

Abstract
Background
Amputation is one of the most common procedures in the practice of Orthopaedics and Traumatology in Nigeria. Many previous studies and reports from different centres show variations in the indications for this surgical procedure.
Aims & Objectives
The aim of this study is to find the most important indications for amputation in our immediate environment and make possible suggestions towards reducing the incidence.
Patients and Method
This is a retrospective study of consecutive patients who had limb amputations at the Central Hospital, Warri between January, 2009 and December, 2011. Case notes of patients were retrieved, relevant information extracted and analysed.
Results
A total of 44 patients had 46 amputations within the study period. The age range of patients was between 8-88 years. Amputation in 63.6% of the patients was due to diabetic foot disease, followed by trauma in 20.5% of cases. About (62.5%) of the amputations were below knee amputations while toe amputations made up 17.4% of cases. The lower limb was involved in 91% of cases and upper limbs in 9% of cases. Complication rate was about 39.1% which was mostly as a result of wound infections.
Conclusion
Diabetic foot disease was the most important indication for amputation in this study. Rigorous public enlightenment on the prevention and effective treatment of diabetes will reduce the incidence of lower limb amputations in this environment.
Keywords: Amputations, Diabetic foot disease, South-south Nigeria
Introduction
Limb amputation refers to the severance of part of a limb or a whole limb from the rest of the body. It may be post traumatic or surgical1. It is one of the commonest surgical procedures2.
In some patients, amputation is performed as a primary procedure because the patient’s limb condition is irreversible and must be removed in order to save that particular patient’s life3.
The decision to amputate a patient’s limb is often one of the most difficult one for the surgical team to make and a most trying period for the patient and his relations to give consent for the procedure. This is even more critical in our environment where amputees often become permanently handicapped and dependent due to the difficulties with accessing rehabilitative and prosthetic facilities. The loss of a limb thus, has profound economic, social and psychological effects on the patients and their families4. This had made some patients to discharge themselves against medical advice only to return in a moribund state.
The indications for amputation are generally considered as the 3Ds – Dead or Dying; Dangerous or Deadly; Damned nuisance5. In the developed world, most amputations are done due to peripherial vascular disease 3,5, while in developing countries, the main indications include: diabetic foot disease, trauma, malignancies and the complications of traditional bone setters’ treatment of musculoskeletal injuries. The extent to which any of these indications contribute vary from one environment to the other even in the same country or subregion3,4,6,7,8,9,10,11.
In Nigeria, most of the limb amputations are preventable through public enlightenment, good health care policies and the provision of affordable appropriate health care that patient could access on time. The aim of this study is to highlight the main indications for amputation in our environment and to make recommendations towards reducing the incidence.
Reports
PATIENTS & METHOD
This is a retrospective study of consecutive patients who had limb amputations at the Central Hospital, Warri, South-South Nigeria, from January, 2009 to December, 2011.
The case notes of patients were retrieved and data on age, sex, indications for amputation, affected limb, level of amputation and outcome were extracted and analyzed using the SPSS (Statistical Package for Scientific Solutions) version 17.
RESULTS
A total of 46 amputations were performed in the hospital during the study period involving 44 patients. There were 27 males and 17 females giving a male: female ratio of 1.6:1.
The age of the patients ranged from 8 to 88 years with a mean of 53.8 ± 18.3 years. The highest number of patients were in their seventh decade of life followed by those in their sixth decade as shown in Figure 1.
Diabetic foot disease was the commonest indication for amputation in this environment occurring in 28 (63.6%) of the patients followed by trauma in 9 (20.5%) as shown in Figure 2.
About 63% of the amputations were below knee amputations while 17% were toe amputations as shown in Figure 3.
About 91% of the patients had lower limb amputations while 9% involved the upper limbs. Of the 91% affecting the lower limbs, the right lower limb was involved in 17 cases (39%) while 23 (52%) of the cases involved the left lower limb. In the upper limbs, of the 9%, seven per cent involved the right and 2% the left as shown in Table 1.
The outcome of treatment is as shown in Table 2. Of the 46 amputations, 28 (60.9%) of the wounds healed primarily, while 18 (39.1%) developed complications which included wound infections in 13 (28.3%) patients and re-amputation in2 (4.3%). The mortality rate was 6.5%.
Fig. 1.
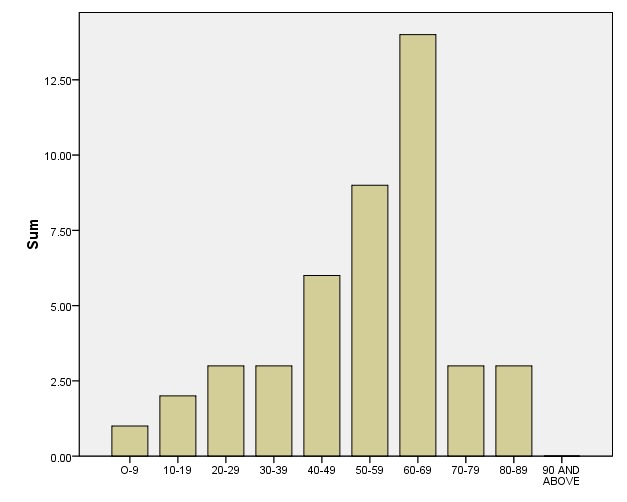
AGE DISTRIBUTION OF PATIENTS
Fig. 2 .
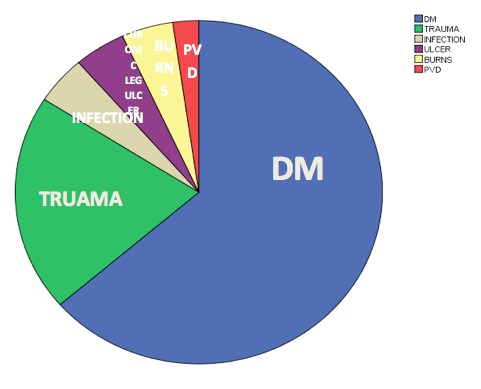
INDICATIONS FOR AMPUTATION (PVD = PERIPHERIAL VASCULAR DISEASE; DM = DIABETES MELLITUS)
Fig. 3.
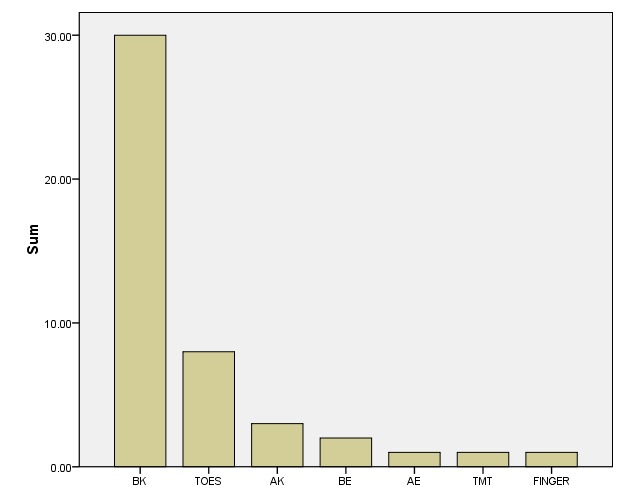
LEVELS OF AMPUTATION (BK = BELOW KNEE; AK = ABOVE KNEE; BE = BELOW ELBOW; AE = ABOVE ELBOW; TMT = TRANSMETATARSAL)
TABLE 1. SHOWING LIMB INVOLVEMENT & LATERALITY
| RIGHT | LEFT | TOTAL | |
| LOWER LIMBUPPER LIMBTOTAL | 17 (39%)3 (7%)20 (45.5) | 23 (52%)1 (2%)24 (54.5) | 40 (91%)4 (9%)44 (100%) |
TABLE 2. SHOWING OUT COME OF AMPUTATION SURGERIES
| OUTCOME | NO. OF PATIENTS/SURGERIES | PERCENTAGE OF TOTAL |
| PRIMARY WOUND HEALINGWOUND BREAKDOWN/INFECTIONRE-AMPUTATION (BK to AK)DIEDTOTAL | 28132346 SURGERIES | 60.9%28.3%4.3%6.5%100% |
Conclusions
Diabetic foot disease was the most important indication for amputation in this study. Rigorous public enlightenment on the prevention, and effective treatment of diabetes will reduce the incidence of lower limb amputations in this environment.
Discussion
The indications for amputation varies from one environment to the other, from one region to the other and is changing with time even within the same locality 2,3,4,6,7,10,12,13,14,15,16.
In nearly all the previous series reviewed, there is a male preponderance for amputations, although the ratio varies from one environment to the other. This study is in keeping with this pattern. There were 27 (61%) males and 17 (39%) females in this study giving a male to female ratio of 1.6:1. This is similar to the findings of 1.4:1 by Naeder16 in Ghana but at variance with 2.8:1 recorded by Ofiaeli3 in Southeast Nigeria and Dada & Awoyomi7 in Southwest Nigeria. Jawaid et al4 in Pakistan reported a ratio of 6.6:1. Although the trend is not quite distinct, a closer look at these studies reveals that the male : female ratio tends to be lower in environments where diabetic foot disease and peripherial vascular are the major indications for amputation and higher where trauma and traditional bone setters treatment complications are the main indications for amputations. This may be due to the fact that trauma is a more common event in males than females as males are more adventurous and are involved more in physical exertions.
The age range in this study varied from 8-88 years with a mean of 53.8+18.3 years. Ofiaeli3 in Eastern Nigeria obtained a similar average of 54.4 years. Lower age averages were obtained in Lagos (47.6 years)7, Pakistan (47.45+13.2 years)4 and Malaysia (39.7 years)13 while a higher one of 70 years was obtained at Korle-Bu hospital in Ghana16. More than 50% of the amputees in this study were in their 6th and 7th decades of life. Dada et al in Lagos, Nigeria also reported similar peak incidence at the 6th decade followed by the 7th decade in their study. Common to these two studies is the fact that diabetic foot complication ranked the commonest indication for amputation as opposed to lower peak ages in other studies were trauma and traditional bone setter complication10,12,17 were the most common indications. Type II diabetes mellitus was the cause for most of the foot complications which tend to manifest clinically in later years which explains the older peak age while trauma is commoner in younger active adults respectively.
In a review of several studies in Nigeria over a 15 year period, Thanni et al6 reported 34% of amputations to be due to trauma and 23% due to the complications of traditional bone setters (TBS) treatment, malignancies in 14.5% and diabetic foot disease in 12.3%. The same authors also reported some variations in the indications from region to region within the same country.
Twenty eight (63.6%) of the patient s in this study had amputations due to diabetic complications making diabetic foot disease the commonest indication for amputation.
Of particular note however is the fact most of the studies that reported diabetic complications as the leading indication for amputation3,4,7, were more recent. This increasing importance of diabetic foot as a cause for limb amputation in the developing world, has both clinical and socioeconomic implications which need to be addressed in order to ameliorate the problem. The effect of diabetic mellitus and its complications are usually more pronounced among the poor socioeconomic group who most times could not afford the cost treatment and regular check-ups needed for good glycaemic control.
Furthermore, some authors 3,7 also reported very poor use of prosthesis in this environment due to financial reason.
Educating diabetic patients on foot care has been shown to reduce the incidence of diabetic foot complications7,11,18. Ikem et al 19 advocated the routine use of the 507/10g Semmes-Weinstein monofilament as an instrument to routinely detect diabetic neuropathies with appropriate education on foot care.
These measures will help to reduce amputations due to diabetic foot complications and consequently save resources in the health sector.
Other less common indications for amputation in this study include: electric burns, chronic leg ulcer and peripherial vascular disease as highlighted under results. Of note in this study is that traditional bone setter complication was not recorded as an indication for amputation. This contrasts with the report by Umaru and others17 in Maiduguri Northeast Nigeria that traditional bone setters complication was the commonest indication for amputation in their study. The difference in methods of splinting injured limbs between the traditional bone setters in that part of the country and other areas has been implicated as possible explanation for this contrasting observation17.
Below knee amputation was carried out in 65% of the patients in this study. This agrees with findings of other workers3,7. It however contrasts with the findings of Umaru and others in Maiduguri17 who reported above knee amputation as the commonest in their centre.
Three of the patients in this study died post operatively giving a mortality rate of about 7% all of whom were diabetic . This mortality rate is lower when compared with 15.2% reported by Ofiaeli3 and 16% by Dada et al7. It is however, higher than the 1.9% reported by Jawaid et al4 in Karachi, Pakistan. This low mortality rate as reported was attributed to good glycaemic control and monitoring during the postoperative period. It has also been shown that meticulous surgical technique and good post-operative nursing care produce better outcome3.
The 30% infection rate observed in this study is quite comparable with the thirty six per (36%) overall infection rate reported in South-east Nigeria3 and 31.4%7 reported in Lagos, Southwest Nigeria.
Footnotes
Competing Interests: The authors have declared that no competing interests exist.
Grant support: None
References
- 1.Amputation and Amputation Surgery www.vascular,co.nz>amputation surgery.
- 2.Obalum DC, Okeke GC. Lower Limb Amputations at a Nigerian Private Hospital. West Afr J med. 2009;28(1):24–27. doi: 10.4314/wajm.v28i1.48420. [DOI] [PubMed] [Google Scholar]
- 3.Ofiaeli RO. Indications, Levels and Outcome of Lower Extremity Amputations In Nnewi, Nigeria. JOMIP. 2001;2(5):18–21. [Google Scholar]
- 4.Jawaid M, Ali I, Kaimkanni GM. Current Indications For Lower Limb Amputations At Civil Hospital Karachi, Pakistan. Journal Of Surgery. 2008;24(4):228–231. [Google Scholar]
- 5.Solomon L, Warwick DJ, Nayagam S. Arnold Edward., editor. Appley System of Orthopaedics And Fractures. 8 2001. pp. 267–267.
- 6.Thanni LOA, Tade AO. Extremity Amputations In Nigerian. A Review Of Indications And mortality. . Surgeon. 2007;5(4):213–217. doi: 10.1016/s1479-666x(07)80006-0. [DOI] [PubMed] [Google Scholar]
- 7.Dada AA, Awoyomi BO. Is The Trend Of Amputation In Nigeria changing?A Review of 51 Consecutive Cases Seen At The Federal Medical Centre, Ebute Metta, Lagos, Nigeria. Niger J Med. 2010;51(4):167–169.. [Google Scholar]
- 8.Olasinde AA, Oginni LM, Bankole JO, Adegbehingbe OO, Oluwadiya KS. Indications for Amputations In Ile-Ife, Nigeria. Niger J Med. 2002 Jul-Sep;11(3):118–121. [PubMed] [Google Scholar]
- 9.Yakubu A, Muhammad I, Mabogunje CA. Major Limb Amputations In Adults, Zaria, Nigeria. J R Coll Surg Eding. 1996;41(2):102–104.. [PubMed] [Google Scholar]
- 10.Akiode A, Shonubi AMO, Musa A, Sule G. Major Limb Amputations: An Audit Of Indications In A Sub-urban Surgical Practice. J Nat Med Association. 2005;;97:74–78. [PMC free article] [PubMed] [Google Scholar]
- 11.Obimbo JA, King’ori J. Pattern Of Limb Amputation In A Kenyan Rural Hospital. Intern Orthop. 2009;33(5):1449–1453. doi: 10.1007/s00264-009-0810-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Abbas AD, Musa AM. Changing Pattern Of Extremity Amputations In University Of Maiduguri Teaching Hospital, Nigeria. Niger J Med. 2007;16(4):330–333. doi: 10.4314/njm.v16i4.37332. [DOI] [PubMed] [Google Scholar]
- 13.Hazmy W, Muhamad M, Ashikin N, Jamilah S, Yee LE, Shong HK. Major Limb Amputations In Serebian Hospital:A Review Of 204 Cases From 1997-1999. Med J Malaysia. 2001;3(7):56–56. [PubMed] [Google Scholar]
- 14.Akinyoola AL, Oginni LM, Adegbehingbe OO, Orimolade EA, Ogundele OJ. Causes of Limb Amputations In Nigerian Children. West Afr J Med. 2006; 25.(4):273–275. [PubMed] [Google Scholar]
- 15.Ekere AU. The Scope of Extremity Amputations In A Private Hospital In South-South Region of Nigeria. Niger J Med. 2003. Oct-Dec;14(4):24–27. [PubMed] [Google Scholar]
- 16.Naader SB. Amputations of The Lower Limbs In Korle-Bu Teaching Hospital, Accra. West Afr.J Med. 1993;12:21–26. [PubMed] [Google Scholar]
- 17.Umaru RH, Gali BM, Ali N. The Role of Inappropriate Traditional Splintage In Limb Amputation In Maiduguri, Nigeria. Annals of African Medicine. 2004;3(3):138–140. [Google Scholar]
- 18.Viswanathan, V Kumpatha. Pattern And Causes Of Amputation In Diabetic Patients A Multi-centric Study From India. JAPI. 2011;59:148–151. [PubMed] [Google Scholar]
- 19.Ikem RT, Ikem IC. Screening And Identifying Diabetic Patients A Risk Of Foot Ulceration. Use of Semes Weinstein Monofilament. Diabetes International. 2009;. pp. 15–17.