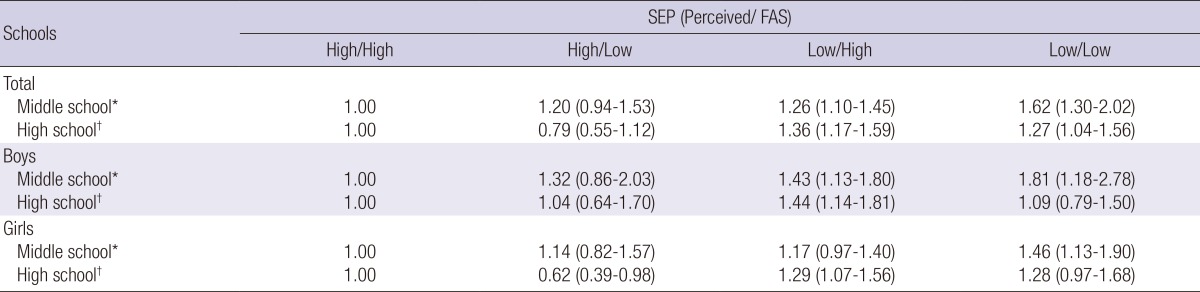
*Model was adjusted for age, smoking, drinking, drug use, experience of sexual relationship, stress perception, and depression symptom; †Model was adjusted for age, school type, smoking, drinking, drug use, experience of sexual relationship, stress perception, and depression symptom. FAS, family affluence scale; SEP, socioeconomic position.
DISCUSSION
This study suggests that the higher risks of suicide attempts were found in the Korean adolescents with the low level of both the subjective and objective SEP in the middle school and with the low subjective SEP and high objective SEP in the high school. Although the objective SEP itself is associated with the complete suicide or suicidal behaviors, the objective SEP ignores the personal perception of one's place in the society (16, 23). In youth, one's social status among peers may be of a greater importance to health than the parent's objective social status (24). While the subjective perception of the family economic circumstances was affected by the objective SEP measures, the influence from the objective SEP on the subjective perception may not be identical in young people (23). When we additionally analyzed the correlation between FAS and perceived SEP, correlation coefficient was 0.39 (P<0.001) and kappa index was 0.25, indicating weak positive correlation (data were not shown).
The lower perceived social status has been reported to be related with worse biomarkers, including the worse lipid profiles, central obesity, and glucose intolerance, all of which may activate the hypothalamus-pituitary-adrenal axis and the sympathetic nervous system (25). The subjective feelings of one's relative socioeconomic condition may induce the social inequalities in the morbidity and mortality rates in the later life, particularly when the lower levels of the self-assessment SEP are associated with the depressive symptoms as detected in the Hungarian adult study population (26). In this study, the risk of suicide attempts was generally elevated in the combination group of both the low level of perceived SEP and FAS score. However, among the high school students, it was only significant in those with the low perceived SEP and high FAS score. The review paper on the SEP and health in adolescence reported that some health behaviors in the early teens may be influenced by the family social status, as they spend most of their time with the family members. In late adolescence, however, the influence of friends and peers may eclipse the effects of the family SEP, which may help explain the relatively higher influence of the subjective SEP possibly being reflected by the influence of the friends' or peer's SEP (18).
The current study adds to the evidence that the elevated risk of attempted suicide related to SEP is higher among boys than girls (8). The line of evidence has suggested that the attempted suicides of men are more likely to be associated with income, while the attempted suicides of women are more associated with the educational attainment. This observation supports the hypothesis that men respond more strongly to the economic conditions than women in the development of the suicidal behavior (27, 28). As both the FAS and perceived SEP are related with income, which is more significant in men, the gender difference may be explained in this context.
To interpret the findings of this study accurately, there are several limitations that are worth noting. Firstly, the cross-sectional nature of this study does not allow for the inference of the causal relationship among the SEP and suicide attempts in adolescents. Secondly, this study is based on the self-reported data. However, self-reports have been suggested to provide more valid information than other methods on the sensitive issues, especially among the adolescent age groups (4). Thirdly, some variables including the subjective SEP and suicide attempts were measured by a single item rather than by a scale consisting of multiple items; this may have resulted in some reliability and validity problems. Nonetheless, the most recent previous studies focusing on the various racial and ethnic groups have used this self-reported single question method, and this trend has increased in the recent years (4).
Despite the limitations mentioned above, we are not aware of any previous study that has explored the relationship among both the subjective and objective SEP and suicide attempts in adolescents. In addition, this study targeted a large representative youth sample with a high response rate. We have also included the FAS, a relatively objective SEP in adolescence, and employed various psychological risk factors, such as the stress perception and depression symptoms.
In conclusion, the results of this study suggest that the relationship of the subjective SEP is important in suicide attempts as much as the objective SEP and far more important in the high school students. This information could be used to develop effective interventions, including the cognitive reappraisal training to improve the mental health and reduce the suicide attempts in adolescents.
Footnotes
Funding: This research was supported by the research fund of Dankook University in 2013 (No. 115694).
Authors declare that they have no conflict of interest
References
- 1.Organization of Economic Co-operation and Development. OECD factbook 2013: Economic, Environmental and Social Statistics. OECD Publishing; 2013. doi: 10.1787/factbook-2013-en. [Google Scholar]
- 2.Suokas J, Suominen K, Isometsä E, Ostamo A, Lönnqvist J. Long-term risk factors for suicide mortality after attempted suicide: findings of a 14-year follow-up study. Acta Psychiatr Scand. 2001;104:117–121. doi: 10.1034/j.1600-0447.2001.00243.x. [DOI] [PubMed] [Google Scholar]
- 3.Herba CM, Ferdinand RF, van der Ende J, Verhulst FC. Long-term associations of childhood suicide ideation. J Am Acad Child Adolesc Psychiatry. 2007;46:1473–1481. doi: 10.1097/chi.0b013e318149e66f. [DOI] [PubMed] [Google Scholar]
- 4.Kokkevi A, Rotsika V, Arapaki A, Richardson C. Changes in associations between psychosocial factors and suicide attempts by adolescents in Greece from 1984 to 2007. Eur J Public Health. 2011;21:694–698. doi: 10.1093/eurpub/ckq160. [DOI] [PubMed] [Google Scholar]
- 5.Kokkevi A, Rotsika V, Arapaki A, Richardson C. Adolescents' self-reported suicide attempts, self-harm thoughts and their correlates across 17 European countries. J Child Psychol Psychiatry. 2012;53:381–389. doi: 10.1111/j.1469-7610.2011.02457.x. [DOI] [PubMed] [Google Scholar]
- 6.Bridge JA, Goldstein TR, Brent DA. Adolescent suicide and suicidal behavior. J Child Psychol Psychiatry. 2006;47:372–394. doi: 10.1111/j.1469-7610.2006.01615.x. [DOI] [PubMed] [Google Scholar]
- 7.Jeon HJ, Bae J, Woo JM. Recent statistics and risk factors of suicide in children and adolescents. J Korean Med Assoc. 2013;56:93–99. [Google Scholar]
- 8.Zhang J, McKeown RE, Hussey JR, Thompson SJ, Woods JR. Gender differences in risk factors for attempted suicide among young adults: findings from the third National Health and Nutrition Examination Survey. Ann Epidemiol. 2005;15:167–174. doi: 10.1016/j.annepidem.2004.07.095. [DOI] [PubMed] [Google Scholar]
- 9.Burrows S, Laflamme L. Socioeconomic disparities and attempted suicide: state of knowledge and implications for research and prevention. Int J Inj Contr Saf Promot. 2010;17:23–40. doi: 10.1080/17457300903309231. [DOI] [PubMed] [Google Scholar]
- 10.Laflamme L, Burrows S, Hasselberg M. Socioeconomic differences in injury risks: a review of findings and a discussion of potential countermeasures. Copenhagen: World Health Organization Regional Office for Europe; 2009. [Google Scholar]
- 11.Chan WS, Law CK, Liu KY, Wong PW, Law YW, Yip PS. Suicidality in Chinese adolescents in Hong Kong: the role of family and cultural influences. Soc Psychiatry Psychiatr Epidemiol. 2009;44:278–284. doi: 10.1007/s00127-008-0434-x. [DOI] [PubMed] [Google Scholar]
- 12.Yoder KA, Hoyt DR. Family economic pressure and adolescent suicidal ideation: application of the family stress model. Suicide Life Threat Behav. 2005;35:251–264. doi: 10.1521/suli.2005.35.3.251. [DOI] [PubMed] [Google Scholar]
- 13.Evans E, Hawton K, Rodham K. Factors associated with suicidal phenomena in adolescents: a systematic review of population-based studies. Clin Psychol Rev. 2004;24:957–979. doi: 10.1016/j.cpr.2004.04.005. [DOI] [PubMed] [Google Scholar]
- 14.Boyce W, Torsheim T, Currie C, Zambon A. The family affluence scale as a measure of national wealth: validation of an adolescent self-report measure. Soc Indic Res. 2006;78:473–487. [Google Scholar]
- 15.Cho H, Khang Y. Family Affluence Scale, other socioeconomic position indicators, and self-rated health among South Korean adolescents: findings from the Korea Youth Risk Behavior Web-based Survey (KYRBWS) J Public Health. 2010;18:169–178. [Google Scholar]
- 16.Goodman E, Adler NE, Daniels SR, Morrison JA, Slap GB, Dolan LM. Impact of objective and subjective social status on obesity in a biracial cohort of adolescents. Obes Res. 2003;11:1018–1026. doi: 10.1038/oby.2003.140. [DOI] [PubMed] [Google Scholar]
- 17.Karvonen S, Rahkonen O. Subjective social status and health in young people. Sociol Health Illn. 2011;33:372–383. doi: 10.1111/j.1467-9566.2010.01285.x. [DOI] [PubMed] [Google Scholar]
- 18.Hanson MD, Chen E. Socioeconomic status and health behaviors in adolescence: a review of the literature. J Behav Med. 2007;30:263–285. doi: 10.1007/s10865-007-9098-3. [DOI] [PubMed] [Google Scholar]
- 19.Korea Centers for Disease Control and Prevention. The Eighth Korea Youth Risk Behavior Web-based Survey. Seoul: Ministry of Education, Science and Technology, Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention; 2012. [Google Scholar]
- 20.Korea Centers for Disease Control and Prevention. Reliability and validity of the Korea Youth Risk Behavior Web-based Survey questionnaire. Seoul: Ministry of Education, Science and Technology, Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention; 2009. [Google Scholar]
- 21.Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc Sci Med. 2008;66:1429–1436. doi: 10.1016/j.socscimed.2007.11.024. [DOI] [PubMed] [Google Scholar]
- 22.Boudreau B, Poulin C. An examination of the validity of the Family Affluence Scale II (FAS II) in a general adolescent population of Canada. Soc Indic Res. 2009;94:29–42. [Google Scholar]
- 23.Goodman E, Huang B, Schafer-Kalkhoff T, Adler NE. Perceived socioeconomic status: a new type of identity that influences adolescents' self-rated health. J Adolesc Health. 2007;41:479–487. doi: 10.1016/j.jadohealth.2007.05.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Glendinning A, Hendry L, Shucksmith J. Lifestyle, health and social class in adolescence. Soc Sci Med. 1995;41:235–248. doi: 10.1016/0277-9536(94)00316-l. [DOI] [PubMed] [Google Scholar]
- 25.Brunner E. Socioeconomic determinants of health: stress and the biology of inequality. BMJ. 1997;314:1472. doi: 10.1136/bmj.314.7092.1472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Piko B, Fitzpatrick KM. Does class matter? SES and psychosocial health among Hungarian adolescents. Soc Sci Med. 2001;53:817–830. doi: 10.1016/s0277-9536(00)00379-8. [DOI] [PubMed] [Google Scholar]
- 27.Taylor R, Morrell S, Slaytor E, Ford P. Suicide in urban New South Wales, Australia 1985-1994: socio-economic and migrant interactions. Soc Sci Med. 1998;47:1677–1686. doi: 10.1016/s0277-9536(98)00243-3. [DOI] [PubMed] [Google Scholar]
- 28.Noh YH. Determinants of suicidal ideation: a microeconometic analysis. Korean J Health Econ Policy. 2007;13:41–58. [Google Scholar]