

Abstract
AIM: To identify the anthropometric, metabolic and mood state in hepatitis C virus (HCV)-infected patients from the west of Mexico and to evaluate the effect of Breathwalk (BW), a combination of walking, synchronized breathing and focussed attention, on those patients.
METHODS: In an experimental study, 17 patients with serological and molecular diagnosis of HCV, not receiving pharmacological treatment, were studied. One hour sessions of BW were practiced 3 times at week for six months. Body composition was assessed by electric impedance. Biochemical profiles and insulin resistance (IR) risk was assessed by conventional methods. Mood state was evaluated with specific and open questions at the beginning and at the end of the program.
RESULTS: Seventy percent of patients were overweight or obese, and 77% of the patients presented with IR at the beginning of the study. Improvements were observed at the 3rd mo, and statistically significant differences were recorded at the 6th mo using the fitness score (76 vs 83, P < 0.01), in alanine aminotransferase (ALT) (106 ± 93 U/L vs 59 ± 32 U/L, P < 0.01), total bilirubin (0.09 ± 1 mg/dL vs 0.62 ± 0.2 mg/dL, P < 0.01), ALT/AST ratio (1.04 vs 0.70, P < 0.01), triglycerides (165 ±86 mg/dL vs 124 ± 49 mg/dL, P < 0.01) and the IR risk (4.0 vs 2.7). Most patients (88%) indicated to feel better at the end of BW (P < 0.01).
CONCLUSION: Breathwalk has an important effect on body composition, lipid profile and liver enzymes. It is also easy, inexpensive and has a beneficial effect on metabolic and mood state in HCV patients.
Keywords: Breathwalk, Chronic hepatitis C, Insulin resistance, Obesity, Quality of life
INTRODUCTION
It has been estimated that hepatitis C virus (HCV) has infected more than 170 million people globally and is responsible for up to 70% of all viral chronic infections[1]. Furthermore, obesity, type 2 diabetes (DM2) and insulin resistance (IR) are current health problems that especially affect chronic HCV patients[2-6]. The occurrence of obesity is an additional risk factor that can further deteriorate the health condition of chronic hepatitis C patients[7], with increased insulin resistance[8] and potential development of diabetes and progression to liver fibrosis[9,10]. Also, poor quality of life related to changes in mood, emotional state, and depressions are common findings among chronic HCV patients[11,12]. This is mainly attributed to the impact of the diagnosis and subsequent anxiety over long-term health[12]. This situation may limit the tolerability of antiviral treatment and reduce compliance[11], together with the fact that HCV patients with excess body weight are known to be poor responders to antiviral therapy in comparison to normal-weight individuals[13,14]. Therefore, it is important to search for additional therapeutic strategies focused on lifestyle habits in chronic HCV patients that can contribute to improve metabolic and liver function as well as better quality of life.
Conventional therapeutic interventions for chronic HCV patients are primarily focused on antiviral regimens with minor attention on lifestyle modifications[15]. For instance, in the past and up to date, it has been stated that patients diagnosed with liver cirrhosis regardless of the stage must remain in a resting state or maintain minimal physical activity. Even when exercise and/or physical activity is a common therapeutic modality recommended for obese, DM2 and IR patients[16,17], studies related to the modality and strategy of exercise that could be beneficial for the patients with chronic liver disease are limited[18]. Breathwalk (BW) is a novel exercise strategy that is different from conventional walking, in fact it synchronizes walking steps with specific breath patterns and mental sustained attention[19].
Since obesity and IR are dependent on genetic and environmental factors of each population, the identification of such variables and implementation of specific strategies are necessary in order to achieve a better quality of life and response to antiviral treatments. The aim of the present study was to measure anthropometric and metabolic parameters as well as the mood state in HCV-infected patients from the west of Mexico and to evaluate the effect of BW on those parameters.
MATERIALS AND METHODS
Patients
In an experimental study, 22 patients with chronic hepatitis C infection attending the Gastroenterology and Molecular Biology in Medicine Departments at the Civil Hospital of Guadalajara were included. Molecular and serological diagnosis of HCV was performed as described before[20]. All patients had serologic and molecular diagnosis (PCR) of chronic hepatitis C virus and were not receiving interferon or any other specific treatment. The Civil Hospital of Guadalajara is one of the biggest public hospitals in Mexico that mainly attends low income patients that have no other social health security. Due to the cost of interferon, the low income level and the large number of patients with HCV attending the hospital, most of them do not receive specific pharmacological treatment.
Patients with HCV infection without interferon treatment were invited to participate in the program. Only those volunteers who signed a written consent were included. Clinical evaluations involved identification of the stage of the disease through Child-Pugh score. Patients with decompensated hepatic disease and/or Child C were not included. Twenty two patients remained until after the third month of the program. At this time period, an important improvement was registered, however 5 patients did not continue and dropped out because of the following reasons: two patients were from out of the city and returned to their villages, one patient felt better and decided not to further attend and 2 more patients did not show up. The protocol was conducted in accordance with the Helsinki declaration and with approval by the ethical committee of the hospital.
Body composition
Body composition was measured by electric impedance technique (In Body 3.0, Biospace, Inc). Patients were indicated to fast at least 8 h, to not carry out any type of exercise 5 d before evaluation and to empty the bladder and bowels before testing[21,22]. The parameters evaluated in body composition were body mass index BMI (kg/m2), percentage of fat and muscle, waist circumference (WC) and fitness score. Patients were classified for risk of metabolic complications associated with obesity, according to WC. High risk of cardiovascular disease was marked at 94 cm of WC for men and 80 cm for women according to WHO[23]. Also the Official Mexican Norm for the classification of BMI[24] was used.
Biochemical profile
Blood samples for measurement of the biochemical profile were obtained after an overnight fast (12 h minimum). The biochemical profile included lipid profile [total cholesterol, triglycerides, high density lipoprotein (HDL), low density lipoprotein (LDL)], liver function tests aspartate amine transferase (AST), alanine amine transferase (ALT), total bilirubin, glucose and insulin. Routine biochemical test were performed by the use of manual enzymatic assays (Human Gessellschaft für Biochemica und Diagnostica mbH, Germany). Insulin levels were detected by microparticle enzyme immunoassay (Abbott Laboratories, North Chicago, IL). Insulin resistance was measured by the homeostasis model of assessment (HOMA)[25,26] and/or the triglycerides/high-density lipoprotein (TG/HDL) ratio[27].
Evaluation of mood state
Initially and at the end of the BW program, an interview was carried out with specific questions in order to assess the patients’ mood regarding their illness during this intervention as described elsewhere[28,29]. Also, an interview was performed with two questionnaires. The first had two types of questions: open and with multiple option answers related to negative and positive mood states. One open question was: How is your mood state actually? Options for positive mood state were: Happy, calm, good in general and negative mood options were: angry, nervous, anguished, fear, bad in general.
The second questionnaire asked specific questions like: “Have you reduced the time spent in your job or other activities?” “Have you been done less of what you like to do?” “Have you done your job or others activities carelessly?” These specific questions had a transformed score after evaluation. Patients were scored in four categories: excellent (100 points), good (66.66 points), regular (33.33) and bad (0 points).
Breathwalk protocol
Breathwalk is an exercise strategy that consists basically of walking with different synchronized breath patterns enhanced with a meditative episode[19]. Physical movements in BW are combined aerobic and resistance exercises. The first and basic tool is a conscious complete deep breathing. While inhaling in a rhythmic and flowing way, air is taken from the stomach and directed smoothly towards the thoracic chest and it finishes in a lightly upward movement of the clavicle and the superior part of the chest. While exhaling, all movements are inverted. This breathing pattern is continually practiced throughout the BW session.
The one hour session is composed of five steps. During the first 10 min, the participant began with a series of specific movements to warm up both arm and leg muscles and to relax the entire body, complete deep breathing as described above, in a synchronized pattern with body movements and was mentally focus on breathing. The following 5 min were dedicated to mentally scan the body posture while walking consciously and breathing patterns were continually synchronized. In the next 25 min, the participant was engaged in a quicker walking rhythm in which inhaling and exhaling patterns are performed at different intervals and combined with silently short-repeated phrases. The walking episode was concluded in the next 5 min by gradually reducing the walking pace. In the final remaining time, a new series of resistance exercises were initiated together with stretching and concluded with an episode of meditative visualization. The physical activity of BW was imparted by a qualified doctor trained in this program. Patients practiced a 1 h session of BW, three times a week for 6 mo.
Statistical analysis
Data and statistical analysis only of the 17 patients that remained until the end of the program were included. Numeric data was grouped by mean ± SD and minimum and maximum as indicated. Results at 3 and 6 mo of the program were compared against the basal using the non-parametric Wilcoxon rank test. A P value less than < 0.05 was considered statistically significant.
RESULTS
Demographic and clinical characteristics of HCV patients that participated in the BW program are shown in Table 1. A higher proportions of women than men is in agreement with the frequency of HCV in the west of Mexico as reported before[30,31]. Normal weight was present only in 29.4% of the patients, overweight in 17.6% and obesity in 53%. Five patients had cirrhosis and the rest had fibrosis and liver steatosis. Waist circumference was 84.9 ± 10.0 cm in women and 97.6 ± 11.6 cm in men. Waist circumference above 80 cm for women and more than 90 cm for men is considered a risk factor for the development of type 2 diabetes mellitus and/or insulin resistance in Mexico[24].
Table 1.
Demographic and clinic characteristics of patients with HCV infection at the beginning of the breathwalking (BW) program
| Parameter | HCV group | Reference range |
| n = 17 | ||
| Age (yr) | 51 ± 10.2 | - |
| Sex F/M (%) | 11/6 (65/35) | - |
| DM2 (%) | 3 (18) | - |
| BMI (kg/m2) | 27.6 ± 3.2 | < 25 |
| Waist circumference (cm) | 88.0 ± 10.4 | < 80 cm F, < 94 cm M |
| Fat percentage (mean) | 32.3 ± 7.1 | < 28% F, < 20% M |
| Soft lean mass (kg) | 44.2 ± 7.9 | - |
| Glucose (mg/dL) | 94.0 ± 16.5 | < 110 |
| ALT (U/L) | 106.7 ± 93.1 | < 55 |
| AST (U/L) | 101.4 ± 66.6 | < 40 |
| Cholesterol (mg/dL) | 157.1 ± 35.0 | < 200 |
| Triglycerides (mg/dL) | 165.0 ± 86.5 | < 160 |
| HOMA ratio | 3.7 ± 1.8 | < 2.5 |
| Metabolic syndrome (%) | 10 (59) | 1 |
DM2: Type 2 diabetes mellitus; BMI: Body mass index; ALT: Alanine aminotransferase; AST: Aspartate aminotransferase; F: Female; M: Male; HOMA: Homeostasis model of assessment.
NCEP (National cholesterol education program) ATP III (adult treatment panel III) 2001/2 criteria from metabolic syndrome.
Type 2 diabetes was present in 18% of the patients studied, whereas dyslipidemia was in 41.1%. Two patients had isolated hypercholesterolemia and 5 presented with isolated hypertriglyceridemia. Insulin resistance as determined by the HOMA index was present in 77% of the participants.
Anthropometric measurement in HCV patients at baseline, 3rd and 6th mo of the program are shown in Table 2. In spite of minimal changes in body weight, a reduction in BMI and waist circumference was observed during the program period, as well as a statistically significant increase in the fitness score (P < 0.001) at the 3rd and 6th mo.
Table 2.
Anthropometric measurements in chronic HCV patients at start, 3 and 6 mo of breathwalking (BW) intervention
| Parameter | Unit of parameter | Basal | 3 mo | 6 mo |
| Weight | kg | 69.1 ± 11.0 | 68.2 ± 10.8 | 68.4 ± 10.4 |
| BMI | kg/m2 | 27.6 ± 3.3 | 26.7 ± 3.6 | 26.5 ± 3.0a |
| Fat | % | 32.3 ± 7.1 | 31.6 ± 7.1b | 31.5 ± 6.6a |
| Muscle | kg | 44.2 ± 7.9 | 45.3 ± 9.4 | 45.2 ± 9.4 |
| WC | cm | 88.0 ± 10.4 | 87.2 ± 10.0 | 86.0 ± 9.4b |
| Fitness | Score | 76.0 ± 13.4 | 81.0 ± 3.0b | 83.0 ± 2.6d |
P < 0.05,
P < 0.01,
P < 0.001 between baseline and 3 or 6 mo.
An improvement in the lipid profile and liver function tests was observed during the BW program (Table 3). A statistically significant reduction in triglycerides was detected at 6th mo (P < 0.01). This reduction was associated with a statistically significant decrease of the TG/HDL ratio. Improvement in liver function tests was documented by a statistically significant decrease in bilirubin (P < 0.01) and ALT serum levels after six months (P < 0.01), as well as in the ratio ALT/AST (P < 0.01).
Table 3.
Biochemical profile in chronic HCV patients at start, 3 and 6 mo of breathwalking (BW) (mean ± SD)
| Biochemical parameter | Basal | 3 mo | 6 mo |
| Glucose (mg/dL) | 94.0 ± 16.5 | 93.5 ± 21.8 | 87.2 ± 12.3 |
| (77-128) | (71-142) | (75-121) | |
| ALT (U/L) | 106.6 ± 93.1 | 82.8 ± 63.4 | 59.4 ± 32.7b |
| (18-349) | (20-241) | (17-112) | |
| AST (U/L) | 101.4 ± 66.6 | 87.8 ± 61.8 | 84.7 ± 61.8 |
| (32-265) | (20-226) | (24-241) | |
| ALT/AST ratio | 1.04 | 0.94 | 0.70b |
| Total bilirubin (mg/dL) | 1.38 ± 1.2 | 1.22 ± 1.1 | 0.62 ± 0.36b |
| (0.30-5.2) | (0.29-4.9) | (0.0-1.1) | |
| Cholesterol (mg/dL) | 157.1 ± 86.5 | 148.0 ± 38.4 | 146.0 ± 39.8 |
| (103-231) | (82-217) | (67-205) | |
| Triglycerides (mg/dL) | 165.0 ± 86.5 | 141.9 ± 46.4 | 124.6 ± 49.2b |
| (86-378) | (85-210) | (64-197) | |
| TG/HDL ratio | 4.0 | 3.9 | 2.7a |
Data are expressed in mean ± SD. TG/HDL: Triglycerides/high density lipoprotein.
P < 0.05,
P < 0.01 between baseline and 3 or 6 mo.
Viral load was documented only in 7 patients at the beginning and at the end of the BW program. A reduction of the viral load was detected in 4 patients; from 78 667 ±50 000 copies baseline levels to 600 ± 0 at the end of BW intervention. Patients that showed an improvement in the viral load had HCV genotype 1b, 2a, 2c and 3. In the other three patients no changes in viral load were detected.
At the beginning of the program, 47% of the HCV patients expressed negative mood states (depression, anger, anguish, fear). At mo 6 of BW, 94% of the patients presented with positive mood states (Figure 1). At the end of BW, the patients report improved emotional state (P < 0.001) compared with the beginning in all categories (Table 4). In general, the majority of the patients were motivated towards physical activity, optimistic towards life, and they referred being happy.
Figure 1.
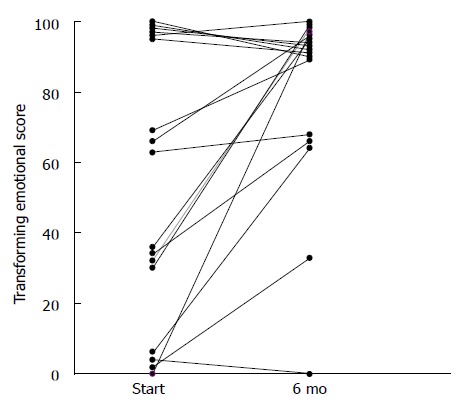
Patients’ mood state with respect to disease at the beginning (start) and at the end of breathwalk (BW) after 6 mo. Wilcoxon rank test. P < 0.01 between start and 6 mo.
Table 4.
Mood state based on transformed score evaluation at start, 3 and 6 mo of breathwalking (BW)
| Mood state category | Transformed score | Baseline | 3 mo | 6 mo |
| n (%) | n (%)b | n (%)b | ||
| Excellent | 100 | 6 (35) | 11 (65) | 15 (88) |
| Good | 66.66 | 3 (18) | 5 (29) | 1 (6) |
| Regular | 33.33 | 4 (23.5) | 0 (0) | 1 (6) |
| Bad | 0 | 4 (23.5) | 1 (6) | 0 (0) |
Wilcoxon rank test;
P < 0.001 between start and 3 or 6 mo.
DISCUSSION
Obesity and DM2 are an epidemiological problem worldwide, associated with changes in lifestyle. Traditional homeland dietary and physical activity habits have shifted to a mixture of occidentalized and traditional diets combined with more sedentary life. Therefore, the extent of obesity and DM2 in HCV infected patients could be expected to vary in each continent or country mainly due to the diversity of race and environmental factors present in the population. More than fifty percent of the adults are overweight or obese in Mexico[32], and the association of HCV infection with obesity, which by itself is associated with insulin resistance[33], feasibly explains why 77% of the studied patients presented with IR at the time of the study. Hypercholesterolemia and hypertriglyceridemia were the two main dyslipidemia present in 41% of the participants. Indeed, hypertriglyceridemia has been associated with insulin resistance and development of DM2[34]. Therefore, a further rise in DM2 incidence could be expected in these HCV-infected patients in a near future. This reinforces the need to establish specific strategies based on lifestyle changes in order to prevent further metabolic abnormalities or deterioration of liver function.
In order to analyze the effect of BW on lipid profile, only patients that did not vary their dietetic habits during the program were evaluated. A statistically significant decrease in triglycerides at mo 6 of the program was observed as well as the decrease of the TG/HDL ratio. Therefore, BW had an important effect on both types of dyslipidemia and IR without a dietary intervention as seen in other studies[16,17,35]. However, the inclusion of an individualized dietetic program considering their own culture and specific habits could exert a further decrease on dyslipidemia and BMI.
The BW intervention achieved an important effect on the fitness score with a statistically significant increase at 3 mo of the program. The fitness score is an impedance measurement that reflects the muscle/fat ratio, which explains the lack of significant changes in weight, especially during the initial weeks or month of the exercise.
It has been shown that walking requires a longer time period to exert its beneficial effect on lipid metabolism in obese and patients with DM2[36,37]. An advantage that BW has over conventional walking is that it is an aerobic exercise where the patients maintain up to 70% VO2max through rhythmic walking, and during the same session resistance exercise is included and associated with mental attention. Furthermore, it has been shown that anaerobic exercise (exercise load), which could be harmful for the patient with chronic liver disease, does not have significant effect on lipid metabolism at shorter periods of time[38].
An important effect of BW on liver function was also observed in HCV-infected patients. A statistically significant decrease of ALT, the ratio ALT/AST and total bilirubin was detected at mo 6 of the program as well as a decrease of the viral load in four of seven patients, where RNA-HCV was quantified at the beginning and at the end of the program. Little is known about the physiopathological mechanism related to the effect of exercise on the improvement of liver function tests in patients with chronic liver disease. However, even when it is known that exercise can improve insulin resistance at the cellular level[39], it can be speculated that a decrease in fatty liver would cause less liver injury, although further studies are required in order to determine any proposed mechanism. Also, the small number of analyzed patients with changes in viral load may only indicate the importance of performing further studies with this approach, primarily in those patients that have not responded to antiviral treatment[14] either because of the virus genotype[40] or as a secondary effect of the interferon by itself[41].
At the beginning of the program, only 12% of the patients reported a positive mood state, however, negative mood state shifted towards a positive mood score in 88% of the patients at the end. Most studies focus on analyzing the effect of exercise on metabolic parameters, yet it is unusual to evaluate the emotional state of the patients[42]. The observed significant change in mood state and therefore in quality of life may be attributed to the synchronized breathing patterns combined with walking throughout the BW routine. A meditative state of mind is provoked that allows disconnection from the external environment and liberates negative thought and feeling[43]. Another important factor that may have contributed to the results in this study is the fact that, throughout the six-month program, a close relationship was established between the instructor and the patients. This could have enhanced compliance and adherence of the patients to exercise and therefore to the changes in habits.
The fact that in the past and even in current days exercise has been controindicated in patients with chronic liver disease appears to be proven wrong, since in this study, chronic HCV patients with fibrosis and compensated cirrhosis improved in their metabolic and hepatic profiles at the end of the program. This approach is important because it can be incorporated as a complementary treatment in patients who are candidates for interferon treatment including non-responder patients. However, further studies should be continued to evaluate the effect of an integrative management of the patient that includes antiviral treatment, specific types of exercise, diet and mood state.
In conclusion, this study identifies a specific effect of BW on anthropometric, metabolic and liver functional tests, and demonstrates the importance of the patient’s mood state to enhance compliance to the program. Furthermore, this approach could be used in patients living in developing countries, where the cost of the antiviral treatment is expensive and in the mean time government authorities and/or international institutions can aid with financial funding to treat these patients.
ACKNOWLEDGMENTS
We thank Daniel Quezada for his laboratorial and technical support and kind attention to this work and Teresa Salcedo for the typing of the manuscript.
COMMENTS
Background
In the last few years, two different issues have been on top of the table in the hepatology field: the association of obesity and type 2 diabetes in patients infected with hepatitis C virus versus the traditional medical indication of resting in patients with chronic liver disease and, on the other hand, the current problem of the nonresponder patient to antiviral treatments, especially in those who are overweight or obese.
Research frontiers
Whereas it is clear that an increase in physical activity and/or specific exercises are indicated in overweight, obese and type 2 diabetes patients, there are few studies related to the effect of exercise on metabolic and hepatic function parameters in patients with liver disease and even to further approach patient’s emotions and well-being. Such strategy intends to involve different research areas so to achieve an integrative evaluation of patients that includes the study of metabolic parameters, liver function tests, emotional state, diet and exercise that are otherwise accessed in an individual manner.
Innovations and breakthroughs
This study represents an initial attempt to use Breathwalk as a specific technique in chronic liver disease patients, and to test in the near future the effect of different physical activity and exercise strategies on metabolic, liver function and anthropometric parameters, as well as emotional states in these patients.
Applications
Breathwalk is an innovative exercise technique that is easy to perform which could be implemented as a tool for patients with chronic liver diseases, especially at early stages of disease and in other chronic pathological conditions such as obesity, metabolic syndrome and type 2 diabetes.
Terminology
Breathwalk: An exercise technique that synchronizes walking steps, specific breathing patterns and focused attention. No-responders: Patients who do not achieve to lower viral loads after administration of the standard doses of antiviral monotherapy or combination therapy after (months) treatment.
Peer review
The manuscript studies the impact of breathwalking exercise on metabolic and fitness paramters in patients with chronic hepatitis C infection. It is interesting and of possible relevance to the field.
Footnotes
Supported by Grant Salud-Conacyt-2004-C01-025 to AP
S- Editor Zhu LH L- Editor Kremer M E- Editor Liu Y
References
- 1.Hussain SA, Ferry DR, El-Gazzaz G, Mirza DF, James ND, McMaster P, Kerr DJ. Hepatocellular carcinoma. Ann Oncol. 2001;12:161–172. doi: 10.1023/a:1008370324827. [DOI] [PubMed] [Google Scholar]
- 2.Petit JM, Bour JB, Galland-Jos C, Minello A, Verges B, Guiguet M, Brun JM, Hillon P. Risk factors for diabetes mellitus and early insulin resistance in chronic hepatitis C. J Hepatol. 2001;35:279–283. doi: 10.1016/s0168-8278(01)00143-x. [DOI] [PubMed] [Google Scholar]
- 3.Mason AL, Lau JY, Hoang N, Qian K, Alexander GJ, Xu L, Guo L, Jacob S, Regenstein FG, Zimmerman R, et al. Association of diabetes mellitus and chronic hepatitis C virus infection. Hepatology. 1999;29:328–333. doi: 10.1002/hep.510290235. [DOI] [PubMed] [Google Scholar]
- 4.Yazicioglu G, Isitan F, Altunbas H, Suleymanlar I, Ozdogan M, Balci MK, Karayalcin U. Insulin resistance in chronic hepatitis C. Int J Clin Pract. 2004;58:1020–1022. doi: 10.1111/j.1742-1241.2004.00170.x. [DOI] [PubMed] [Google Scholar]
- 5.Koike K. Hepatitis C virus infection can present with metabolic disease by inducing insulin resistance. Intervirology. 2006;49:51–57. doi: 10.1159/000087263. [DOI] [PubMed] [Google Scholar]
- 6.Zekry A, McHutchison JG, Diehl AM. Insulin resistance and steatosis in hepatitis C virus infection. Gut. 2005;54:903–906. doi: 10.1136/gut.2004.059873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Uauy R, Albala C, Kain J. Obesity trends in Latin America: transiting from under- to overweight. J Nutr. 2001;131:893S–899S. doi: 10.1093/jn/131.3.893S. [DOI] [PubMed] [Google Scholar]
- 8.Narita R, Abe S, Kihara Y, Akiyama T, Tabaru A, Otsuki M. Insulin resistance and insulin secretion in chronic hepatitis C virus infection. J Hepatol. 2004;41:132–138. doi: 10.1016/j.jhep.2004.03.020. [DOI] [PubMed] [Google Scholar]
- 9.Wang CS, Wang ST, Yao WJ, Chang TT, Chou P. Hepatitis C virus infection and the development of type 2 diabetes in a community-based longitudinal study. Am J Epidemiol. 2007;166:196–203. doi: 10.1093/aje/kwm061. [DOI] [PubMed] [Google Scholar]
- 10.Hui JM, Sud A, Farrell GC, Bandara P, Byth K, Kench JG, McCaughan GW, George J. Insulin resistance is associated with chronic hepatitis C virus infection and fibrosis progression [corrected] Gastroenterology. 2003;125:1695–1704. doi: 10.1053/j.gastro.2003.08.032. [DOI] [PubMed] [Google Scholar]
- 11.Forton DM, Taylor-Robinson SD, Thomas HC. Cerebral dysfunction in chronic hepatitis C infection. J Viral Hepat. 2003;10:81–86. doi: 10.1046/j.1365-2893.2003.00416.x. [DOI] [PubMed] [Google Scholar]
- 12.Strauss E, Dias Teixeira MC. Quality of life in hepatitis C. Liver Int. 2006;26:755–765. doi: 10.1111/j.1478-3231.2006.01331.x. [DOI] [PubMed] [Google Scholar]
- 13.Bressler BL, Guindi M, Tomlinson G, Heathcote J. High body mass index is an independent risk factor for nonresponse to antiviral treatment in chronic hepatitis C. Hepatology. 2003;38:639–644. doi: 10.1053/jhep.2003.50350. [DOI] [PubMed] [Google Scholar]
- 14.Walsh MJ, Jonsson JR, Richardson MM, Lipka GM, Purdie DM, Clouston AD, Powell EE. Non-response to antiviral therapy is associated with obesity and increased hepatic expression of suppressor of cytokine signalling 3 (SOCS-3) in patients with chronic hepatitis C, viral genotype 1. Gut. 2006;55:529–535. doi: 10.1136/gut.2005.069674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Strader DB, Wright T, Thomas DL, Seeff LB. Diagnosis, management, and treatment of hepatitis C. Hepatology. 2004;39:1147–1171. doi: 10.1002/hep.20119. [DOI] [PubMed] [Google Scholar]
- 16.Cuff DJ, Meneilly GS, Martin A, Ignaszewski A, Tildesley HD, Frohlich JJ. Effective exercise modality to reduce insulin resistance in women with type 2 diabetes. Diabetes Care. 2003;26:2977–2982. doi: 10.2337/diacare.26.11.2977. [DOI] [PubMed] [Google Scholar]
- 17.Ross R, Janssen I, Dawson J, Kungl AM, Kuk JL, Wong SL, Nguyen-Duy TB, Lee S, Kilpatrick K, Hudson R. Exercise-induced reduction in obesity and insulin resistance in women: a randomized controlled trial. Obes Res. 2004;12:789–798. doi: 10.1038/oby.2004.95. [DOI] [PubMed] [Google Scholar]
- 18.Hickman IJ, Clouston AD, Macdonald GA, Purdie DM, Prins JB, Ash S, Jonsson JR, Powell EE. Effect of weight reduction on liver histology and biochemistry in patients with chronic hepatitis C. Gut. 2002;51:89–94. doi: 10.1136/gut.51.1.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bhajan Y, Singh-Khalsa G. Breathwalk: Breathing Your Way to a Revitalized Body, Mind and Spirit. Broadway, New York: Random House Inc; 2000. pp. 1–306. [Google Scholar]
- 20.Rivas-Estilla AM, Sanchez LV, Matsui O, Campollo O, Armendáriz BJ, Segura-Ortega J, Panduro A. Identification of Hepatitis C virus (HCV) genotypes in infected patients from the west of Mexico. Hepatol Res. 1998;12:121–130. [Google Scholar]
- 21.Segal KR. Use of bioelectrical impedance analysis measurements as an evaluation for participating in sports. Am J Clin Nutr. 1996;64:469S–471S. doi: 10.1093/ajcn/64.3.469S. [DOI] [PubMed] [Google Scholar]
- 22.Lukaski HC, Bolonchuk WW, Siders WA, Hall CB. Body composition assessment of athletes using bioelectrical impedance measurements. J Sports Med Phys Fitness. 1990;30:434–440. [PubMed] [Google Scholar]
- 23.Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1995;854:1–452. [PubMed] [Google Scholar]
- 24.Secretaria de Salud. Norma Oficial Mexicana NOM 174-SSA-1-1998 para el manejo integral de la obesidad. (In Spanish). Online publication Diario Oficial de la Federación, 2000-04-12, cited 2007-03-19; screens. Available from: http: //www.salud.gob.mx/unidades/cdi/nom/174ssa18.html.
- 25.Tuan CY, Abbasi F, Lamendola C, McLaughlin T, Reaven G. Usefulness of plasma glucose and insulin concentrations in identifying patients with insulin resistance. Am J Cardiol. 2003;92:606–610. doi: 10.1016/s0002-9149(03)00735-5. [DOI] [PubMed] [Google Scholar]
- 26.Acosta AM, Escalona M, Maiz A, Pollak F, Leighton F. [Determination of the insulin resistance index by the Homeostasis Model Assessment in a population of Metropolitan Region in Chile] Rev Med Chil. 2002;130:1227–1231. [PubMed] [Google Scholar]
- 27.McLaughlin T, Abbasi F, Cheal K, Chu J, Lamendola C, Reaven G. Use of metabolic markers to identify overweight individuals who are insulin resistant. Ann Intern Med. 2003;139:802–809. doi: 10.7326/0003-4819-139-10-200311180-00007. [DOI] [PubMed] [Google Scholar]
- 28.Ferguson RJ, Robinson AB, Splaine M. Use of the reliable change index to evaluate clinical significance in SF-36 outcomes. Qual Life Res. 2002;11:509–516. doi: 10.1023/a:1016350431190. [DOI] [PubMed] [Google Scholar]
- 29.Durán-Arenas L, Gallegos-Carrillo K, Salinas-Escudero G, Martínez-Salgado H. [Towards a Mexican normative standard for measurement of the short format 36 health-related quality of life instrument] Salud Publica Mex. 2004;46:306–315. doi: 10.1590/s0036-36342004000400005. [DOI] [PubMed] [Google Scholar]
- 30.Chiquete E, Panduro A. Low prevalence of anti-hepatitis C virus antibodies in Mexico: A systematic review. Intervirology. 2007;50:1–8. doi: 10.1159/000096306. [DOI] [PubMed] [Google Scholar]
- 31.Florez H, Ryder E, Campos G, Fernandez V, Morales LM, Valbuena H, Rincón E, Gómez ME, Raleigh X. Women relatives of Hispanic patients with type 2 diabetes are more prone to exhibit metabolic disturbances. Invest Clin. 1999;40:127–142. [PubMed] [Google Scholar]
- 32.Olaiz-Fernández G, Rivera-Dommarco J, Shamah-Levy T, Rojas R, Villalpando-Hernández S, Hernández-Avila M, Sepúlveda-Amor J. Encuesta Nacional de Salud y Nutrición 2006. Cuernavaca Morelos, México: Instituto Nacional de Salud Pública; 2006. pp. 1–132. Available from: http: //www.insp.mx/ensanut/ensanut2006.pdf. [Google Scholar]
- 33.Weinman SA, Belalcazar LM. Hepatitis C: a metabolic liver disease. Gastroenterology. 2004;126:917–919. doi: 10.1053/j.gastro.2003.01.001. [DOI] [PubMed] [Google Scholar]
- 34.Båvenholm PN, Kuhl J, Pigon J, Saha AK, Ruderman NB, Efendic S. Insulin resistance in type 2 diabetes: association with truncal obesity, impaired fitness, and atypical malonyl coenzyme A regulation. J Clin Endocrinol Metab. 2003;88:82–87. doi: 10.1210/jc.2002-020330. [DOI] [PubMed] [Google Scholar]
- 35.Sreenivasa Baba C, Alexander G, Kalyani B, Pandey R, Rastogi S, Pandey A, Choudhuri G. Effect of exercise and dietary modification on serum aminotransferase levels in patients with nonalcoholic steatohepatitis. J Gastroenterol Hepatol. 2006;21:191–198. doi: 10.1111/j.1440-1746.2005.04233.x. [DOI] [PubMed] [Google Scholar]
- 36.Kraus WE, Torgan CE, Duscha BD, Norris J, Brown SA, Cobb FR, Bales CW, Annex BH, Samsa GP, Houmard JA, et al. Studies of a targeted risk reduction intervention through defined exercise (STRRIDE) Med Sci Sports Exerc. 2001;33:1774–1784. doi: 10.1097/00005768-200110000-00025. [DOI] [PubMed] [Google Scholar]
- 37.Poirier P, Després JP. Exercise in weight management of obesity. Cardiol Clin. 2001;19:459–470. doi: 10.1016/s0733-8651(05)70229-0. [DOI] [PubMed] [Google Scholar]
- 38.Kraus WE, Houmard JA, Duscha BD, Knetzger KJ, Wharton MB, McCartney JS, Bales CW, Henes S, Samsa GP, Otvos JD, et al. Effects of the amount and intensity of exercise on plasma lipoproteins. N Engl J Med. 2002;347:1483–1492. doi: 10.1056/NEJMoa020194. [DOI] [PubMed] [Google Scholar]
- 39.Duncan GE, Perri MG, Theriaque DW, Hutson AD, Eckel RH, Stacpoole PW. Exercise training, without weight loss, increases insulin sensitivity and postheparin plasma lipase activity in previously sedentary adults. Diabetes Care. 2003;26:557–562. doi: 10.2337/diacare.26.3.557. [DOI] [PubMed] [Google Scholar]
- 40.Myers RP, Poynard T. Interferon for interferon nonresponding and relapsing patients with chronic hepatitis C. Cochrane Database Syst Rev. 2002:CD003617. doi: 10.1002/14651858.CD003617. [DOI] [PubMed] [Google Scholar]
- 41.Sleijfer S, Bannink M, Van Gool AR, Kruit WH, Stoter G. Side effects of interferon-alpha therapy. Pharm World Sci. 2005;27:423–431. doi: 10.1007/s11096-005-1319-7. [DOI] [PubMed] [Google Scholar]
- 42.Lee S, Kuk JL, Davidson LE, Hudson R, Kilpatrick K, Graham TE, Ross R. Exercise without weight loss is an effective strategy for obesity reduction in obese individuals with and without Type 2 diabetes. J Appl Physiol (1985) 2005;99:1220–1225. doi: 10.1152/japplphysiol.00053.2005. [DOI] [PubMed] [Google Scholar]
- 43.Lazar SW, Bush G, Gollub RL, Fricchione GL, Khalsa G, Benson H. Functional brain mapping of the relaxation response and meditation. Neuroreport. 2000;11:1581–1585. [PubMed] [Google Scholar]