

Abstract
Objective
To examine the impact of financial incentives on physician goal commitment to guideline-recommended hypertension care.
Study design
Clinic-level cluster-randomized controlled trial with four arms: control, individual-, group-, or combined incentives. Intervention arm participants received performance-based incentives every four months for five periods. All participants received guideline education at baseline and audit and feedback every four months.
Methods
83 full-time primary care physicians at 12 VA Medical Centers completed web-based survey responses to Hollenbeck’s goal commitment scale every four months and telephone interviews at months 8 and 16.
Results
Physician goal commitment did not vary over time or across arms. Participants reported patient non-adherence and consistent follow-up as perceived barriers and facilitators to successful hypertension care, suggesting providers may perceive hypertension management as more of a patient responsibility (external locus of control).
Conclusions
Financial incentives may constitute an insufficiently strong intervention to influence goal commitment when providers attribute performance to external forces beyond their control.
Keywords: Goal commitment, financial incentives, Pay-for-performance, mixed methods, physicians
BACKGROUND
Financial incentives as a tool to improve clinical quality are a growing trend in American health care1; insurers and hospitals are employing pay-for-performance programs to change clinician behavior and improve quality of care. Importantly, the Affordable Care Act of 2010 will implement a Value Based Purchasing Program in 2012 that offers financial incentives to hospitals based on the quality of care provided. Consequently, understanding how to incentivize providers’ behavior effectively may significantly improve quality of care.
Some researchers have identified an association between financial incentives and improved care, though these data are limited and additional evidence using rigorously designed methods is needed.2–7 In the largest randomized controlled trial to our knowledge of the impact of financial incentives on quality of care, preliminary findings by Petersen and colleagues8 found financial incentives improved blood pressure control or an appropriate clinical response to uncontrolled blood pressure suggesting financial incentives could impact care if designed correctly. However, we are not aware of any health care studies to date examining the mechanism by which financial incentives may act to change provider behavior. Without this knowledge, it is very difficult to design effective financial incentive programs.
Conceptual Model: The Role of Incentives in Provider Goal Setting
Research from both industrial/organizational psychology and management has demonstrated that financial incentives are linked to behavior resulting from setting and committing to a goal.9–13 According to Locke and Latham’s theory of goal setting and task motivation, setting goals positively impacts performance; goal commitment (i.e., the psychological commitment to achieving a goal) moderates this relationship such that the greater the goal commitment, the stronger the impact of setting goals will be on performance. Although increasing goal commitment is mostly accomplished via intrinsic means, such as increasing self-efficacy or expectancy of task attainment, financial incentives present one of the few extrinsic tactics an organization can use to improve goal commitment (and subsequently performance), particularly if goals are assigned rather than self-set.8 Figure 1 displays these relationships.
Figure 1.

Study-relevant relationships from Locke and Latham’s Theory of Goal Setting and Task Motivation.
Studies have shown that financial incentives are unrelated to performance once goal-setting is accounted for, 10,12,14 and that goal commitment is the key driver of goal setting behavior for self-set and assigned goals. Goal commitment has also been linked to increased planning activities, which in turn leads to improved performance, much like intension is linked to actual behavior.15,16 We therefore hypothesized that financial incentives would significantly impact provider goal commitment to guideline-recommended hypertension management. We are not aware of any studies in health care settings exploring the relationship between financial incentives and goal commitment, nor the impact of different financial incentive configurations (e.g., group versus individual).
METHOD
Design
This mixed methods study is part of a larger cluster-randomized controlled trial evaluating the impact of financial incentives on adherence to guidelines established in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) in the primary care setting. Primary care clinics within twelve geographically diverse VA Medical Centers were randomly assigned to one of four study arms: 1) audit and feedback only (control); 2) physician-level financial incentive + audit and feedback 3) group-level financial incentive + audit and feedback; 4) physician- and group-level financial incentives and audit + feedback (combined incentive).
The parent trial tests the impact of financial incentives (using the four arms described above) on improvements in three hypertension performance measures based on national guidelines (prescription of guideline-recommended medication, blood pressure control, and appropriate clinical response to uncontrolled blood pressure). A study protocol detailing the design and methods of this project has been published elsewhere.17 Performance data in the parent trial are collected via patient chart review. To assess the individual attitudes, cognitions, and interactions of interest in the current study, we surveyed and interviewed participating clinical personnel at multiple time points to explore their commitment to meeting guideline recommended hypertension management goals and improvement strategies. This mixed methods design allows quantitative attitudinal data to be linked to the chart review data to explore causal pathways between financial incentives and performance, and qualitative data to gain a richer understanding of how these attitudes and explanatory phenomena manifest themselves in clinic settings.
Participants
We recruited 83 primary care physicians (approximately seven from each site) who reported a full-time equivalent (FTE) of at least 0.60 (approximately 3 days per week related to clinical activities) or had a panel size of at least 500 patients (see Table 1).
Table 1.
Physician characteristics.
| Characteristic | N | % | Characteristic | N* | % |
|---|---|---|---|---|---|
| Gender - Male | 45 | 54 | Years Practicing Since Residency Completion | ||
| Race | Less than 5 | 12 | 14 | ||
| White or Caucasian | 35 | 42 | 5–9 | 19 | 23 |
| Asian Indian | 23 | 28 | 10–14 | 26 | 31 |
| Asian* | 11 | 13 | 15–19 | 9 | 11 |
| African American | 6 | 7 | 20 or more | 17 | 20 |
| Hispanic | 4 | 5 | M | SD | |
| Other | 3 | 4 | Distribution of Work Duties | ||
| No Answer | 1 | 1 | % Time in Direct Primary Care | 89 | 13 |
| Primary Specialty | % Time in Teaching | 5 | 7 | ||
| Internal Medicine | 71 | 86 | % Time in Research | 1 | 6 |
| General/Family Medicine | 12 | 14 | % Time in Administration | 5 | 9 |
Asian includes Chinese, Japanese, Korean, and Vietnamese; “Asian” and “Asian Indian” are mutually exclusive.
Measures
Goal commitment
Hollenbeck’s seven-item Likert-type scale 18 was used to measure goal commitment as part of the audit and feedback process (see Appendix A). This measure is widely used in the organizational literature; reported reliability is 0.7118.
Knowledge and attitudes about guidelines
One possible confounder of goal commitment levels is previous knowledge and attitudes about hypertension management; for example, if participants hold negative views about the utility or appropriateness of the guidelines for managing hypertension, goal commitment would be unduly low. To account for confounders, participants completed a knowledge and attitudes questionnaire after viewing an educational presentation on the JNC 7 Hypertension Guidelines (see Provider Education section below). The questionnaire included questions about prior awareness and understanding of the JNC 7 guidelines, agreement with its recommendations, and self-reports of whether the respondents apply the guideline’s recommendations. Participants also completed a demographics survey upon enrollment. Appendix A presents both questionnaires.
Planning Quality
Because goal commitment is associated with improvements in planning behaviors, which lead to improved performance, we sought to qualitatively identify participants’ planning and improvement strategies in hypertension care. We employed Smith and colleagues’ taxonomy,19 who posit seven characteristics indicative of high quality planning efforts: (1) clear definitions of roles and functions; (2) systematic SWOT analysis; (3) development of action plans; (4) communication of action plans; (5) extensive interaction among team members; (6) allocation of resources, and (7) future orientation (i.e., thinking longer term). The more of these characteristics that are present in planning efforts, the higher the quality. It is these later characteristics of allocation of resources and future orientation that are most likely to lead to actual changes in behavior; we coded for evidence of these characteristics in our interviews as our means of assessment.
Intervention Components
Provider education
All participants received a standardized, web-based presentation summarizing the JNC 7 guidelines and educating participants about their study arm assignment and the study performance measures. A question and answer session followed. All participants also received pocket cards summarizing the JNC 7 guidelines and the study performance measures. The study website contained links to this presentation, pocket card, other JNC 7 resources, and patient resources for lowering blood pressure.
Financial incentives
Participants in the intervention arms received payments approximately every four months over a 20-month intervention period. Incentive payments rewarded participants for chart-documented care of hypertensive patients (i.e., prescribing guideline-recommended antihypertensive medications, providing guideline-recommended responses to an uncontrolled blood pressure, and blood pressure control. See Petersen et al. 2011 for chart abstraction and criterion data collection process details)17. In the individual arm, each physician received a direct payment based on his/her guideline adherence. In the group arm, a payment based on the collective performance of the participating physicians in the group was divided equally amongst all group members (both physician and non-physician). In the combined arm, each physician received a direct payment based on his/her adherence; additionally, a payment based on the overall adherence of the physicians in the group was divided equally amongst all group members.
Audit and feedback
Audit and feedback reports were delivered to participants in all four arms approximately every four months for five consecutive periods via a website. Reports were designed based on the tenets of Feedback Intervention Theory,20 employing feedback characteristics found to improve feedback effectiveness in health care.21 The report showed the percent of patients meeting each performance measure, the amount earned for meeting each measure (incentive arm reports only), and performance goals for the following period, a feature shown to improve feedback effectivenesss20,22 but not often found in feedback reports (see Appendix B for a sample feedback report). The participants’ goal was to reach a benchmark based on the top performers in the previous period.23 We tracked participant visits to the feedback reports to identify who viewed their report and thus had the opportunity to cognitively link their earnings to their performance.
Procedure
Human subjects and informed consent
We obtained Institutional Review Board (IRB) approval at each of the twelve sites in the study. We followed the approval requirements for the most conservative IRB to secure approvals at all sites.
Surveys
Physicians completed three surveys: (1) a demographics survey upon enrollment in the study; (2) a knowledge and attitudes survey about the JNC-7 hypertension guidelines, administered as part of their provider education; and (3) a post-feedback survey containing Hollenbeck’s goal commitment measure, completed after receipt of each audit and feedback report. This survey also served to check that participants read their reports.
Interviews
Two rounds of 30-minute telephone interviews were conducted at each clinic, one each at months 8 and 16 (time points 2 and 4) of the study intervention period. Two physician participants were randomly selected from each site and invited to participate in the interviews; similarly, two non-physician clinicians (e.g., nurse practitioner, case manager) were selected from each site with a group incentive and invited to participate. Interview topics included any planning activities the participant employed to improve their quality of hypertension care and clinic operations. Appendix A lists the questions used to capture these constructs. The questions were deliberately broad and open-ended to avoid leading the participants and to capture a wide range of potential behaviors. Interviews were transcribed and analyzed using Atlas.ti. 6.2. Each transcript was reviewed and coded for themes by a trained coder and verified by an independent coder. Disagreements between coders were resolved by discussion and consensus; the lead author served as tiebreaker when needed.
Results
Survey Response Rates
Demographics
All 83 physician participants completed the survey (100% response rate).
Knowledge and attitudes
78 of the 83 physician participants completed the survey (93.98% response rate).
Goal commitment
Table 2 summarizes goal commitment response rates. Of the physicians who received a feedback report each period, a mean of 42.45% viewed the feedback report. Goals were assigned to participants via the feedback report; thus, only amongst participants who viewed the feedback report could goal commitment mediate the relationship between financial incentives and performance. Thus, the appropriate denominator for this response rate is the number of physicians who viewed the feedback report, rather than all 83 physicians. Of these physicians, a mean of 78.48% completed the survey.
Table 2.
Physician response rates to goal commitment survey by study period.
| Period | |||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| Number of physicians who viewed their feedback report | 46 | 27 | 30 | 30 | 25 |
| Number of physicians who completed post- feedback survey | 35 | 18 | 23 | 26 | 22 |
| Percent of physicians who viewed their feedback report who completed post-feedback survey | 76.09% | 66.67% | 76.67% | 86.67% | 88.00% |
There were no significant differences in demographic characteristics or study arm assignment between the intervention arm physicians who viewed their feedback report and those who did not for any of the five periods (only one control arm participant viewed the feedback report over more than one period, hence the intervention arm-restricted comparisons). Similarly there were no significant differences in knowledge and attitudes between intervention arm physicians who did and did not view their feedback report; the only exception occurred during period 2, where intervention arm physicians who did not visit the feedback report were more likely to agree with lifestyle modification as an acceptable treatment than those who did view their feedback report (F(1,58) = 5.52, p<.022). Because lifestyle modification was one of several possible ways to receive an incentive, this is unlikely to significantly impact goal commitment to guideline adherence.
Reliability Analysis
We calculated Chronbach’s alpha on the goal commitment scale to check its internal consistency reliability. Analyses showed acceptable levels of reliability at 0.78.
Knowledge and Attitudes about Hypertension Guidelines
Table 3 summarizes physicians’ knowledge and attitudes about guidelines. As can be seen from the table, most respondents were aware of and agreed with the JNC 7 guidelines, making attitudes an unlikely reason for goal commitment scores to be artificially deflated. Percentages noted in Table 3 did not significantly vary by study arm.
Table 3.
Physician knowledge and attitudes about JNC 7 guideline recommendations.
| Knowledge or Attitude Marker | Percent |
|---|---|
| Read either the full or summarized JNC 7 guideline report | 73% |
| Reported having a good or excellent understanding of the guideline before the educational presentation | 62% |
| Agreed or strongly agreed with the guideline’s recommendations, regardless of their prior knowledge. | 81% |
| Reported implementing the hypertension guidelines with their patients. | 61% |
Hypothesis Test
To test the hypothesis that financial incentives positively impact goal commitment, we conducted a repeated measures analysis of variance amongst the intervention armsi. This test, establishing a relationship between the independent variable and the potential mediator, is the first step in establishing goal commitment as a mediating mechanism between financial incentives and adherence to guideline recommended hypertension management24,25. Table 4 presents means and standard deviations for each study arm; Table 5 presents the results of the repeated measures analysis of variance. Initial diagnostic analyses indicated goal commitment exhibited very limited variability. As shown in Table 5, we found no significant differences in goal commitment over time or across arms, nor did time and study arm interact to produce any significant effects. Our hypothesis was thus not supported. As no relationship was found between financial incentives and goal commitment, the latter cannot serve as an explanatory mechanism through which financial incentives operate; thus, no further analyses were needed or conducted.
Table 4.
Means and Standard Deviations for physician goal commitment over five study periods, by study arm.
| Study Arm | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| ||||||||||||
| Study Period | Control | Combined Incentive | Group Incentive | Individual Incentive | ||||||||
|
| ||||||||||||
| Mean | SD | N | Mean | SD | N | Mean | SD | N | Mean | SD | N | |
| 1 | 2.81 | .36 | 3 | 3.06 | .71 | 23 | 2.95 | .48 | 15 | 2.83 | .35 | 10 |
| 2 | 2.57 | . | 1 | 2.63 | .55 | 16 | 2.78 | .33 | 15 | 3.18 | .24 | 4 |
| 3 | 2.86 | . | 1 | 2.80 | .63 | 19 | 2.75 | .61 | 16 | 2.88 | .35 | 6 |
| 4 | 2.29 | . | 1 | 2.75 | .68 | 16 | 2.85 | .39 | 16 | 2.76 | .26 | 7 |
| 5 | 2.29 | . | 1 | 2.87 | .62 | 17 | 2.76 | .33 | 13 | 2.71 | .34 | 7 |
Table 5.
Repeated Measures Analysis of Variance Results Summary
| Source | SS | df | MS | F | P |
|---|---|---|---|---|---|
| Between subjects | |||||
| Intercept | 282.86 | 1 | 282.86 | 637.62 | .00 |
| Study Arm | .51 | 2 | .25 | .57 | .61 |
| Error 1 | 1.77 | 4 | .44 | ||
| Within subjects (Huynh-Feldt correction) | |||||
| Time | .30 | 4 | .08 | .84 | .52 |
| Time X Study Arm | .39 | 8 | .05 | .54 | .81 |
| Error 2 | 1.45 | 16 | .09 | ||
Follow-Up Interviews
As the literature specifically identifies planning as an outcome of improved goal commitment, we searched for evidence of planning activities to help improve hypertension care at each site. We employed Smith, Locke, and Barry’s taxonomy of planning quality19 to search for evidence of the aforementioned planning characteristics. Three characteristics, extensive interaction, development of action plans, and communication of action plans, emerged as the most central to planning improvements in hypertension care:
I: So they were asking you for input on how to manage hypertension, is that what I’m hearing?
R: It was like a group session, you know just in a group, it was like feedback. …
I: So tell me a little bit about what got discussed in that meeting. …
R: Well, it’s just, the uh, on the sheet, you know they’d be discussing just what, for the BP, for the sheet that they sent us. Like that.
I: So the notification sheet is something that came out of that feedback meeting?
R: Yes, ma’am.
I: And do you think that at that meeting people had a pretty good chance to sort of, you know, express their ideas or throw ideas into the mix?
R: Oh yes. Yes.
I: Did anybody try during that meeting or at any other time try to identify strengths and weaknesses of the clinic or ways the clinic could improve? Or was that it?
R: That was it.
-- Non-physician clinician in combined site A
Interestingly, however, the later characteristics of planning quality, allocation of resources and future orientation, were scarce in our data; indeed, no passages were identified in our data as indicative of future orientation. This pattern was consistent across sites and arms.
As we found no differences across arms in our quantitative analysis of goal commitment and no differences across arms in our qualitative analysis of planning quality, our next step was to search for external factors, that is, barriers and facilitators, to improving management of hypertension. Patient non-adherence emerged as the chief barrier to guideline adherence:
We need mamas as far as the non-compliance is concerned. A lot of these patients really need a mother, a wife, whatever to make them take their medicines. If the VA could find someone to make the patients take their medicine, like a dorm mother or something, the numbers would look a lot better.
--Physician, control site A
Problems such as patient mental illness and inaccurate or missing patient contact information were cited as specific issues exacerbating the non-adherence barrier; however, the most often reported barrier in conjunction with patient non-adherence was lack of follow-up:
Seeing the patient back promptly for re-evaluation. That’s the key part. If they come back late, that’s time lost…Within a month, unless it’s really high, then maybe a week. But for stage 1 hypertension, a month is good to get it addressed.
-- Physician, individual incentive site A
Consequently, the most reported solution to help improve guideline adherence was a dedicated way of providing consistent patient follow-up.
“So as a team, just starting from the nurse, they try to reinforce compliance with meds, lifestyle modifications, that kind of education. As a team we formulate a plan on how often to see the patient and after making adjustments, as a team we tell them what they need to be doing and give them an appointment in the near future to check it again. We go over the list and see who we need to see for the adjustments. That has helped actually, bringing them in more often…3 months is normal but some--on multi-drug regimen--we try to bring them back more often than that.”
-- Physician, combined incentive site B
For example, sites reported assigning the task of patient follow-up to other primary care personnel, such as nurses, case managers, or pharmacists, who had more capacity in their schedules to provide regular follow-up instead of the primary care provider.
There are patients who have a difficulty coming back and forth to the clinic with transportation issues, etc. With those patients putting in the referral to the CM really worked because she could get the information over the phone and reinforce education, dietary compliance. This saved the patient trips and we got a better result with better readings.
-- Physician, group incentive site B
These findings, patient non-adherence and patient follow-up, were mentioned consistently across sites in all four arms. We found no evidence in the qualitative data of any phenomena known in the literature to impact goal commitment, such as internal locus of control 26, self-efficacy, or an inspiring vision that would increase the importance of the goal 14,27.
Discussion
We assessed the effect of financial incentives on physician goal commitment to adhere to hypertension management guidelines. Results from our quantitative survey revealed no variability in physician goal commitment over time or across study arms; physician attitudes about guidelines were generally positive, and did not significantly vary across study arms. A priori qualitative analysis of interviews using Smith et al.’s taxonomy of planning quality showed consistently across arms some amount of development and communication of action plans to improve hypertension care, though little evidence of allocating resources for the developed action plans. Finally, post-hoc qualitative analyses of interviews identified patient non-adherence and consistent follow-up with patients as perceived barriers and facilitators to successful hypertension care, regardless of study arm.
Provider perceptions of non-adherence could explain why we found no effect, and might suggest the presence of physician perceptions of external locus of control for hypertension care. That is, physicians may believe the outcome of hypertension care is mostly a patient responsibility, and thus perceive to have little control over outcomes. Therefore, they would see no benefit in committing to a goal that they perceive as unachievable. Non-adherence perceptions could also explain the absence of resource allocation and future orientation noted during the telephone interviews.
An alternative possible explanation for our finding of a lack of variability in goal commitment: the existing VA policies and systems for hypertension management and clinical performance. VA has various systems in place nationwide to improve and ensure quality. For example, hypertension performance measures exist where facilities are monitored and compared quarterly both to target performance standards and to other facilities;28 additionally, electronic clinical reminders exist to help ensure providers deliver the required care during the patient encounter. This set of structures results in what is known in organizational psychology as a strong situation 29 - i.e., one that is construed similarly by participants, 30 that induces uniform expectancies, whose incentives are intended to induce a uniform response, and where everyone has the skills to perform to standard. Faced with these parameters, goal commitment for hypertension care was unlikely to vary among physicians, and thus consequently unable to impact hypertension care.
This has important implications for creating a culture that values quality of care: although structural elements such as policies and decision aids are critical foundations for high quality care 31, care must be taken to not squelch individual-level drivers of provider behaviors that result in higher quality care, such as goal commitment, locus of control, and self-efficacy. Fundamentally, whether working alone or in a team, it is the actions of individuals that result in higher or lower quality care, and whether by structures, incentives, or other forms of intervention, it is the behavior of individuals that we ultimately seek to change. We caution, however, that the explanation of a strong situation was not endorsed one way or the other by the participant interviews.
Limitations
Our biggest limitation was sample size, particularly the dwindling number of respondents as the study progressed over time. However, the lack of significant findings in our study was not due to too much variability to detect an effect, which is often the case with small sample sizes (i.e., the means appear to be different, but because of the large error terms resulting from the small sample size, significance cannot be established). On the contrary, this was due to insufficient variability: most physicians, regardless of study arm, exhibited a consistently modest level of goal commitment over time. Thus we can exhibit some level of confidence in our findings, despite the small sample size 32.
Conclusion
We conclude that to the extent that external forces, such as strong situations or perceptions of external locus of control, influence physician goal commitment to hypertension care, financial incentives may be an insufficiently strong intervention to overcome these other influences on goal commitment, thus limiting the ability of goal commitment to serve as an operating mechanism for financial incentives. More research is needed to better understand the behavioral levers triggered by financial incentives in the clinician population, so as to better target both pay-for-performance and other quality improvement initiatives.
Take-away points.
Designers of pay-for-performance programs for clinicians should consider rewarding behaviors and outcomes under direct clinician control, as well as behaviors and outcomes where there is room for individual goal commitment to increase, in order to maximize the likelihood that the incentive will result in a positive clinical outcome.
Acknowledgments
Source of funding:
The research reported here was supported by the Department of Veterans Affairs, Health Services Research and Development Service (VA HSR&D) (IIR 04-349, CDA 07-0181 & HFP #90-020) and by the National Heart, Lung, & Blood Institute of the National Institutes of Health (NHLBI 1R01HL079173, NHLBI 1R01HL079173-S1, NHLBI 1R01HL079173-S2)
Appendix A: Measures Used in this Study
Hollenbeck’s Goal Commitment Measure
We used Hollenbeck’s 7-item scale 18 to measure goal commitment. This scale is well documented, has good reliability and construct evidence of validity,18 and has been used widely for this purpose. Respondents will rate items on the 5-point Likert scale below.
What do you think of the hypertension treatment goals you received in your feedback report?
It’s hard to take these goals seriously.
It’s unrealistic for me to expect to reach these goals.
It is quite likely that these goals may need to be revised, depending on how things go.
Quite frankly, I don’t care if I achieve these goals or not.
I am strongly committed to pursuing this goal
It wouldn’t take much to make me abandon this goal
I think this goal is a good goal to shoot for.
Response Choices:
1= strongly agree
2= agree
3= neither agree nor disagree
4= disagree
5=strongly disagree
Demographics Survey
What is your PERCENT (%) FTEE in the clinic? _________
-
What is your GENDER?
-
□
Male
-
□
Female
-
□
What is your AGE? _________
What is your DATE OF BIRTH? __________________
-
What is the RACE/ETHNICITY that best describes you?
-
□
White or Caucasian
-
□
Black or African American
-
□
Asian (Chinese, Japanese, Korean, Vietnamese)
-
□
Asian Indian
-
□
Native Hawaiian/Other Pacific Islander
-
□
Hispanic/Spanish/Cuban/Mexican American/Puerto Rican/Latino/Chicano/Haitian
-
□
American Indian/Alaska Native
-
□
Other (please fill in the blank):________________________________
-
□
Refused to answer
-
□
-
What is your DEGREE(S)?
-
□
M.D.
-
□
D.O.
-
□
Other (please fill in the blank): _________
-
□
What year did you graduate from medical school? _________
-
Are you BOARD CERTIFIED? _________
If yes, what year were you last board certified? _________
-
What is your primary specialty?
-
□
Internal Medicine
-
□
General/Family Practice
-
□
Other (please fill in the blank):________________________________
-
□
-
Do you have a SUBSPECIALTY or SECONDARY SPECIALTY in the following areas? Check all that apply.
-
□
Nephrology
-
□
Cardiology
-
□
Geriatrics
-
□
Endocrinology
-
□
Other (please fill in the blank):________________________________
-
□
No subspecialty/secondary specialty
-
□
How many years have you been in practice since the completion residency? _________
-
What percentage of your professional time is spent in each of the following professional roles? (should add to 100%)
-
□
Direct Primary Care ________%
-
□
Teaching ________%
-
□
Research ________%
-
□
Administration ________%
-
□
-
What is your annual household gross income? (Please select one.)
-
□
Less than $100,000
-
□
$100,000– $125,000
-
□
$125,001– $150,000
-
□
$150,001– $175,000
-
□
$175,001–$200,000
-
□
$200,001– $225,000
-
□
$225,001– $250,000
-
□
$250,001– $275,000
-
□
$275,001– $300,000
-
□
Over $300,000
-
□
Refused to answer
-
□
Knowledge and Attitudes Survey
Thank you for participating in the RIGHT-BP study. We would like to know a little more about how you currently manage your patients’ hypertension, and your views on the JNC 7 hypertension guidelines and the information you received in the educational presentation. We would greatly appreciate your taking 5–10 minutes to complete our questionnaire.
-
In my clinic we provide the following hypertension management resources (check all that apply):
-
□
a. Educational literature/materials for the patient
-
□
b. Educational workshops for the patient
-
□
c. Hypertensive patient registry
-
□
d. Web-based blood pressure monitoring tools (e.g., My Health-e Vet)
-
□
e. Patient educational reminders (e.g., periodic mailings reminding patients to eat healthfully)
-
□
f. Reminders to patients of upcoming clinical appointments
-
□
g. Reminders to patients of upcoming medication refills
-
□
h. Pharmacy feedback systems to monitor patient compliance with medication (e.g., provider reminders that medication supply should be running out for patients)
-
□
i. Group visits for hypertension
-
□
j. None of the above
-
□
-
To what extent were you aware of the JNC 7 guideline for treatment of hypertensive patients before today’s information session (check all that apply – skip to question 5 if you select a or b)?
-
□
a. I was not aware that JNC had issued a hypertension guideline.
-
□
b. I was aware of its existence, but not aware of its contents
-
□
c. I had read the physician reference card.
-
□
d. I had used the PDA application.
-
□
e. I had read the JNC 7 Express Report.
-
□
f. I had read the full report.
-
□
Please rate how strongly you agree with each of the following statements, using the following scale:
1= strongly disagree
2= somewhat disagree
3 = neither agree nor disagree
4= somewhat agree
5= strongly agree
| Strongly disagree → Strongly agree | |||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| 3. Before today’s presentation, I had an excellent understanding of the JNC 7 guideline’s recommendations | |||||
| 4. I currently implement the guideline’s recommendations with all my hypertensive patients | |||||
| Given what you learned from our educational presentation, please rate how much you agree with the JNC 7 guidelines’ recommendations using the scale above | |||||
| 5. Lifestyle modification recommendations | |||||
| 6. List of compelling indications for hypertension treatment | |||||
| 7. Use of thiazide-type diuretics as the first line of defense for most hypertensives | |||||
| 8. Use of 2-drug combination for patients with Stage 2 hypertension | |||||
| Please rate how strongly you agree with each of the following statements, using the scale above | |||||
| 9. I have a better understanding of the JNC 7 guideline now than before today’s presentation. | |||||
| 10. The incentive process was explained well to me. | |||||
| 11. I have a good understanding of how the reward in this study will be calculated. | |||||
| 12. The process for calculating the reward is fair. | |||||
| 13. The criteria used to evaluate how well I follow the guideline’s medication recommendations are fair. | |||||
| 14. The criteria used to evaluate how well I control my patients’ blood pressure are fair. | |||||
| 15. The amount of the incentive would motivate me to improve. | |||||
| 16. In general, financial incentives are a useful tool for improving quality of hypertension care. | |||||
Thank you for your candid responses, and for participating in our study!
Semi-Structured Interview Question Pool
As a ________________ (job title), what is your key responsibility in managing your patients’ hypertension?
Who else in the primary care team plays a key role in managing your patients’ hypertension? What are their key roles and responsibilities in managing patients’ hypertension (e.g., nurses are responsible for x, y, and z)
How do primary care team members communicate information about a patient’s situation?
Think about the last time your primary care team worked very well together as a team to manage a patient’s hypertension. What was the situation? What did the team do that was so successful? What was the result?
Think about the last time your primary care team worked very poorly together as a team to manage a patient’s hypertension. What was the situation? What did the team do that was so problematic? What was the result?
On a scale of 1 to 10, with your successful example being a 10 and your poor example being a 1, where does your primary care team operate most of the time with respect to hypertension care? Why?
What efforts, if any, were made to identify strengths, weaknesses, and opportunities for the clinic to improve?
Appendix B: Sample Audit and Feedback Report for the Third Performance Period for a Physician in the Combined Incentive Arm
| Your Scores This Period: | You | Your group | ||
|---|---|---|---|---|
|
| ||||
| # of pts (%) | You earned | # of pts (%) | Group earned | |
| Number of eligible hypertensive patients randomly sampled from your panel/group | 40 | 280 | ||
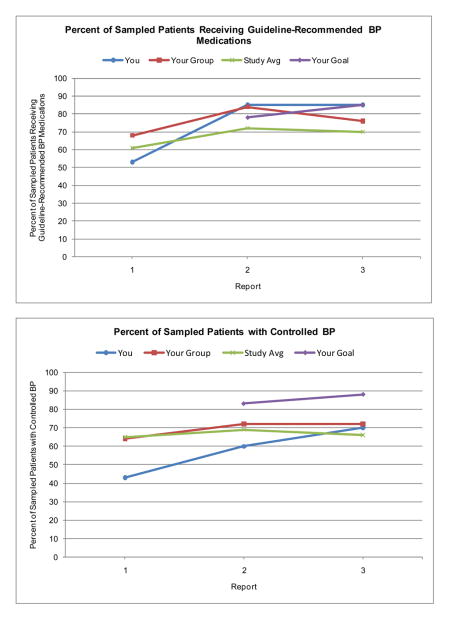
| Number of patients who received guideline-recommended BP medications | 34 (85%) | $309.40 | 213 (76%) | $1,938.30 |
| Congratulations! You are among the top 10% of performers across the entire study for this period. | ||||
| Number of patients with controlled BP | 28 (70%) | $254.80 | 201 (72%) | $1,829.10 |
| Number of patients with uncontrolled BP… | 12 (30%) | 79 (28%) | ||
| … who received an appropriate clinical response to uncontrolled BP this period | 4 (33%) | $36.40 | 42 (53%) | $382.20 |
|
| ||||
| Total Earnings: | ||||
|
| ||||
| This period - Congratulations! Good work! | $600.60 | $4,149.60 | ||
| Overall | $1,583.30 | $11,657.10 | ||
| Your Goals for the Upcoming Period: | You | Your group | ||
|---|---|---|---|---|
|
| ||||
| % of pts. | % of pts. | |||
| Percent of eligible hypertensive patients in your panel/group… | ||||
| … who will receive guideline-recommended BP medications | 85% | 85% | ||
| For the next period, your goal is to maintain or exceed your current performance level. Keep up the great work! | ||||
| … with controlled BP | 85% | 85% | ||
| … with uncontrolled BP who will receive an appropriate clinical response to uncontrolled BP | 83% | 83% | ||
| If you and your group meet or exceed your goals next period, you and your group could earn at least: | $664.30 | $4,650.10 | ||
|
| ||||
| Total earnings that you will receive this period: | $946.40 | |||
Graphs of Performance over Time from Sample Report
Footnotes
The control arm was not included in these analyses due to insufficient sample size (only one participant from the control arm chose to respond to our survey).
References
- 1.Committee on Quality of Health Care in America. Rewarding Provider Performance: Aligning Incentives in Medicare. Washington DC: National Academies Press; 2006. [Google Scholar]
- 2.Petersen LA, Woodard LD, Urech T, Daw C, Sookanan S. Does Pay-for-Performance Improve the Quality of Health Care? Annals of Internal Medicine. 2006 Aug 15;145(4):265–72. doi: 10.7326/0003-4819-145-4-200608150-00006. [DOI] [PubMed] [Google Scholar]
- 3.Rodriguez HP, von GT, Elliott MN, Rogers WH, Safran DG. The effect of performance-based financial incentives on improving patient care experiences: a statewide evaluation. J Gen Intern Med. 2009 Dec;24(12):1281–8. doi: 10.1007/s11606-009-1122-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chung S, Palaniappan LP, Trujillo LM, Rubin HR, Luft HS. Effect of physician-specific pay-for-performance incentives in a large group practice. Am J Manag Care. 2010 Feb;16(2):e35–e42. [PubMed] [Google Scholar]
- 5.Jha AK, Orav EJ, Epstein AM. The effect of financial incentives on hospitals that serve poor patients. Ann Intern Med. 2010 Sep 7;153(5):299–306. doi: 10.7326/0003-4819-153-5-201009070-00004. [DOI] [PubMed] [Google Scholar]
- 6.Lester H, Schmittdiel J, Selby J, Fireman B, Campbell S, Lee J, Whippy A, Madvig P. The impact of removing financial incentives from clinical quality indicators: longitudinal analysis of four Kaiser Permanente indicators. BMJ. 2010;340:c1898. doi: 10.1136/bmj.c1898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Scott A, Sivey P, Ait OD, Willenberg L, Naccarella L, Furler J, Young D. The effect of financial incentives on the quality of health care provided by primary care physicians. Cochrane Database Syst Rev. 2011;9:CD008451. doi: 10.1002/14651858.CD008451.pub2. [DOI] [PubMed] [Google Scholar]
- 8.Petersen L, Simpson K, Woodard LD, et al. Do financial incentives for guidelines adherence improve care of hypertension in the primary care setting? A multi-site RCT 2011. 2012 May 4; [Google Scholar]
- 9.Wright PM. Monetary incentives and task experience as determinants of spontaneous goal setting, strategy development, and performance. Human Performance. 1990;3(4):237–58. [Google Scholar]
- 10.Wright PM. Test of the mediating role of goals in the incentive^performance relationship. [References] Journal of Applied Psychology. 1989;74(5):699–705. [Google Scholar]
- 11.Locke EA. Toward a theory of task motivation and incentives. Organizational Behavior & Human Performance. 1968;3(2):157–89. [Google Scholar]
- 12.Locke EA, BRYAN JF, KENDALL LM. Goals and intentions as mediators of the effects of monetary incentives on behavior. [References] Journal of Applied Psychology. 1968;52(2):104–21. [Google Scholar]
- 13.Riedel JA, Nebeker DM, Cooper BL. The Influence of Monetary Incentives on Goal Choice, Goal Commitment, and Task-Performance 1. Organizational Behavior And Human Decision Processes. 1988 Oct;42(2):155–80. [Google Scholar]
- 14.Locke EA, Latham GP. Building a practically useful theory of goal setting and task motivation: A 35-year odyssey 300–314. 2002;57(9):705–17. doi: 10.1037//0003-066x.57.9.705. [DOI] [PubMed] [Google Scholar]
- 15.Stout RJ, Cannon-Bowers JA, Salas E, Milanovich DM. Planning, Shared Mental Models, and Coordinated Performance: An Empirical Link Is Established. Human Factors. 1999;41(1):61–71. [Google Scholar]
- 16.Mathieu JE, Goodwin GF, Heffner TS, Salas E, Cannon-Bowers JA. The Influence of Shared Mental Models on Team Process and Performance. Journal of Applied Psychology. 2000;85(2):273–83. doi: 10.1037/0021-9010.85.2.273. [DOI] [PubMed] [Google Scholar]
- 17.Petersen LA, Urech T, Simpson K, Pietz K, Hysong SJ, Profit J, Conrad DA, Dudley RA, Lutschg MZ, Petzel R, Woodard LD. Design, rationale, and baseline characteristics of a cluster randomized controlled trial of pay for performance for hypertension treatment: Study Protocol. Implementation Science. 2011 Oct 3;6(1):114. doi: 10.1186/1748-5908-6-114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hollenbeck JR, Klein HJ, O’Leary AM, Wright PM. Investigation of the construct validity of a self-report measure of goal commitment. Journal of Applied Psychology. 1989 Dec;74(6):951–6. [Google Scholar]
- 19.Smith KG, Locke EA, Barry D. Goal-Setting, Planning, and Organizational Performance - An Experimental Simulation 3. Organizational Behavior And Human Decision Processes. 1990 Jun;46(1):118–34. [Google Scholar]
- 20.Kluger AN, DeNisi A. The effects of feedback interventions on performance: A historical review, a meta-analysis, and a preliminary feedback intervention theory. Psychological Bulletin. 1996;119(2):254–84. [Google Scholar]
- 21.Hysong SJ. Meta-Analysis: Audit & Feedback Features Impact Effectiveness on Care Quality. Medical Care. 2009;47(3):356–63. doi: 10.1097/MLR.0b013e3181893f6b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kluger AN, DeNisi A. Feedback interventions: Toward the understanding of a double-edged sword. Current Directions in Psychological Science. 1998;7(3):67–72. [Google Scholar]
- 23.University of Alabama at Birmingham - Center for Outcomes and Effectiveness Research & Education. [Accessed October 26, 2011];The Achievable Benchmark of Care (ABC) System. 2005 Available at: URL: http://main.uab.edu/show.asp?durki=14527.
- 24.Baron RM, Kenny DA. The moderator-mediator variable discinction in social psychological research: Conceptual, strategic, and statistical considerations 95054970. 1986;51:1173–82. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- 25.Kenny DA. Mediation. 2011 Dec 21; Available at: URL: http://davidakenny.net/cm/mediate.htm.
- 26.Erez A, Judge TA. Relationship of core self-evaluations to goal setting, motivation, and performance. J Appl Psychol. 2001 Dec;86(6):1270–9. doi: 10.1037/0021-9010.86.6.1270. [DOI] [PubMed] [Google Scholar]
- 27.Wofford JC, Goodwin VL, Premack S. Meta-analysis of the antecedents of personal goal level and of the antecedents and consequences of goal commitment. J Manage. 1992 Sep;18(3):595–615. [Google Scholar]
- 28.Hysong SJ, Khan M, Petersen LA. Passive Monitoring versus Active Assessment of Clinical Performance: Impact on Measured Quality of Care. Medical Care. 2011 Oct 1;49(10):883–90. doi: 10.1097/MLR.0b013e318222a36c. [DOI] [PubMed] [Google Scholar]
- 29.Chatman J. Improving interactional organizational research: A model of person-organization fit. Academy of Management Review. 1989;14(3):333–49. [Google Scholar]
- 30.Hysong SJ, Petersen LA. Provider Knowledge and Attitudes toward Hypertension Guidelines Impact Implementation of Evidence-Based Care. New Orleans, LA: 2008. [Google Scholar]
- 31.Hysong SJ, Esquivel A, Sittig DF, Paul LA, Espadas D, Singh S, Singh H. Toward Successful Coordination of Electronic Health Record Based-Referrals: A Qualitative Analysis. Implementation Science. 2011;6(84) doi: 10.1186/1748-5908-6-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Darlington RB. Regression and Linear Models. New York: McGraw-Hill; 1990. [Google Scholar]