

Abstract
Objective: To describe a quick and simple diagnostic approach to monocular diplopia.
Background: Diplopia is a common visual complain in casualty departments, general practice clinics, neurologic clinics as well as ophthalmic clinics. Monocular diplopia, however, is uncommon. Many well established clinical examination methods are available to address diplopia. Some require special equipments which are not easily available or unfamiliar outside of ophthalmic clinic. We describe a simple two-minute diagnostic approach to monocular diplopia.
Conclusion: Basic knowledge and understanding of simple clinical examination techniques enhances diagnostic skill and allow proper localization of underlying disorders.
Keywords: Monocular diplopia, metamorphopsia, pinhole, red reflex
INTRODUCTION
Diplopia is a common visual complain in casualty departments, general practice clinics, neurologic clinics as well as ophthalmic clinics. The causes of diplopia are multitude and can range from simple benign refractive error to life threatening intracranial aneurysm. As with any neurologic complains, localization is the foremost task in the management of diplopia. Monocular diplopia, however, is uncommon and presents a diagnostic challenge to most general practitioners. In order to make things simpler for the busy practitioners, we describe a simple two-minute diagnostic approach to monocular diplopia.
Pathophysiology of diplopia
Diplopia or double vision is the visualization of object in two different spatial locations. Diplopia can occur during monocular viewing (monocular diplopia) or binocular viewing (binocular diplopia). Monocular diplopia occurs when two images are viewed by a single eye. Monocular diplopia can result from three conditions; light diffraction, metamorphopsia and cerebral polyopia. The fovea consists solely of cone photoreceptors and is responsible for fine vision and colour vision. Other parts of the retina (extra-foveal retina) are responsible for peripheral vision. Light diffraction causes images of a single object to fall on the fovea and the extra-foveal retina of the same eye. The images are of different clarity, with the extra-foveal ghost-image overlapping the clear foveal image. Monocular diplopia due to light diffraction resolves with viewing through a pinhole (Figure 1).1 Metamorphopsia or distortion of retinal images is due to maculopathies such as macular edema or epiretinal membrane. Metamorphopsia is frequently reported as double vision. A good historian will be able to distinguish between the two, but this can sometimes be difficult. Metamorphopsia does not resolve with viewing through a pinhole. Cerebral polyopia is the perception of multiple images due to pathologies in occipital cortex or central visual pathway lesions. Monocular diplopia occurs bilaterally, the images are of equal clarity and do not overlap.2
Figure 1.

Monocular diplopia due to light diffraction resolved with pinhole
Under normal circumstances, when a person looks at a three-dimensional object, images form on the fovea of both eyes. The left eye sees slightly more detail on the left side and vice versa. This causes a slight horizontal retinal image disparity. Fusion of the two disparate retinal images by the occipital cortex results in binocular single vision and stereopsis (binocular sensation of relative depth). Cortical fusion only occurs if the disparate images fall on certain area of subjective visual space, the Panum’s area. Images outside the Panum’s area are too disparate to be fused cortically into single image, and will be perceived as diplopia.
Binocular diplopia is due to misalignment of the visual axes. Images fall on non-corresponding parts of both retinas. Image falls on the fovea of the fixating eye and extra-foveal retina in the non-fixating eye. Both images fall outside the Panum’s area of single binocular vision, the object will be seen as having two different spatial locations in the subjective space, hence diplopia.3 The foveal image is clearer than the extra-foveal image. The separation of both images is greatest when the object is viewed in the direction of the field-of-action of the paretic extra-ocular muscle.
The two-minute approach to monocular diplopia
The initial approach is to determine whether the diplopia is monocular or binocular (Figure 2). This is achieved by first presenting a target to the patient with both eyes open to confirm the presence of diplopia. The right eye is then covered, followed by the left eye. In binocular diplopia, the double vision resolves with either eye covered. In monocular diplopia, the double vision persists when the good eye is covered and disappears when the affected eye is covered. If double vision persists when either eye is covered, one should consider the presence of cerebral polyopia. Psychogenic diplopia due to inorganic causes should always be a diagnosis of exclusion.
Figure 2.

Flowchart for monocular diplopia
Once unilateral monocular diplopia is confirmed, the next step is to ask the patient to view an object through a pinhole to differentiate those caused by light diffraction from those caused by maculopathies (Table 1). Diplopia due to light diffraction will resolve with pinhole, but those due to maculopathies will persist. The causes of light diffraction include refractive errors and ocular media abnormalities. Examples of refractive errors are high ametropia and irregular astigmatism. Mechanical compression on the cornea caused by eyelid tumors can cause irregular astigmatism. Tear film abnormalities, corneal opacities and irregularities, cataract, abnormal lenticular shapes, ectopia lentis, extra-pupillary openings and vitreous opacities can all lead to light diffraction.
Table 1. Causes of monocular diplopia.
| Anatomic location | Causes |
|---|---|
| Refractive error | High refractive error, irregular astigmatism; Edge effect of spectacle or contact lens |
| Eyelid | Mechanical compression on cornea chalazion, tumor, hematoma, edema |
| Tear film | Abnormalities of tear film causing light diffraction mucus strand, foreign bodies, oil droplets |
| Cornea | Opacity causing light diffraction: scar, edema, corneal dystrophies; Abnormal corneal shape: keratoconus, keratoglobus, megalocornea; Post refractive surgery |
| Lens | Opacity: cataract, vacuoles, water cleft; Shape: lenticonus, spherophakia; Position: ectopia lentis, intraocular lens subluxation |
| Iris and pupil | Iridodialysis, polycoria, peripheral iridotomy / iridectomy |
| Vitreous | Foreign bodies |
| Retina | Macular edema; Central serous retinopathy |
| Cerebral polyopia | Trauma, migraine, multiple sclerosis, encephalitis, seizure |
The direct ophthalmoscope is an efficient instrument but unfortunately underused by most practitioners. The direct ophthalmoscope will differentiate light diffraction caused by refractive error, media opacities and media irregularities as well as diplopia due to macular pathologies. Binocular red reflex test is performed by viewing the red reflex of both eyes simultaneously. If red reflex of the affected eye is slightly paler than the unaffected eye, the presence of retinal detachment must be entertained and urgent referral is indicated. Relative afferent pupillary defect (RAPD) is usually positive in the presence of retinal detachment large enough to cause a pale red reflex. If the red reflexes are asymmetrical with one eye brighter than the other, anisometropia is usually present. This can be confirmed by using the focusing dial of the direct ophthalmoscope as one focuses on the optic disc.
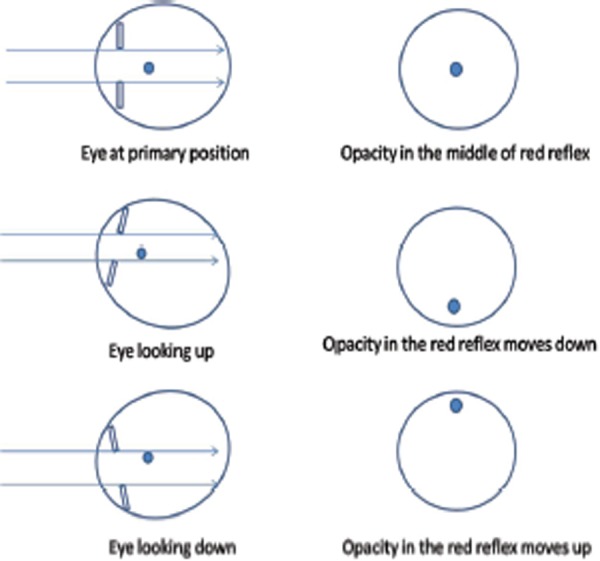
If opacity is detected within the red reflex, the location of the media opacity within the globe can be located by asking the patient to look up and down. If the opacity moves up as the patient looks up, and moves down as the patient looks down, the opacity is situated in front of the pupillary plane (Figure 3). If the opacity moves in opposite direction, the opacity is located behind the pupillary plane (Figure 4). If the opacity does not move with eye movement, it is located at the pupillary plane (Figure 5).
Figure 3.

Movement of opacity in red reflex for media opacity in front of pupillary plane
Figure 4.
Movement of opacity in red reflex for media opacity behind the pupillary plane
Figure 5.

No movement of opacity in red reflex for media opacity in the pupillary plane
Oil droplet red reflex appears as a dark circle within the red reflex. Oil droplet red reflex is seen in keratoconus and lenticonus. The area of curvature change causes light rays to be projected away from the examiner’s eye, leaving a dark circle in the red reflex. The presence of keratoconus is confirmed by positive Munson sign where there is bulging of the lower lid in downgaze. Lastly, the direct ophthalmoscope is used to examine the macula for any maculopathies.
Limitations
The two-minute approach to monocular diplopia is intended as a quick screening test for initial localization of pathologies.
Using four easily available equipment (an occluder, a pinhole, a direct ophthalmoscope and a target), the causes of monocular diplopia can be localized with relative ease and accuracy. It is not intended to replace comprehensive evaluation by ophthalmologists.
CONCLUSION
Basic knowledge and understanding of simple examination techniques enhances diagnostic skill and allow proper identification of underlying disorders.
Footnotes
Conflicts Of Interest
None
Contributor Information
AK Tan, MD.
HA Faridah, MS(UKM).
Less than one-third of diabetics in the health clinic have good nutrition knowledge
Lim CJ, Suzana S, Hanis Mastura Y, et al. Level of nutritional knowledge and health awareness among diabetes mellitus patients at Cheras Health Clinic, Kuala Lumpur, Malaysia. Sains Malaysiana. 2010;39(3):505-11.
http://pkukmweb.ukm.my/~jsm/pdf_files/SM-PDF-39-3-2010/24%20Lim%20Ching.pdf
132 diabetic patients at Cheras Health Clinic were evaluated for their nutrition knowledge. The majority of the respondents had poor glycaemic control (93.6%). Overall, 37.1% respondents were categorized as having poor nutrition knowledge, followed by 31.8% moderate and only 31.1% good.
Home glucose monitoring may not be cost-effective for diabetics managed without insulin
Cameron C, Coyle D, Ur E, Klarenbach S. Cost-effectiveness of self-monitoring of blood glucose in patients with type 2 diabetes mellitus managed without insulin. Can Med Assoc J. 2010;182(1):28-34.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2802601/pdf/1820028.pdf
This cost-effective analysis concluded that: For most patients with type 2 diabetes not using insulin, use of blood glucose test strips for frequent self-monitoring (e•7 times per week) is unlikely to represent efficient use of finite health care resources, although periodic testing (e.g. 1 or 2 times per week) may be cost effective. Reduced test strip price would likely also improve cost-effectiveness.
References
- 1.Elkington AR, Frank HJ. 2nd ed. Oxford: Blackwell Science; 1991. Clinical optics; p. 98. [Google Scholar]
- 2.Norton JW, Corbett JJ. Visual perceptual abnormalities: hallucinations and illusions. Semin Neurol. 2000;20((1)):111–21. doi: 10.1055/s-2000-6837. [DOI] [PubMed] [Google Scholar]
- 3.San Francisco: American Academy of Ophthalmology; 2007. American Academy of Ophthalmology. 2007-2008 Basic science and clinical course; p. 52. Section 5: Pediatric ophthalmology and strabismus. [Google Scholar]