

Abstract
Self-rated health (SRH) is a valid measure of health status and associated with mortality. Based on individual-level biannual repeat data on SRH we sought to characterize the natural history of poor SRH during the 12 years prior to death in men and women in different age groups. We conducted a retrospective analysis of the Health and Retirement Study participants who died between 1998 and 2010 and had at least two SRH measurements in the 12 years prior to death. We used a nested case-control design to compare SRH trajectories of deceased men and women aged 30–64, 65–79 and 80 years versus surviving participants. The cases comprised 3,350 deceased participants who were matched to surviving controls (n = 8,127). SRH was dichotomized into good vs. poor health. Men and women dying at age 65–79 and ≥80 years had 1.5 to 3 times higher prevalence of poor SRH already 11–12 years prior to death compared to surviving controls. The risk estimates remained statistically significant even after adjusting for life-style related risk factors and diagnosed diseases. Prevalence of poor SRH before death was lowest among those aged ≥80 years and highest in 30–64 year-olds. In conclusion, men and women who subsequently die perceive their health worse already 11–12 years prior to death compared to their surviving controls.
Introduction
The one-item assessment of self-rated health (SRH) is a global measure of health status that is widely used in surveys partly because of its simplicity and convenience. SRH has been shown to capture a wide range of health-related phenomena, such as chronic diseases, health behaviors, symptoms, functional limitations [1], and even immunological biomarker abnormalities [2], [3]. It is also considered an important tool to monitor population health and has been shown to be an independent predictor of subsequent health events, including functional decline [4], physician visits [5] and hospital episodes [6]. Research during the past three decades has also documented the association between poor SRH and increased risk of mortality [7], [8], [9] across different cultures [7], [10] and age groups [5], [11], .
The majority of prior investigations on the association between SRH and mortality have relied on SRH measurement at one time point, despite the fact that SRH likely changes over the course of long follow-up periods. In studies of mortality, the assessment of SRH at just one point in time is likely to introduce bias toward the null because of non-differential misclassification. To overcome this bias some studies have treated SRH as a time-varying variable [13], [14], and found that time-varying SRH is more strongly related to mortality compared to baseline-only measurement of SRH. However, even in these studies SRH has been measured at just two time points. Longitudinal studies with repeated measures focusing on within-individual changes in SRH remain sparse and very few studies have presented trajectories of SRH in different population subgroups [15], [16], [17], [18], [19], [20]. In these studies, however, the aim has been to characterize the different profiles of SRH over time rather than to examine it in respect to certain outcome of interest, such as mortality.
A better understanding of SRH trajectories at the end of life potentially may help to shed light on the mechanisms linking age, SRH, chronic conditions and death. To examine this issue, we used data from the Health and Retirement Study (HRS), a longitudinal cohort study of retirement and health among a representative sample of older people in the United States. The extraordinarily rich and complex data with repeated measurements provides an opportunity to examine the trajectories of SRH during the 12 years prior to death in different age groups of men and women utilizing a nested case-control design. Such data also allowed our examination of the role of common risk factors and diseases in explaining the differences in SRH between deceased cases and surviving controls.
Methods
Study design and participants
The Health and Retirement Study (HRS) is an ongoing cohort study of Americans, with interview data collected biennially on demographics, health behavior, health status, employment, income and wealth, and insurance status. The first cohort was interviewed in 1992 and every two years subsequently, with 5 additional cohorts added in the phases between 1994 and 2010. The full details of the study are described elsewhere [21], [22].
In this study we focused on the HRS participants who died between 1998 and 2010 (n = 9,901, Figure 1). We restricted inclusion in the study to those who had at least two SRH measurements in the 12 years prior to death, one observation proximal (1–6 years) and one distal (7–12 years) prior to death (n = 5,673). To compare SRH trajectories of those who died to surviving participants we utilized a nested case-control design with deaths being the cases (n = 3,350) and randomly selected survivors (at least one, but three at most) serving as controls for each case (n = 8,127). Controls were matched for sex, baseline age (5-year groups), race (White/Caucasian, Black/African American and Other) and study cohort. The trajectory of SRH for each individual was traced backwards for 12 years and they also had to have one proximal and one distal SRH measurement. The analytic sample consisted of 1,622 men and 1,728 women who died at a mean age of 73.9 (SD 8.5) years and 75.9 (SD 10.0) years, respectively. On average, deceased cases provided data on SRH at 5.1 (SD 1.0) timepoints while surviving controls provided data at 5.1 (SD 1.1) of the possible 6 waves.
Figure 1. Flow chart of the study population.

* At least two self-rated health measurements in the 12 years prior to death, one proximal (1–6 years prior to death) and one distal (7–12 years prior to death).
Ethical approval
Ethical approval for the HRS Study was obtained from the University of Michigan Institutional Review Board and the study has been conducted according to the principles expressed in the Declaration of Helsinki. Since the interviews were conducted by telephone, all respondents are read a confidentiality statement when first contacted, and they give verbal consent by agreeing to do the interview. This consent procedure was approved by the ethic committee.
Measurement of self-rated health
At each study wave, the participants were asked to rate his or her health on a five-point scale ranging from 1 (excellent) to 5 (poor). For the purpose of this study SRH was dichotomized by categorizing response scores 1–3 (excellent, very good, good) as good health and scores 4–5 (fair and poor) as poor health. We used all available annual measurements in the 12-year timeframe before death.
Mortality outcome
Mortality data on all participants was available in the HRS database. The HRS procedure to confirm the death and the timing of a participant's death relies on proxy informants, matching to the Social Security Death Index as well as matching to the commercial Insight databases to determine the vital status of all participants. These death records are periodically validated with the gold standard National Death Index (NDI). HRS routinely confirms death dates against the NDI report by comparison with the proxy reported death dates. For deceased participants, the month and year of death are recorded in the database. In the analyses we included deaths between 1 January 1998 and 31st December 2010.
Covariates
There are two time-invariant variables: age at death and education. Age was categorized as 30–64 years, 65–79 years and ≥80 years. Education was categorized in three levels (low = less than high school, medium = high school or some college, and high = college and above). All other covariates were time-varying since they could change between study phases. Marital status was categorized as married/cohabiting, widowed and other possibilities. Non-housing financial wealth was divided into sex-specific tertiles.
Of the major risk factors, we had information on smoking, obesity and high blood pressure. Smoking status was defined as no, ex-smoker and current smoker. Body Mass Index (BMI) was calculated using reported height and weight, and categorized as normal weight BMI 18.5–24.9 kg/m2, overweight BMI 25–29.9 kg/m2, obese BMI≥30 kg/m2. High blood pressure was based on self-report of a doctor-diagnosed condition.
Chronic diseases were determined at each study wave by asking respondents: “Has a doctor ever told you that you have…?” Six chronic diseases were included: (1) heart disease (heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems), (2) stroke, (3) chronic lung disease (chronic bronchitis or emphysema), (4) cancer (cancer or a malignant tumor of any kind except skin cancer), (5) diabetes (diabetes or high blood sugar) and (6) psychiatric condition.
Statistical analysis
Characteristics of the study population are presented separately for men and women as well as by case and control status. Marital status and non-housing financial wealth are based on the last information prior to death for deceased cases and from the corresponding study phase for the surviving controls.
Trajectories of poor SRH in the 12 years preceding death were assessed using log-binomial regression analysis with generalized estimating equations (GEE) controlling for the intra-individual correlation between repeated measurements using an exchangeable correlation structure [23], [24], [25]. First, we plotted sex-specific SRH trajectories for all deceased cases and surviving controls. Second, we examined whether the trajectories were dependent on age groups and tested age group x time interaction terms for cases and controls. The interactions for deceased men (p<0.001) and women (p<0.001) were statistically significant and therefore the main results are shown by age groups.
To examine whether the prevalence of poor SRH among the deceased cases and surviving controls differed during the 12-year period, we compared their first (11–12 years before death) and last (1–2) SRH measurements. In addition, we also examined the change from first to last recorded SRH within cases and controls. The analysis was initially adjusted for education, wealth and marital status. The second set of models further adjusted for life-style related risk factors and the third set of models for chronic diseases. All covariates, except education, were used as time-varying using the closest available assessment corresponding to the self-reported health measurement. Results are presented as risk ratios (RR) and their 95% confidence intervals (CI).
Our sensitivity analysis addressed the possibility that including only those deceased participants for whom we could find an age, sex, race and cohort matched control may have affected the findings. We estimated the 12-year SRH trajectory by taking into account all those men and women who met the first inclusion criteria (one proximal and one distal SRH measurement (n = 5,089). The SAS 9.4 Statistical Package was used for all analyses (SAS Institute Inc., Cary, NC).
Results
Characteristics before death of deceased cases and surviving controls (selected from the same study wave) are shown in Table 1. The average age at death was 73.9 years among male and 75.9 years among female cases and the respective age of the controls were 73.1 years and 75.4 years. Age, sex, race and cohort matched controls had higher level education and non-housing wealth compared to deceased cases (p for all <0.0001). In addition, deceased women were more often married or cohabiting than their controls (p = 0.01).
Table 1. Characteristics Before Death Among Deceased Cases and Surviving Controls*.
| Men | Women | |||||
| Deceased cases | Surviving controls | p | Deceased cases | Surviving controls | p | |
| N | 1622 | 3827 | 1728 | 4300 | ||
| Age at death/last visit,% | 0.04 | 0.45 | ||||
| 30–64 | 13.0 | 13.8 | 12.9 | 13.6 | ||
| 65–79 | 59.9 | 62.3 | 49.0 | 49.9 | ||
| ≥80 | 27.1 | 23.9 | 38.2 | 36.5 | ||
| Race,% | 0.38 | 0.85 | ||||
| White | 80.6 | 82.1 | 77.7 | 78.3 | ||
| Black | 15.5 | 13.5 | 19.0 | 18.6 | ||
| Other | 3.9 | 3.8 | 3.3 | 3.1 | ||
| Education,% | <.0001 | <.0001 | ||||
| Less than high school | 39.1 | 30.2 | 41.3 | 30.8 | ||
| High school | 43.0 | 47.5 | 48.9 | 55.4 | ||
| College and above | 18.0 | 22.3 | 9.7 | 13.8 | ||
| Non-housing financial wealth,% | <.0001 | <.0001 | ||||
| Lowest tertile | 44.7 | 30.2 | 43.3 | 30.5 | ||
| Middle tertile | 28.2 | 32.6 | 29.5 | 32.4 | ||
| Highest tertile | 27.1 | 37.3 | 27.1 | 37.1 | ||
| Marital status,% | <.0001 | <.0001 | ||||
| Married or cohabiting | 71.9 | 79.9 | 38.1 | 47.2 | ||
| Widowed | 14.2 | 9.9 | 46.0 | 39.0 | ||
| Other possibilities | 13.9 | 10.2 | 15.9 | 13.9 | ||
* Characteristics are selected from the same study wave for cases and controls.
Figure 2 shows the trajectories of poor SRH in the 12 years preceding the death in deceased cases and surviving controls. In men and women, the prevalence of poor SRH across the 12-year period was higher among deceased cases compared to controls (p for all <0.0001). In deceased men, comparing their first SRH measurement (11–12) to their last SRH measurement (1–2), the prevalence of poor SRH doubled (RR 1.88, 95% CI 1.72–2.06). Among surviving controls the increment from first to last SRH measurement was 1.5-fold (RR 1.48, 95% CI 1.36–1.62). In women, the increment from first to last SRH measurement was slightly less than in men (cases RR 1.56, 95% CI 1.45–1.68 and controls RR 1.44, 95% CI 1.34–1.55). Compared to the surviving controls, the prevalence of poor SRH increased more steeply among male and female cases of all ages (interaction for age*group p<0.0001 for men and p = 0.01 for women).
Figure 2. Estimated prevalence with 95% confidence intervals of poor self-rated health during the 12 years prior to death in deceased cases and surviving controls.
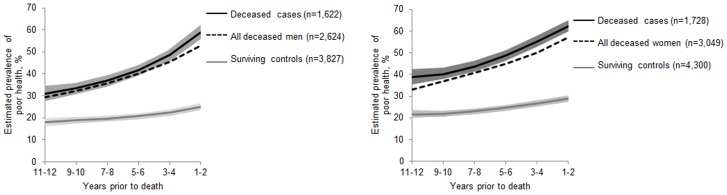
Panel A: men, Panel B: women. Dotted line indicates the trajectory for all deceased men/women in the HRS study with one proximal and one distal self-rated health measurement including also those who did not have a matched control.
For the sensitivity analysis Figure 2 also shows the trajectory of all deceased men and women who had one proximal and one distal SRH measurement including those who did not match to a control. The trajectory of all deceased men closely trailed the trajectory of deceased males fulfilling the case definition. The trajectory of all deceased women was slightly lower but parallel with the trajectory of deceased female cases. This was because many of the oldest participants did not anymore have surviving controls available. For those 2,323 cases who were excluded, due to not having a matched control, the average death age was 86.5 years among males and 89.5 among females.
Figure 3 shows the trajectories of poor SRH in the 12 years preceding the death among deceased cases and surviving controls in the three different age groups. In men and women, the prevalence of poor SRH across the 12-year period among cases was lowest among those aged 80 years and older, whereas among controls it was lowest among those aged 30–64 years. The risk ratios for poor SRH comparing deceased cases and surviving controls at 11–12 and 1–2 years prior to death are shown in Table 2 (men) and Table 3 (women). In men aged 65–79 and 80 years and older, those who subsequently died reported between a 1.5 to 2.0-fold higher prevalence of poor SRH already 12 years prior to death compared to their surviving controls (RR 1.92, 95% CI 1.66–2.24 and RR 1.48, 95% CI 1.15–1.92) (Table 2). Among men aged 30–64 years, there was no statistically significant difference in prior poor SRH comparing cases and controls (RR 1.61, 95% 0.93–2.81), but the association was significant two years later i.e. 10 years prior to death (RR 1.85, 95% 1.31–2.61). Adjustment for sociodemographic factors and lifestyle-related risk factors slightly attenuated the risk estimates, which were further attenuated after accounting for chronic diseases. In the fully adjusted model, the difference between cases and controls remained significant for both older age groups.
Figure 3. Estimated prevalence of poor self-rated health during the 12 years prior to death in deceased cases and surviving controls by age groups.

Panel A: men, Panel B: women.
Table 2. Risk Estimates (RR) and Their 95% Confidence Interval (CI) for Men's Poor Self-Rated Health Comparing Deceased Cases to Surviving Controls at 11–12 and 1–2 Years Prior to Death.
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
| Age group | RR | 95% CI | RR | 95% CI | RR | 95% CI | RR | 95% CI | ||||
| 30–64 years | ||||||||||||
| 11–12 years prior | 1.61 | 0.93 | 2.81 | n/a* | n/a | n/a | ||||||
| 1–2 years prior | 2.79 | 2.29 | 3.40 | n/a | n/a | n/a | ||||||
| 65–79 years | ||||||||||||
| 11–12 years prior | 1.92 | 1.66 | 2.24 | 1.76 | 1.52 | 2.04 | 1.71 | 1.48 | 1.99 | 1.49 | 1.29 | 1.71 |
| 1–2 years prior | 2.55 | 2.32 | 2.80 | 2.31 | 2.10 | 2.54 | 2.26 | 2.05 | 2.48 | 1.69 | 1.53 | 1.86 |
| ≥80 years | ||||||||||||
| 11–12 years prior | 1.48 | 1.15 | 1.92 | 1.42 | 1.10 | 1.82 | 1.40 | 1.09 | 1.80 | 1.28 | 1.01 | 1.64 |
| 1–2 years prior | 1.65 | 1.45 | 1.88 | 1.56 | 1.37 | 1.78 | 1.55 | 1.36 | 1.77 | 1.28 | 1.12 | 1.47 |
Notes: Model 1 is adjusted for age; Model 2 is additionally adjusted for education, wealth and marital status; Model 3 is additionally adjusted for BMI, smoking and blood pressure; Model 4 is additionally adjusted for heart disease, stroke, lung disease, cancer, diabetes, and psychiatric disease.
* model fails to converge.
Table 3. Risk Estimates (RR) and Their 95% Confidence Interval (CI) for Women's Poor Self-Rated Health Comparing Deceased Cases to Surviving Controls at 11–12 and 1–2 Years Prior to Death.
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
| Age group | RR | 95% CI | RR | 95% CI | RR | 95% CI | RR | 95% CI | ||||
| 30–64 years | ||||||||||||
| 11–12 years prior | 3.33 | 2.17 | 5.10 | 2.72 | 1.78 | 4.16 | 2.54 | 1.67 | 3.86 | 2.11 | 1.41 | 3.16 |
| 1–2 years prior | 2.84 | 2.37 | 3.41 | 2.32 | 1.93 | 2.78 | 2.12 | 1.77 | 2.54 | 1.54 | 1.28 | 1.85 |
| 65–79 years | ||||||||||||
| 11–12 years prior | 2.07 | 1.81 | 2.37 | 1.80 | 1.58 | 2.05 | 1.69 | 1.48 | 1.91 | 1.43 | 1.27 | 1.62 |
| 1–2 years prior | 2.38 | 2.18 | 2.60 | 2.07 | 1.89 | 2.26 | 1.97 | 1.80 | 2.16 | 1.46 | 1.33 | 1.61 |
| ≥80 years | ||||||||||||
| 11–12 years prior | 1.50 | 1.26 | 1.79 | 1.47 | 1.23 | 1.75 | 1.44 | 1.21 | 1.72 | 1.36 | 1.15 | 1.61 |
| 1–2 years prior | 1.59 | 1.43 | 1.76 | 1.54 | 1.39 | 1.70 | 1.53 | 1.38 | 1.69 | 1.30 | 1.17 | 1.44 |
Notes: Model 1 is unadjusted; Model 2 is adjusted for education, wealth and marital status; Model 3 is additionally adjusted for BMI, smoking and blood pressure; Model 4 is additionally adjusted for heart disease, stroke, lung disease, cancer, diabetes, and psychiatric disease.
In women aged 30–64 years those who died reported more than three times higher prevalence of poor SRH compared to surviving controls 12 years prior to death (RR 3.33, 95% CI 2.17–5.10) and the risk ratio remained relatively stable across the 10-year time period (Table 3). Among women aged 65–79 years and 80 years and older the risk ratios of mortality among those with poor SRH were between 1.5–2.0 fold higher, comparing cases and surviving controls. Adjustment for sociodemographic factors, lifestyle-related risk factors and chronic diseases attenuated but did not eliminate the observed differences between deceased cases and surviving controls in all age groups.
As expected, there was a marked difference between cases and controls in the prevalence of poor SRH in the wave immediately preceding death for both sexes (Table 2 and Table 3). However, the prevalence ratio of poor health was inversely related to age. Poor SRH was reported nearly three times more often by deceased men (RR 2.79, 95% CI 2.29–3.40) and women (RR 2.89, 95% CI 2.37–3.41) aged 30–64 compared to their surviving controls. The risk ratio was slightly lower in men and women aged 65–79 years and much lower among 80 years and older men (RR 1.65, 95% 1.45–1.88) and women (RR 1.59, 95% CI 1.43–1.76) compared to surviving controls. Adjustment for sociodemographic factors, lifestyle-related risk factors and chronic diseases attenuated but did not eliminate the observed differences between deceased cases.
Discussion
Our analysis of the individual-level repeat data from the US Health and Retirement Study provides two insights into the SRH trajectories prior to death in middle-aged and older US adults. First, those who died reported 1.5 to 3 times higher prevalence of poor SRH even 11–12 years prior to their death compared to their age, sex and race matched surviving controls. Large differences between deceased cases and surviving controls were observed among women dying at age of 30–64 years. Second, trajectories of poor SRH among deceased cases differed across age groups and sex, being lowest in men and women aged 80 years and older and highest in women aged 30–64 years. In surviving controls, poor SRH increased linearly with age, the prevalence being highest among those aged 80 years and older.
To examine factors that might explain the differences between deceased cases and surviving controls 12 years prior to death, we separately adjusted for lifestyle factors and chronic diseases. In men and women dying in 30–64 and 65–79 years of age, obesity, smoking and high blood pressure partly explained the observed difference. However, lifestyle factors had a minor role in the oldest age group. Further adjustment for chronic diseases explained large part of the difference between deceased cases and surviving controls in all age groups, but all risk estimates remained statistically significant even in the fully adjusted models. These results confirm earlier findings of the nature of SRH by capturing some unobserved factors predisposing to death in addition to clinically observed diseases and risk factors [2], [7], [26].
To our knowledge this is the first study to present age-related SRH trajectories 12 years prior to death for deceased cases and their surviving controls. In surviving controls the prevalence of poor SRH increased over time in all age groups, slightly more in the oldest age group, which is in accordance with the previously reported age-related SRH trajectories [27]. Interestingly, the trajectories of poor SRH among deceased cases and surviving controls were furthest apart for those aged 30–64 years and closest to each other in those in the oldest age group. This unexpected finding is most likely due to a selective survival bias at older ages, i.e. people with very poor SRH have already died prior to reaching age of 80 years. It is also possible that the level of expectations regarding “good” health decreases with age, and at any given level of SRH more health problems are tolerated [28].
SHR is a simple but comprehensive measure of global health and several other factors besides disease risk factors and comorbid diseases may determine people's perceptions as suggested by recent meta-analysis [29]. First, it is possible that SRH captures a wide array of mortality-related physiological and pathological characteristics, such as increased inflammation [2], [3], which we could not examine in this study. Moreover, it has been suggested that positive self-ratings reflect a general optimistic disposition to life. Good perceived health may be particularly important at more advanced ages when physical and psychological impairments are common [30]. Finally, SRH also captures some other “private” or unobserved characteristics that determine health status, such as family history, health behavior, pre-illness symptoms, as well as social and psychological resources [31], which may partly explain the differences observed already in the middle-aged group.
The main strengths of the study include the prospective longitudinal design with biennial information on SRH during 12 years of follow-up. The results can be generalized to the US adult population due to the nationally representative sample and because our inclusion criteria did not seem to cause bias in the SRH trajectories. In addition, by using the nested case-control design we were able to examine the “true” differences between SRH trajectories in deceased cases and surviving controls during 12-year time window since the matching took care of the confounding role of age, sex and race, which all are found to influence of SRH measurement.
The limitations of the study also need to be acknowledged. Our analysis examined the associations of SRH trajectories with all-cause mortality, since cause-specific mortality data was not available. Further studies are warranted to examine whether SRH trajectories differ according to causes of death. Second, the HRS ascertained a limited list of self-reported comorbid conditions, thus no information was available for many chronic illnesses such as Parkinson's disease which can impact on perceived health. It is also possible that we failed to capture prodromal illnesses (i.e. diagnoses of diseases which had not yet been confirmed by a physician at the time of answering the surveys).
To conclude, data from a population-based sample of US adults showed that men and women who subsequently die perceive their health worse already 11–12 years prior to death compared to their surviving controls. In clinical practice single-item SRH can serve as a comprehensive, patient-centered and inexpensive “screening” tool to identify persons at increased risk of deteriorating health and premature death.
Data Availability
The authors confirm that all data underlying the findings are fully available without restriction. The RAND HRS Data file is an open access data set based on the HRS data. It was developed at RAND with funding from the National Institute on Aging and the Social Security Administration. The research paper is based on the Health and Retirement Study (HRS). The data products are available without cost to registered users. More information can be found at (http://hrsonline.isr.umich.edu).
Funding Statement
This work was supported by the EU's Era-Age 2 program (Academy of Finland (264944) and the Swedish Research Council for Health, Working Life and Welfare (Forte, 2012-1661)). Mika Kivimäki is supported by a professorial fellowship from the Economic and Social Research Council. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Jylhä M, Guralnik JM, Balfour JB, Fried LP (2001) Walking Difficulty, Walking Speed, and Age as Predictors of Self-Rated Health: The Women's Health and Aging Study. Journal of Gerontology: Medical Sciences 56: M609–M617. [DOI] [PubMed] [Google Scholar]
- 2. Jylhä M, Volpato S, Guralnik JM (2006) Self-rated health showed a graded association with frequently used biomarkers in a large population sample. Journal of Clinical Epidemiology 59: 465–471. [DOI] [PubMed] [Google Scholar]
- 3. Cohen HJ, Pieper CF, Harris T, Rao KM, Currie MS (1997) The association of plasma IL-6 levels with functional disability in community-dwelling elderly. Journal of Gerontology: Biol Sci Med Sci 52: M201–M208. [DOI] [PubMed] [Google Scholar]
- 4. Idler EL, Kasl SV (1995) Self-ratings of health: do they also predict change in functional ability? J Gerontol B Psychol Sci Soc Sci 50: S344–353. [DOI] [PubMed] [Google Scholar]
- 5. Miilunpalo S, Vuori I, Oja P, Pasanen M, Urponen H (1997) Self-rated health status as a health measure: the predictive value of self-reported health status on the use of physician services and on mortality in the working-age population. J Clin Epidemiol 50: 517–528. [DOI] [PubMed] [Google Scholar]
- 6. Kennedy BS, Kasl SV, Vaccarino V (2001) Repeated hospitalizations and self-rated health among the elderly: a multivariate failure time analysis. Am J Epidemiol 153: 232–241. [DOI] [PubMed] [Google Scholar]
- 7. Idler EL, Benyamini Y (1997) Self-rated health and mortality: a review of twenty-seven community studies. Journal of Health and Social Behavior 38: 21–37. [PubMed] [Google Scholar]
- 8. Idler EL, Angel RJ (1990) Self-rated health and mortality in the NHANES-I Epidemiologic Follow-up Study. Am J Public Health 80: 446–452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Mossey JM, Shapiro E (1982) Self-rated health: a predictor of mortality among the elderly. Am J Public Health 72: 800–808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Jylhä M, Guralnik JM, Ferrucci L, Jokela J, Heikkinen E (1998) Is self-rated health comparable across cultures and genders? J Gerontol B Psychol Sci Soc Sci 53B: S144–S152. [DOI] [PubMed] [Google Scholar]
- 11. Grant MD, Piotrowski ZH, Chappell R (1995) Self-reported health and survival in the Longitudinal Study of Aging, 1984–1986. J Clin Epidemiol 48: 375–387. [DOI] [PubMed] [Google Scholar]
- 12. Larsson D, Hemmingsson T, Allebeck P, Lundberg I (2002) Self-rated health and mortality among young men: what is the relation and how may it be explained? Scand J Public Health 30: 259–266. [DOI] [PubMed] [Google Scholar]
- 13. Lyyra TM, Leskinen E, Jylha M, Heikkinen E (2009) Self-rated health and mortality in older men and women: a time-dependent covariate analysis. Arch Gerontol Geriatr 48: 14–18. [DOI] [PubMed] [Google Scholar]
- 14. Ferraro KF, Kelley-Moore JA (2001) Self-rated health and mortality among black and white adults: examining the dynamic evaluation thesis. J Gerontol B Psychol Sci Soc Sci 56: S195–205. [DOI] [PubMed] [Google Scholar]
- 15. Lee HL, Huang HC, Lee MD, Chen JH, Lin KC (2012) Factors affecting trajectory patterns of self-rated health (SRH) in an older population–a community-based longitudinal study. Arch Gerontol Geriatr 54: e334–341. [DOI] [PubMed] [Google Scholar]
- 16. Ayyagari P, Ullrich F, Malmstrom TK, Andresen EM, Schootman M, et al. (2012) Self-rated health trajectories in the African American health cohort. PLoS One 7: e53278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Sacker A, Worts D, McDonough P (2011) Social influences on trajectories of self-rated health: evidence from Britain, Germany, Denmark and the USA. J Epidemiol Community Health 65: 130–136. [DOI] [PubMed] [Google Scholar]
- 18. Sacker A, Wiggins RD, Bartley M, McDonough P (2007) Self-rated health trajectories in the United States and the United Kingdom: a comparative study. Am J Public Health 97: 812–818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Vahtera J, Westerlund H, Ferrie JE, Head J, Melchior M, et al. (2010) All-cause and diagnosis-specific sickness absence as a predictor of sustained suboptimal health: a 14-year follow-up in the GAZEL cohort. J Epidemiol Community Health 64: 311–317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Westerlund H, Kivimäki M, Singh-Manoux A, Melchior M, Ferrie JE, et al. (2009) Self-rated health before and after retirement in France (GAZEL): a cohort study. Lancet 374: 1889–1896. [DOI] [PubMed] [Google Scholar]
- 21.National Institute on Aging (2013) Growing older in America: The Health and Retirement Study.
- 22. Juster F, Suzman R (1995) An overview of the health and retirement study. J Hum Resour 30: S7–S56. [Google Scholar]
- 23. Zeger SL, Liang K-Y (1986) Longitudinal data analysis for discrete and continuous outcomes. Biometrics 42: 121–130. [PubMed] [Google Scholar]
- 24.Diggle PJ, Liang KY, Zeger SL (1994) Analysis of Longitudinal Data. Oxford, U.K: Oxford University Press.
- 25. Spiegelman D, Hertzmark E (2005) Easy SAS calculations for risk or prevalence ratios and differences. American Journal of Epidemiology 162: 199–200. [DOI] [PubMed] [Google Scholar]
- 26. Idler EL, Russell LB, Davis D (2000) Survival, functional limitations, and self-rated health in the NHANES I Epidemiologic Follow-up Study, 1992. First National Health and Nutrition Examination Survey. Am J Epidemiol 152: 874–883. [DOI] [PubMed] [Google Scholar]
- 27. Liang J, Shaw BA, Krause N, Bennett JM, Kobayashi E, et al. (2005) How does self-assessed health change with age? A study of older adults in Japan. J Gerontol B Psychol Sci Soc Sci 60: S224–232. [DOI] [PubMed] [Google Scholar]
- 28. Ferraro KF (1980) Self-ratings of health among the old and the old-old. Journal of Health and Social Behavior 21: 377–383. [PubMed] [Google Scholar]
- 29. Mavaddat N, Parker RA, Sanderson S, Mant J, Kinmonth AL (2014) Relationship of self-rated health with fatal and non-fatal outcomes in cardiovascular disease: a systematic review and meta-analysis. PLoS One 9: e103509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Boehm JK, Peterson C, Kivimaki M, Kubzansky L (2011) A prospective study of positive psychological well-being and coronary heart disease. Health Psychology 30: 259–267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Ostir GV, Markides KS, Black SA, Goodwin JS (2000) Emotional well-being predicts subsequent functional independence and survival. J Am Geriatr Soc 48: 473–478. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The authors confirm that all data underlying the findings are fully available without restriction. The RAND HRS Data file is an open access data set based on the HRS data. It was developed at RAND with funding from the National Institute on Aging and the Social Security Administration. The research paper is based on the Health and Retirement Study (HRS). The data products are available without cost to registered users. More information can be found at (http://hrsonline.isr.umich.edu).