

Abstract
Background
Prevention intervention trials have been conducted to reduce risk of sexual transmission among people living with HIV/AIDS (PLWHA), but the findings were inconsistent. We performed a systematic review and meta-analysis to evaluate overall efficacy of prevention interventions on unprotected vaginal or anal intercourse (UVAI) among PLWHA from randomized clinical trials (RCTs).
Methods
RCTs of prevention interventions among PLWHA published as of February 2012 were identified by systematically searching thirteen electronic databases. The primary outcome was UVAI. The difference of standardized mean difference (SMD) of UVAI between study arms, defined as effect size (ES), was calculated for each study and then pooled across studies using standard meta-analysis with a random effects model.
Results
Lower likelihood of UVAI was observed in the intervention arms compared with the control arms either with any sexual partners (mean ES: −0.22; 95% confidence interval [CI]: −0.32, −0.11) or with HIV-negative or unknown-status sexual partners (mean ES and 95% CI: −0.13 [−0.22, −0.04]). Short-term efficacy of interventions with ≤10 months of follow up was significant in reducing UVAI (1–5 months: −0.27 [−0.45, −0.10]; 6–10 months: −0.18 [−0.30, −0.07]), while long-term efficacy of interventions was weaker and might have been due to chance (11–15 months: −0.13 [−0.34, 0.08]; >15 months: −0.05 [−0.43, 0.32]).
Conclusions
Our meta-analyses confirmed the short-term impact of prevention interventions on reducing self-reported UVAI among PLWHA irrespective of the type of sexual partner, but did not support a definite conclusion on long-term effect. It is suggested that booster intervention sessions are needed to maintain a sustainable reduction of unprotected sex among PLWHA in future risk reduction programs.
Introduction
People who find out that they are HIV-positive may reduce their sexual and drug using behaviors, but some may continue to have difficulties with changing their risk sexual and drug using behaviors [1]. Interventions targeted towards HIV-infected individuals to reduce their risk behaviors, referred to as “positive prevention”, could be a cost-effective strategy for reducing HIV transmission [2], [3], [4]. Positive prevention has three complementary objectives in HIV-infected individuals: (1) reducing high risk sexual behaviors; (2) reducing injection and non-injection drug and alcohol abuse, where relevant; and (3) optimizing clinical care [5]. The last objective seeks to: (i) foster linkage and retention of HIV-infected persons to good care; (ii) enhance coverage and adherence to antiretroviral therapy (ART); (iii) increase full suppression of HIV viral load; and (iv) prevent development of HIV drug resistance [6], [7].
Sexual transmission, via unprotected heterosexual or homosexual contact, is the leading cause of HIV acquisition [8], [9]. Many behavioral intervention programs have been implemented for reducing unprotected sexual intercourse, but findings from these studies have been inconclusive due to heterogeneous methods [10], [11], [12], [13], [14]. Intervention components and behavioral theories have varied, populations have differed, and intensity of interventions has been heterogeneous. However, we believe it is important to assess whether across interventions, there is any overall impact of these risk reduction programs. We fully acknowledge that an intervention applied in the most strategic way in the most receptive population is optimal, but a robust prevention strategy might be revealed if diverse approaches can be demonstrated efficacious in their aggregate. A meta-analysis is warranted for the efficacy of positive prevention to generate summary outcomes from these individual studies, acknowledging their diversity in theory, method, and population, but recognizing their similarity in purpose.
An earlier meta-analysis of 12 RCTs from 1988-2004 suggested that risk reduction interventions targeting people living with HIV/AIDS (PLWHA) were efficacious in reducing 43% of self-reported unprotected sex [15]. However, several additional trials of interventions for changing sexual behaviors among PLWHA have been published in recent years [11], [12], [13], [14], [16], [17], [18], [19], [20], [21], [22], [23], [24]. Two other previous reviews of prevention interventions also reported a similar increase of condom use, but these reviews included HIV-negative individuals [25] and studies without control arms [3]. We want to provide an updated review and meta-analysis of RCTs evaluating the efficacy of prevention intervention on unprotected vaginal or anal intercourse (UVAI) among PLWHA.
Methods
Literature search and study selection
Our review complies with preferred reporting items for systematic reviews and meta-Analyses (PRISMA) [26], [27]. A systematic literature search was performed to identify RCTs that evaluated the impact of prevention interventions on self-reported UVAI among PLWHA, published by February 2012. Thirteen electronic databases were searched: AMED (Allied and Complementary Medicine Database, Ovid Technologies), British Library Direct, British Nursing Index (Ovid Technologies), Centre for Reviews and Dissemination databases (including DARE and NHS EED), Cochrane Library (including the Health Technology Assessment database and ENTRAL), EMBASE (Elsevier), EconLit (The American Economic Association), ERIC (Education Resources Information Centre), Ovid Medline (Ovid Technologies), PsycINFO (American Psychological Association), Scopus (Elsevier), Web of Science (Thomson Scientific Technical Support), and Global Health Library Virtual Platform (World Health Organization). Our search strategy was: (HIV-infected OR HIV-positive OR HIV-seropositive OR people living with HIV/AIDS OR AIDS OR Acquired Immunodeficiency Syndrome) AND (behavior therapy OR behavioral intervention OR risk reduction intervention OR prevention intervention OR treatment adherence OR patient compliance) AND (clinical trial OR intervention study). All publications were retrieved to an Endnote file (Endnote ×4, Thomson Reuters, San Francisco, CA), and the duplicates were deleted.
Inclusion criteria and study selection
Studies were included if they: (1) used a randomized clinical trial (RCT) study design; (2) were HIV prevention interventions for people living with HIV/AIDS (PLWHA); (3) measured unprotected vaginal or anal intercourse; and (4) provided sufficient information to calculate effect size (ES) estimates. Studies targeting HIV-infected pregnant women were excluded because of the unique nature of antenatal care and programs to prevent mother-to-infant transmission. We did not include studies among children and young adolescents, as the interest outcome of this meta-analysis is UVAI. One trial included participants aged 16 years or older but the majority of the study sample were adults, and therefore, this study was included in our analysis [10].
All abstracts were independently reviewed by two authors (L. Yin and N. Wang), and full texts were reviewed for determining eligibility if abstracts missed key information. Papers that did not meet the above-mentioned criteria were excluded. Any disagreements were resolved by further discussion involving another author (H.-Z. Qian). The references from each eligible paper or relevant review were also examined to supplement the literature search described above, termed cross-referencing.
Data extraction
For eligible studies, two authors extracted the following data independently in a standardized manner: authors, publication year, study period, study country, number of cities involved, approach of recruiting participants, gender distribution of participants, sample size and characteristics of participants in each study arm, possible route of acquiring HIV, description of intervention in each study arm, duration of follow-up, retention rate at the last follow-up, HIV status of sexual partners, and proportion or mean frequency of UVAI in each study arm at baseline and subsequent follow-ups. Any disagreements were reviewed and discussed by at least two authors until a consensus was reached.
Rigor score
The rigor of study design for each of the included studies was assessed using an 8-item scale, as used in other reviews [3], [28], plus an additional item of sample size; this cut-off value of 100 for sample size item was chosen to enhance the rigor score of studies with higher statistical power. The scale is additive, with 1 point awarded for each of these 9 items. For example, if more than half of socio-demographical variables at the baseline had no statistically significant difference between study arms as shown in original studies (rigor-scale item (h)), ‘1’ was marked; otherwise ‘0’. Therefore, the rigor score can range from 0 to 9, with a higher value representing a higher rigor of study design. Note that due to our inclusion criteria of RCTs, rigor scores for all studies were 6 or greater.
Statistical methods
The main interest of our meta-analysis was to evaluate the risk of transmitting HIV through unprotected sexual contacts among PLWHA. We analyzed the effects of prevention interventions on combined unprotected virginal and anal intercourse (UVAI) instead separately on unprotected virginal intercourse (UVI) and unprotected anal intercourse (UAI) for two reasons: (1) PLWHA in the included studies in the meta-analysis represented various risk groups such as drug users, blood donors and men who have sex with men (MSM) who could transmit HIV to male and/or female sexual partners through unprotected vaginal intercourse (UVI) or unprotected anal intercourse (UAI), (2) Most studies only reported the status of condom use, but did not specify whether using condoms during anal or virginal intercourse. All of the intervention studies that were included in the meta-analysis had measurements of UVAI at baseline and at least one follow-up time point in each study arm (i.e., intervention or control arm), other measurements were published elsewhere [29], such as alcohol use and drug use. Some studies had multiple measurements at different follow-up time points. In the latter case, the latest follow-up measurement was used in the primary meta-analysis for estimating the overall effect size; in additional subgroup analyses considering the efficacy of interventions at different time points, each follow-up measurement was considered. For studies with more than one intervention arm [10], [20], [22], [24], [30], effect sizes were calculated using the same control condition. The primary meta-analysis ignored correlation between interventions from the same study arm; the robustness of results to this correlation was assessed in sensitivity analyses that removed correlated studies. As the measurements were either expressed as proportion differences or as mean differences of frequency of UVAI, we converted estimates to a common metric of standard mean differences (SMD) using a Cox transformation [31], [32]. SMD in each study arm was calculated as the difference of mean at follow-up and baseline divided by the pooled standard deviation (SD) of these two means [33]. We contacted available authors when published articles provided insufficient information to make the calculations; four studies were excluded because insufficient data was provided by study authors [34], [35], [36], [37]. As study arms might not be comparable at baseline, even in RCTs, Becker's strategy was used to adjust for baseline UVAI between study arms [33]. The difference of SMDs between study arms, defined as effect size (ES), was calculated for each study and then pooled across studies using standard meta-analysis with a random effects model [38]. A negative value of SMD difference indicates reduction of UAVI in the intervention arm compared to the control arm. Random effect estimates allow for variation of the true effects across studies [39], and were derived using the DerSimonian-Laird method [40], [41]. The meta-analysis results were displayed with forest plots separately by type of sexual partners (any sexual partners and HIV-negative or unknown sexual partner [HNUP]).
Heterogeneities were assessed by I2 statistics [42], and standardized deleted residual analyses were performed to identify outliers. The funnel plot, Begg and Mazumdar rank correlation test and Egger's test of the intercept were employed to assess indications of publication bias [43].
Subgroup analyses were performed to examine effect sizes by recall period on UAVI (>3 months, 3 months, or <1 month), number of study cities (>1 or 1), participant recruitment (institution-based or non-institution-based), formats of the delivering intervention (group-based or individual-based), durations of follow-up (≥15 months, 11–15 months, 6–10 months, 1–5 months or immediately after intervention), retention rates at the latest follow-up (<80% or ≥80%), sample sizes at baseline (≤300 or>300), rigor scores (<9 or 9), and risk groups (men who have sex with men [MSM] or other population). Meta-regression was also used to examine the relationship of above-mentioned between-groups effects, except for duration of follow-ups (because outcomes at multiple follow-ups were often reported in individual studies).
Sensitivity analyses were conducted to determine the stability of the intervention efficacy estimate by evaluating whether the overall effect size was sensitive to inclusion of any individual studies. Studies excluded in iterative sensitivity analyses included those producing outliers identified by standardized deleted residuals analyses, those involving two active intervention arms contrasted to the same control arm in the same study, those that noted statistically significant efficacy on UVAI, those published before the year 2006, those targeting MSM only, and those with sample sizes less than 300 participants. All meta-analyses were performed by two authors independently in the R/S plus Software version 2.15.1 [44].
Results
Results of literature search
The initial searches in 13 individual electronic databases yielded 8717 entries meeting our predefined inclusion criteria, of which 3769 were duplicate and were excluded (Figure 1). A total of 4948 titles and abstracts were reviewed, and 4854 were excluded because they were deemed irrelevant to the review topic. In the remaining 94 articles, 73 were further excluded for the following reasons: not original articles but rather editorials, comments or reviews (k = 5); lack of information on target outcome or measure of interest (k = 31); not RCTs (k = 23); HIV-negative study subjects included (k = 8); and repeated reporting of the same study (k = 6). These 73 excluded studies are listed in the supplementary material (File S1). Finally, 21 citations were included in the meta-analysis [10], [11], [12], [13], [14], [16], [17], [18], [19], [20], [21], [22], [23], [24], [30], [45], [46], [47], [48], [49], [50].
Figure 1. Flow diagram of literature search process1.
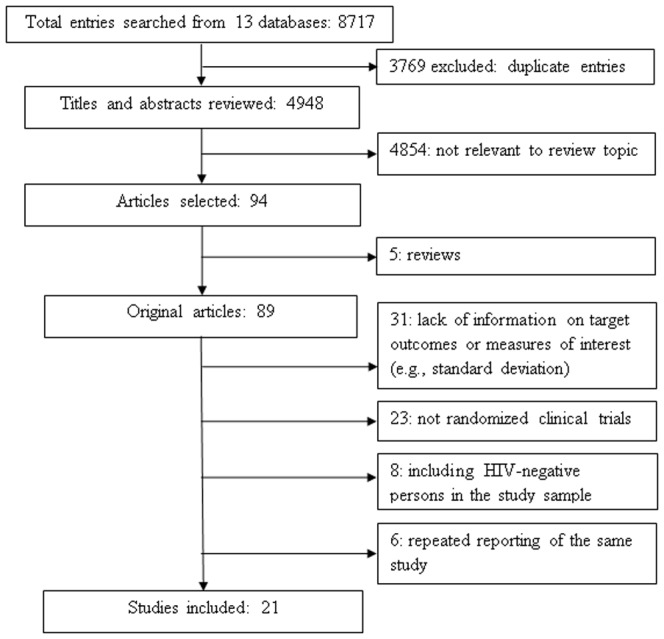
1 Thirteen databases included: 1) AMED; 2) British Library Direct; 3) British Nursing Index; 4) Centre for Reviews and Dissemination databases; 5) Cochrane Library; 6) EMBASE; 7) EconLit; 8) ERIC; 9) Ovid Medline; 10) PsycINFO; 11) Scopus; 12) Web of Science; and (13) Global Health Library Virtual Platform (World Health Organization).
Description of studies
All of the 21 included studies were conducted in the United States (Table 1). The sample sizes ranged from 51 to 3,556 at baseline and totaled 11,286 PLWHA. In most studies (k = 18), the participants were recruited by AIDS-service-organization-based sampling (ASOBS), such as from hospitals, clinics, or detoxification centers. Duration of interventions lasted from 3 to 18 months. The retention rates of participants ranged between 30% and 95%. The commonly used behavioral theories included information-motivation-behavioral skills model [10], [11], [14], [16], [17], [20], [21], [24], [30], [47], [50], social cognitive theory/social learning theory [11], [19], [45], [46], [49], [50], cognitive-behavioral coping [10], [18], [47], and theory of planned behavior [10], [50]. The rigor score of included studies ranged from 6 to 9 with a mean score of 7.95. Eight RCTs had a full score of 9 [11], [12], [17], [19], [21], [23], [49], [50] (Table 2).
Table 1. Randomized clinical trials of prevention intervention among PLWHA1 , 2.
| Publication | Country (trial period) | No. of cities | Study participants | Description of interventions | Duration of follow-up (months) | Retention (%) | |||||||
| Venue of recruiting participants | Gender(%) | Risk group | No. of participants (Mean and range of age at baseline) | IG | CG | ||||||||
| IG | CG | ||||||||||||
| Cleary et al. [45], 1995 | USA (1986–1989) | 1 | ASOBS | 78% Male | Blood donors | Pre-intervention 135 Post-intervention 94 (32, 18–55+) | Pre-intervention 136 Post-intervention 106 (32, 18–55+) | Cognitive behavioral and skills training support group | Community referral program | 12 | IG: 70 CG: 78 | ||
| Kalichman et al. [46], 2001 | USA (N/A) | 1 | ABS, ASOBS | 70% Male | 89% MSM | Pre-intervention 185 Post-intervention 150F3 or 146F6 (40, N/A) | Pre-intervention 143 Post-intervention 121F3 or 110F6 (40, N/A) | Group intervention focused on strategies for practicing safer sexual behavior | Contact-matched, health-maintenance support group | 6 | IG: 79 CG: 77 | ||
| Margolin et al. [47], 2003 | USA (1997–2001) | 1 | ASOBS | 70% Male | IDU | Pre-intervention 45 Post-intervention 32F0 or 34F3 (41, N/A) | Pre-intervention 45 Post-intervention 32F0 or 29F3 (41, N/A) | Manual-Guided HIV+ harm reduction program | Enhanced methadone maintenance program | 3 | 82 | ||
| Sorensen et al. [48], 2003 | USA (1994–1998) | 1 | ASOBS | 73% Male | DU | Pre-intervention 92 Post-intervention 77F6, 73F12, 73F18 (39, N/A) | Pre-intervention 98 Post-intervention 82F6, 77F12, 77F18 (38, N/A) | Case management delivered by paraprofessionals | A brief contact condition | 18 | 79 | ||
| Richardson et al. [30], 2004 | USA (1998–2001) | 1 state | ASOBS | 86% Male | 74% MSM | Pre-intervention 265 A or 324B Post-intervention 175 A or 214B (38, ≥18) | Pre-intervention 297 Post-intervention 196 (39, ≥18) | A: gain-frame: positive consequences of safer sex B: loss-frame: negative consequences of unsafe sex | Attention-control: medication adherence | 7 | 66 | ||
| Rotheram-Borus et al. [10], 2004 | USA (1999–2004) | 3 | ASOBS, ABS, RDS, CBS | 78% Male | 69% MSM | Pre-intervention 59C or 61D Post-intervention 48C or 50D (23, 16–29) | Pre-intervention 55 Post-intervention 45 (23, 16–29) | C: telephone delivered intervention D: in-person delivered intervention | Delayed-intervention | 15 | 82 | ||
| Wingood et al. [49], 2004 | USA (1997–2001) | 2 states | ASOBS | Female | SAA | Pre-intervention 190 Post-intervention 176F6 or 162F12 (34, 18–50) | Pre-intervention 176 Post-intervention 165F6 or 159F12 (34, 18–50) | Sexual risk reduction and social networks | Adherence and nutrition | 12 | IG: 85 CG: 90 | ||
| Wolitski et al. [50], 2005 | USA (2000–2002) | 2 | CBS | Male | MSM | Pre-intervention 413 Post-intervention 358F3 or 375F6 (41, 20–89) | Pre-intervention 398 Post-intervention 335F3 or 354F6 (41, 20–89) | Enhanced intervention (safer sex information, learning activities, peer-led discussion groups) | Standard intervention (safer sex information) | 6 | IG: 91 CG: 89 | ||
| Naar-King et al. [16], 2006 | USA (N/A) | 1 | ASOBS | 51% Male | 41% MSM | Pre-intervention 25 Post-intervention 21 (21, 16–25) | Pre-intervention 26 Post-intervention 26 (21, 16–25) | Four-session motivational enhancement intervention | Wait-list control intervention | 6 | 80 | ||
| Purcell et al. [11], 2007 | USA (2001–2005) | 4 | CBS | 60% Male | IDU | Pre-intervention 486 Post-intervention 419F3, 402F6, 417F12 (42, 22–60) | Pre-intervention 480 Post-intervention 421F3, 404F6, 404F12 (42, 22–60) | Peer mentoring intervention | Video discussion intervention | 12 | IG: 86 CG: 84 | ||
| Gilbert et al. [17], 2008 | USA (2003–2006) | 1 | ASOBS | 79% Male | 51% MSM | Pre-intervention 240 Post-intervention 182F3 or 200F6 (43, ≥18) | Pre-intervention 231 Post-intervention 188F3 or 193F6 (44, ≥18) | Tailored risk-reduction counseling from a “Video Doctor” | Usual care | 6 | IG: 83 CG: 84 | ||
| Sikkema et al. [18], 2008 | USA (2002–2005) | 1 | CBS, ASOBS | 48% Male | People with CSA histories | Pre-intervention 102 Post-intervention 88F0, 88F4, 84F8, 81F12 (41, ≥18) | Pre-intervention 104 Post-intervention 95F0, 88F4, 87F8, 82F12 (42, ≥18) | HIV and trauma coping group experimental intervention | Time-matched HIV support group comparison | 12 | IG: 79 CG: 79 | ||
| Williams et al. [19], 2008 | USA (2003–2006) | 1 | ABS, ASOBS | Male | People with CSA histories | Pre-intervention 75 Post-intervention 70 (43, ≥18) | Pre-intervention 62 Post-intervention 58 (43, ≥18) | Sexual health intervention for men guided by cognitive-behavioral approaches | Standard health promotion Intervention | 6 | 93 | ||
| McKirnan et al. [12], 2010 | USA (2004–2006) | 1 | ASOBS | Male | MSM | Pre-intervention 166 Post-intervention 133F6 or 152F12(42, 18–50+) | Pre-intervention 151 Post-intervention 122F6 or 139F12 (42, 18–50+) | Peer-led treatment advocacy program, primary-care-based, individual counseling intervention | Standard care | 12 | IG: 92 CG: 94 | ||
| Myers et al. [20], 2010 | USA (2004–2007) | 13 | ASOBS | 70% Male | 52% MSM | Pre-intervention 768 E, 975 F, 758 G Post-intervention 583 E, 604 F, 333 G (N/A, ≥18) | Pre-intervention 1055 Post-intervention 612 (N/A, ≥18) | E: MCP-delivered intervention F: PS-delivered intervention G: interventions delivered by MCP and PS | Standard care | 12 | IG: 76A 62B 44C CG: 58 | ||
| Rose et al. [21], 2010 | USA (2004–2006) | 1 | ASOBS | 69% Male | SAA | Pre-intervention 181 Post-intervention 161 (43, 25–65) | Pre-intervention 205 Post-intervention 167 (43, 25–65) | HIV risk-reduction intervention | Standard care | 6 | IG: 89 CG: 81 | ||
| Rosser et al. [22], 2010 | USA (2005–2007) | 6 | ABS, CBS, ASOBS, WBS | Male | MSM | Pre-intervention 248H or 237I Post-intervention 197F6 ,H, 194F6 ,I 196F12 ,H,185F12 ,I 188F18 ,H, 184F18 ,I (N/A, 18–45+) | Pre-intervention 190 Post-intervention 166F6,161F12,155F18 (N/A, 18–45+) | H: Man to Man sexual health seminar; I: positive tailored sexual health seminar | Prevention video (men speaking out) | 18 | IG: 76A 78B CG: 82 | ||
| Teti et al. [13], 2010 | USA (2004–2007) | 1 | ASOBS, PRS, ABS | Female | 86% Black adults | Pre-intervention 92 Post-intervention 61F6, 46F12, 28F18 (40, 20–70) | Pre-intervention 92 Post-intervention 70F6, 52F12, 27F18 (38, 20–70) | Received messages, group-level, peer-led support intervention | Received brief messages | 18 | IG: 30 CG: 29 | ||
| Wolitski et al. [23], 2010 | USA (2004–2007) | 3 | ASOBS | 70% Male | Homeless and unstably housed adults | Pre-intervention 315 Post-intervention 301F6, 284F12, 274F18 (N/A, 18–50+) | Pre-intervention 315 Post-intervention 275F6, 266F12, 259F18 (N/A, 18–50+) | Immediate housing opportunities for people with AIDS rental assistance | Customary housing service | 18 | IG: 87 CG: 82 | ||
| Lovejoy et al. [24], 2011 | USA (2009–2010) | 5 | ABS, ASOBS | 54% Male | Middle-age and older adults | Pre-intervention 38 J or 39K Post-intervention 34F3 ,J,36 F6 ,K 36F3 ,J, 36 F6 ,K (53, 45–66) | Pre-intervention 23 Post-intervention 22F3,23F6 (53, 45–66) | J: 4-session TDMII K: 1-session TDMII | No | 6 | IG: 95A 92B CG: 100 | ||
| Golin et al. [14], 2012 | USA (2006–2009) | 2 | ASOBS | 65% Male | SAA | Pre-intervention 248 Post-intervention 206F4, 183F8, 154F12 (43, ≥18) | Pre-intervention 242 Post-intervention 206F4, 187F8, 155F12 (43, ≥18) | SafeTalk: 4-session MI-based safer sex program | New Leaf: 4-session heart-healthy attention-matched control program | 12 | 63 | ||
PLWHA: people living with HIV/AIDS; IG: intervention group; CG: control groups; ABS: advertisement-based sampling; CBS: community-based sampling; ASOBS: AIDS-service-organization-based sampling; PRS: peer-referral sampling; RDS: response-driven sampling; WBS: web-based sampling; MSM: men who have sex with men; DU: drug users; IDU: injection drug users; CSA: child sexual abuse; SAA: sexually active adults; MCP: medical care provider; PS: prevention specialist; TDMII: telephone-delivered motivational interviewing interventions; N/A: not available;
Some studies explored 2–3 intervention groups, including A: gain-frame positive consequences of safer sex; B: loss-frame, negative consequences of unsafe sex; C: telephone delivered intervention; D: in-person delivered intervention; E: medical care provider-delivered intervention; F: prevention specialist-delivered intervention; G: interventions delivered by primary care providers and prevention specialists; H: Man to Man sexual health seminar; I: positive tailored sexual health seminar; J: 4-session telephone-delivered motivational interviewing intervention; K: 1-session telephone-delivered motivational interviewing intervention;
Immediately after intervention;
In the 3-month follow-up;
In the 4-month follow-up;
In the 6-month follow-up;
In the 8-month follow-up;
In the 12-month follow-up;
In the 18-month follow-up.
Table 2. Rigor score of study design1.
| Publication | Cohort(a) | With control group (b) | Pre/post intervention(c) | Random assignment(d) | Random selection for assessment (e) | Sample size >100 (f) | Follow-up rate ≥80%(g) | Comparable socio-demographics between study arms (h) | Comparable baseline outcome measures between study arms (i) | Total |
| Cleary et al. [45], 1995 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 7 |
| Kalichman et al. [46], 2001 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 8 |
| Margolin et al. [47], 2003 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 7 |
| Sorensen et al. [48], 2003 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 7 |
| Richardson et al. [30], 2004 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 6 |
| Rotheram-Borus et al. [10], 2004 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 8 |
| Wingood et al. [49], 2004 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Wolitski et al. [50], 2005 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Naar-King et al. [16], 2006 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 8 |
| Purcell et al. [11], 2007 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Gilbert et al. [17], 2008 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Sikkema et al. [18], 2008 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 8 |
| Williams et al. [19], 2008 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| McKirnan et al. [12], 2010 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Myers et al. [20], 2010 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 6 |
| Rose et al. [21], 2010 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Rosser et al. [22], 2010 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 8 |
| Teti et al. [13], 2010 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 7 |
| Wolitski et al. [23], 2010 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Lovejoy et al. [24], 2011 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 7 |
| Golin et al. [14], 2012 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 8 |
1-point score was given for meeting each of the following criteria: (a) being a prospective cohort study; (b) using a comparison group; (c) collecting pre-/post-intervention data; (d) employing random assignment of participants to study arms; (e) having all study participants or a random selection of them for assessments; (f) having a sample size >100; (g) having a follow-up rate ≥80%; (h) having comparable socio-demographics between study arms, including age, education, race, employment, income, marital status (“Comparability” was defined as more than half of socio-demographical variables had no statistically significant difference between study arms as shown in the original publication, and ‘1’ was marked; otherwise ‘0’); and (i) had comparable outcome measures at baseline between study arms.
Impact of prevention intervention on UVAI with any sexual partners
Eight studies provided mean frequencies of UVAI [14], [16], [18], [19], [24], [46], [48], [49], and 13 provided proportions of UVAI [10], [11], [12], [13], [17], [20], [21], [22], [23], [30], [45], [47], [50]. Reduction of UVAI was observed in the intervention arm in most studies, except that two studies observed an increased risk of UVAI in the gain-framed approach or telephone-delivered intervention measures [10], [30]. Of these 21 trials, 15 reported UVAI with any sexual partners, and 10 reported UVAI with HNUP.
Figure 2 shows the efficacy of prevention interventions on UVAI with any sexual partners from 18 interventions in 15 RCTs. Of them, 14 intervention measures showed that prevention interventions reduced UVAI after adjusting for the baseline difference between study arms, but only two were statistically significant [46], [49]. Four intervention measures observed an increased risk in intervention arms versus control arms [19], [24], [30], [45]. After pooling, the meta-analysis demonstrated a lower average UVAI with any sexual partners in the intervention arms compared with the control arms (mean ES: −0.20; 95% CI: −0.30, −0.10; P<0.01; k = 15). There was null heterogeneity among these 15 studies (I2 = 0%; P = 0.75). The funnel plot showed no evidence of publication bias (Kendall tau = −0.05; P = 0.82; Egger's t value = −0.41; P = 0.68).
Figure 2. Forest plot of effect size: impact of prevention interventions on UVAI with any sexual partners among PLWHA1.

1 UVAI: unprotected vaginal and/or anal intercourse; PLWHA: people living with HIV/AIDS; TDMII: telephone-delivered motivational interviewing interventions.
Table 3 summarizes the subgroup analyses of the efficacy of intervention on UVAI with any sexual partners. On average, the interventions reduced UVAI with any sexual partner within 10 months post intervention (or “short-term” effect) (mean ES [95% CI]: 1–5 months: −0.23 [−0.37, −0.08], k = 8; 6–10 months: −0.18 [−0.29, −0.08], k = 14), while the long-term impact of the interventions was not statistically significant (mean ES [95% CI]: 11–15 months: −0.12 [−0.30, 0.06], k = 9; >15 months: −0.05 [−0.43, 0.32], k = 2). A reduction of UVAI was observed among studies in which UVAI was recalled in the past 3 months (mean ES [95% CI]: −0.21 [−0.34, −0.08], k = 10), but not among studies where UVAI was recalled for ≤1 month or >3 months (both k = 4). Group-based interventions appeared more effective (mean ES [95% CI]: −0.27 [−0.42, −0.12], k = 12) than individual-based interventions (−0.13 [−0.27, 0.01], k = 6). RCTs with a sample size of >300 showed a reduction of UVAI (mean ES [95% CI]: −0.26 [−0.34, −0.09], k = 7), but those with a sample size of ≤300 did not reach statistical significance (mean ES [95% CI]: −0.16 [−0.34, 0.02], k = 11). Prevention intervention effects were not substantially affected by number of study cities, approach of recruiting participants, retention rate at the last follow-up, and rigor score of study design. With the above noted, it is important to point out that in meta-regression, none of these factors statistically modified the overall effect size of UVAI with any sexual partners (P>0.05).
Table 3. Subgroup and sensitivity analyses for UVAI with any sexual partners among PLWHA1.
| Subgroup | No. of intervention | Combined effect size (95% CI) | P value | Heterogeneity | |
| I2 (%) | P value | ||||
| Recall period on UVAI (months) | |||||
| ≤1 | 4 | −0.16 (−0.44, 0.13) | 0.28 | 33.4 | 0.21 |
| 3 | 10 | −0.21 (−0.34, −0.08) | <0.01 | 0 | 0.68 |
| >3 | 4 | −0.19 (−0.43, 0.04) | 0.11 | 0 | 0.65 |
| Number of study cities | |||||
| 1 | 10 | −0.21 (−0.35, −0.06) | 0.01 | 0 | 0.62 |
| >1 | 8 | −0.19 (−0.33, −0.05) | 0.01 | 0 | 0.59 |
| Venue of recruiting participants | |||||
| AIDS service organizations (ASO) | 10 | −0.17 (−0.29, −0.05) | 0.01 | 0 | 0.55 |
| Non-ASO | 8 | −0.28 (−0.47, −0.09) | <0.01 | 0 | 0.79 |
| Format of delivering intervention | |||||
| Group-based | 12 | −0.27 (−0.42, −0.12) | <0.01 | 0 | 0.71 |
| Individual-based | 6 | −0.13 (−0.27, 0.01) | 0.06 | 0 | 0.69 |
| Duration of follow-up (months) | |||||
| Immediately after intervention | 3 | −0.27 (−0.56, 0.03) | 0.07 | 0 | 0.82 |
| 1–5 | 8 | −0.23 (−0.37, −0.08) | <0.01 | 0 | 0.92 |
| 6–10 | 14 | −0.18 (−0.29, −0.08) | <0.01 | 0 | 0.81 |
| 11–15 | 9 | −0.12 (−0.30, 0.06) | 0.18 | 32.7 | 0.16 |
| >15 | 2 | −0.05 (−0.43, 0.32) | 0.78 | 0 | 0.69 |
| Retention rate at the last follow-up | |||||
| <80% | 8 | −0.16 (−0.30, −0.02) | 0.03 | 7.5 | 0.37 |
| ≥80% | 10 | −0.26 (−0.41, −0.10) | <0.01 | 0 | 0.89 |
| Sample size at baseline | |||||
| ≤300 | 11 | −0.16 (−0.34, 0.02) | 0.08 | 0 | 0.71 |
| >300 | 7 | −0.26 (−0.34, −0.09) | <0.01 | 0 | 0.50 |
| Publication year | |||||
| Prior to 2006 | 9 | −0.22 (−0.37, −0.08) | <0.01 | 9.6 | 0.36 |
| In 2006 or later | 9 | −0.17 (−0.31, −0.02) | 0.03 | 0 | 0.89 |
| Rigor score | |||||
| <9 | 14 | −0.19 (−0.31, −0.06) | <0.01 | 0 | 0.63 |
| 9 | 4 | −0.23 (−0.41, −0.05) | 0.01 | 0 | 0.60 |
| Sensitivity analyses | |||||
| Excluded Cleary et al. [45], 1995 | 17 | −0.22 (−0.32, −0.11) | <0.01 | 0 | 0.83 |
| Excluded Kalichman et al. [46], 2001 | 17 | −0.18 (−0.28, −0.07) | <0.01 | 0 | 0.79 |
| Excluded Richardson et al. [30], 2004 (gain-frame) | 17 | −0.22 (−0.33, −0.11) | <0.01 | 0 | 0.80 |
| Excluded Richardson et al. [30], 2004 (loss-frame) | 17 | −0.19 (−0.29, −0.08) | <0.01 | 0 | 0.73 |
| Excluded Rotheram-Borus et al. [10], 2004 (telephone) | 17 | −0.20 (−0.30, −0.10) | <0.01 | 0 | 0.69 |
| Excluded Rotheram-Borus et al. [10], 2004 (in-person) | 17 | −0.19 (−0.29, −0.09) | <0.01 | 0 | 0.76 |
| Excluded Wingood et al. [49], 2004 | 17 | −0.18 (−0.29, −0.07) | <0.01 | 0 | 0.76 |
| Excluded Naar-King et al. [16], 2006 | 17 | −0.19 (−0.30, −0.09) | <0.01 | 0 | 0.72 |
| Excluded McKirnan et al. [12], 2010 | 17 | −0.20 (−0.30, −0.09) | <0.01 | 0 | 0.69 |
| Excluded Lovejoy et al. [24], 2011 (4-session TDMII) | 17 | −0.20 (−0.31, −0.10) | <0.01 | 0 | 0.72 |
| Excluded Lovejoy et al. [24], 2011 (1-session TDMII) | 17 | −0.20 (−0.30, −0.10) | <0.01 | 0 | 0.69 |
UVAI: unprotected vaginal or anal intercourse; PLWHA: people living with HIV/AIDS; TDMII: telephone-delivered motivational interviewing interventions.
In standardized deleted residual analysis, no individual study was identified as an outlier, but Teti et al. 's study [13] was found as an outlier in the subgroup of 11–15 months follow-up (standardized deleted residual = 2.04). Further sensitivity analyses were used to evaluate the stability of summary effect sizes in meta-analyses for these considerations: use of multiple interventions in a single trial [10], [24], [30], statistically significant efficacy on UVAI [46], [49], publication prior to year 2000 [45], targeting of MSM only [12], and sample size less than 100 [16]. After excluding any one of the above-mentioned studies or interventions, the statistically significant association between interventions and UVAI was still observed (Table 3). Additional sensitivity analysis was performed to determine the stability of the intervention efficacy in the subgroup of 11–15 months follow-up, and found a significant reduction of UVAI during 11–15 months follow-up after intervention (mean ES [95% CI]: −0.17 [−0.32, −0.02; P = 0.03]; I2 = 7.4%, P = 0.37; k = 8).
Impact of prevention intervention on UVAI with HNUP
Ten RCTs including 14 interventions evaluated the impact of interventions on UVAI with HNUP. Among these RCTs, ten intervention measures had a reduction of UVAI and four increased UVAI, but none reached statistical significance. However, a meta-analysis showed that prevention interventions were associated with a significant average reduction of UVAI with HNUP (mean ES: −0.13; 95% CI: −0.22, −0.04; P = 0.01). Neither heterogeneity (I2 = 0%; P = 0.77) nor publication bias were observed (Kendall tau = 0.14; P = 0.52; Egger's t value = −0.004; P = 0.997) (Figure 3).
Figure 3. Forest plot of effect size: impact of prevention interventions on UVAI with HIV negative or unknown status sexual partner among PLWHA1.

1 UVAI: unprotected vaginal and/or anal intercourse; PLWHA: people living with HIV/AIDS; MCP: medical care provider; PS: prevention specialist; Man2Man: man to man sexual health seminar; PoSH: positive sexual health seminar.
Similar subgroup analyses were also conducted for UVAI with HNUP as were for UVAI with any sexual partners. The efficacy of interventions was statistically significant only among some subgroups of interventions: those with the recall period on UVAI >3 months (P = 0.02), those with the number of study cities >1 (P = 0.02), those with participant recruitment through AIDS service organization based venues (P = 0.02), those with group-based format of delivering interventions (P = 0.02), those with retention rate at the latest follow-up <80% (P = 0.02), those with a duration of follow-up between 11–15 months (P = 0.01), those with mixed risk group participants (P = 0.02), those with a sample size at baseline >300 (P = 0.01), and those with a rigor score <9 (P = 0.01). However, no statistical variation of UVAI with HNUP was found among subgroups in meta-regression (P>0.05). No single study was identified as an outlier in standardized deleted residual analysis in overall meta-analysis and each subgroup of follow-up period. Further sensitivity analyses that were performed by removing the studies using multiple intervention approaches [10], [20], [22] found that the aggregate magnitude of impact of the interventions was weakened after removing the study by Myers et al. [20] (mean ES, −0.10; 95% CI, −0.21, 0.01; P = 0.09) (Table 4).
Table 4. Subgroup and sensitivity analyses for UVAI with HIV negative or unknown status sexual partners among PLWHA1.
| Subgroup | No. of intervention | Combined effect size (95% CI) | P value | Heterogeneity | |
| I2 (%) | P value | ||||
| Recall period on UVAI (months) | |||||
| 3 | 8 | −0.11 (−0.24, 0.02) | 0.11 | 0 | 0.65 |
| >3 | 6 | −0.15 (−0.28, −0.02) | 0.02 | 0 | 0.58 |
| Number of study cities | |||||
| 1 | 4 | −0.15 (−0.39, 0.09) | 0.23 | 32 | 0.22 |
| >1 | 10 | −0.12 (−0.23, −0.02) | 0.02 | 0 | 0.87 |
| Venue of recruiting participants | |||||
| AIDS service organizations (ASO) | 6 | −0.16 (−0.29, −0.03) | 0.02 | 0 | 0.68 |
| Non-ASO | 8 | −0.10 (−0.23, 0.03) | 0.15 | 0 | 0.60 |
| Format of delivering intervention | |||||
| Group-based | 12 | −0.12 (−0.22, −0.02) | 0.02 | 0 | 0.78 |
| Individual-based | 2 | −0.23 (−0.58, 0.12) | 0.20 | 27.6 | 0.24 |
| Duration of follow-up (months) | |||||
| Immediately after intervention | 3 | −0.03 (−0.23, 0.17) | 0.78 | 0 | 0.95 |
| 1–5 | 4 | −0.13 (−0.29, 0.02) | 0.09 | 0 | 0.46 |
| 6–10 | 12 | −0.10 (−0.20, 0.01) | 0.08 | 17.8 | 0.27 |
| 11–15 | 11 | −0.13 (−0.24, −0.03) | 0.01 | 0 | 0.64 |
| >15 | 3 | −0.03 (−0.25, 0.19) | 0.80 | 0 | 0.89 |
| Retention rate at the last follow-up | |||||
| <80% | 7 | −0.14 (−0.26, −0.02) | 0.02 | 0 | 0.81 |
| ≥80% | 7 | −0.11 (−0.25, 0.04) | 0.15 | 0.2 | 0.42 |
| Risk group | |||||
| All MSM | 4 | −0.11 (−0.28, 0.06) | 0.20 | 0 | 0.46 |
| Other risk groups or mixed groups | 10 | −0.13 (−0.24, −0.03) | 0.02 | 0 | 0.70 |
| Sample size at baseline | |||||
| ≤300 | 3 | −0.12 (−0.57, 0.33) | 0.61 | 41.8 | 0.18 |
| >300 | 11 | −0.13 (−0.23, −0.04) | 0.01 | 0 | 0.85 |
| Rigor score | |||||
| <9 | 9 | −0.15 (−0.26, −0.03) | 0.01 | 0 | 0.68 |
| 9 | 5 | −0.10 (−0.25, 0.06) | 0.23 | 0 | 0.55 |
| Sensitivity analyses | |||||
| Excluded Rotheram-Borus et al. [10], 2004 (telephone) | 13 | −0.13 (−0.23, −0.04) | 0.01 | 0 | 0.75 |
| Excluded Rotheram-Borus et al. [10], 2004 (in-person) | 13 | −0.12 (−0.21, −0.03) | 0.01 | 0 | 0.87 |
| Excluded Myers et al. [20], 2010 (MCP & PS) and (PS) | 13 | −0.11 (−0.22, −0.01) | 0.04 | 0 | 0.65 |
| Excluded Myers et al. [20], 2010 (MCP & PS) and (MCP) | 13 | −0.11 (−0.22, −0.01) | 0.04 | 0 | 0.65 |
| Excluded Myers et al. [20], 2010 (PS) and (MCP) | 13 | −0.11 (−0.22, −0.01) | 0.03 | 0 | 0.64 |
| Excluded Rosser et al. [22], 2010 (Man2Man) | 13 | −0.14 (−0.23, −0.05) | <0.01 | 0 | 0.77 |
| Excluded Rosser et al. [22], 2010 (PoSH) | 13 | −0.13 (−0.23, −0.04) | 0.01 | 0 | 0.71 |
UVAI: unprotected vaginal and/or anal intercourse; PLWHA: people living with HIV/AIDS; MSM: men who have sex with men; MCP: medical care provider; PS: prevention specialist; Man2Man: man to man sexual health seminar; PoSH: positive sexual health seminar.
Discussion
Our systematic meta-analytic review involving 11,286 PLWHA from 15 RCTs studying 18 interventions suggests that prevention interventions are efficacious to reduce UVAI with any sexual partners. This conclusion is robust, as demonstrated in sensitivity analyses by removing some selected studies, which did not alter the findings. Similar meta-analysis was performed separately for UVAI with HIV negative or unknown status sexual partners from 10 RCTs involving 14 interventions, and confirmed the significant efficacy of prevention interventions.
One previous systematic review and meta-analysis of 10 RCTs and two quasi-experimental studies showed that prevention interventions resulted in a 43% overall reduction in unprotected sex, and a 39% reduction in the subgroup analysis of 10 RCTs [15]. Compared with this review, our meta-analysis included eight of these 10 RCTs; two quasi-experimental studies were excluded [51], [52], and two RCTs were also excluded because they did not report total sexual activity (only reporting insertive anal intercourse) [53] or did not provide sufficient information for calculating ES [34]. Our review included 13 additional more recent RCTs [11], [12], [13], [14], [16], [17], [18], [19], [20], [21], [22], [23], [24]; we found that prevention intervention reduced UVAI by 20%. The magnitude of difference in our study was less than that reported in the earlier meta-analysis [15], but it is useful to appreciate the potential impact of these particular approaches in guiding public health investments and designing future research studies.
Our subgroup analyses of trials that assessed outcomes within 15 months post intervention showed a statistically significant relationship between interventions and reduction of UVAI with any sexual partners; while the follow-up assessments from 11 to 15 months showed a non-significant protective trend, but significant protective trend was found after excluding one outlier study [13]. The evidence available for more than 15 months of follow-up intervals was too sparse to draw a conclusion [13], [48]. These results may suggest that the impact of interventions tapers over time, although it is possible that these results merely reflect the dearth of long-term follow-up data. Future studies should evaluate the long-term impact by comparing with and without booster intervention sessions during the follow-up period, though the costs for long-term interventions sometimes are overwhelming for resources-limit settings, and long-term interventions may even not feasible in developed countries, due to manpower or financial or health insurance problems. Governments and researcher might consider developing cost-effective and easy-to-operate intervention sessions to maintain safe sex in long-term time.
Our analyses that stratified by the format of delivering interventions found a 27% reduction of UVAI for group-based interventions, but 14% non-significant reduction for individual-based interventions. This difference by format of delivering interventions was not statistically significant, but the direction of estimates was opposite to one from the previous meta-analysis of studies published between 1988–2004 by Crepaz et al [15], which found that individual-based interventions were more efficacious than group-based (51% vs. 34%). Group-based interventions could be more cost-effective than individual-based; in addition, participants in group-based interventions might be more likely to have opportunities to obtain social support from peers, as shown in studies for treating adult obesity and promoting children's physical activity [54], [55].
The previous review could not assess the impact on UVAI by HIV status of sexual partner [15]. After this review, several RCTs collected this information [11], [12], [18], [20], [21], [22], [23], so that our analysis was able to explore the impact according HIV status of sexual partner for the first time. We found a 13% reduction of UVAI with HNUP in the intervention arms versus the control arms. Most studies were conducted among PLWHA regardless of risk groups, though MSM were accounted for moderate proportion of HIV-positive participants. Only three articles reported UVAI among pure HIV-positive MSM group [12], [22], [50], whereas the effects of interventions targeting pure MSM was not statistically significant. The goal of prevention intervention programs among HIV-infected individuals is to reduce UVAI with those who have not been infected. While this meta-analysis provides valuable preliminary data on the effect on UVAI with HNUP, more studies are needed for assessing effects on UAI and UVI separately, and for investigating the effect within long-term follow-up.
Given the remarkable findings of HPTN 052 that antiretroviral therapy was associated with a significant reduction in HIV transmission [56], [57], perhaps the field should focus on treatment as prevention and the importance of medication adherence. However, sexual risk reduction should also be a component of combined intervention packages in future intervention programs. By combining results across trials we saw a significant average benefit of prevention interventions on unprotected sex, whereas most of the individual trials failed to show a statistically significant benefit. This suggests that many of these studies were underpowered. Surprisingly, although these were trials of different prevention interventions in different patient populations, there was no evidence to suggest cross-study heterogeneity in outcomes. Although this is not evidence that all prevention interventions are universally good, it does support the idea that several modestly efficacious prevention intervention options are available and that we lack strong evidence that one is better than another. The reasons for differential success may be due less to the content of the interventions and more to design issues (e.g., content of the control group).
Several issues related to the original studies require commentary. The primary outcome UVAI was self-reported; and therefore, it may be subject to social desirability bias. In addition, even though thirteen international databases were explored, all included RCTs were conducted in USA; three RCTs in Africa were excluded because no target outcomes were reported [58], [59] or not enough data were available for calculation [36]. We may not be able to extrapolate the findings from US-based trials to other cultural settings. Therefore, future clinical trials of risk reduction techniques outside of the United States are needed. Our meta-analysis has its own limitations. First, our meta-analysis only included published RCTs. We did not make requests to the scientific community (e.g., listserv) and/or to individual authors with relevant research, so unpublished or in print RCTs were not included. In addition, four trials were excluded because we did not get needed data for analysis from the investigators [34], [35], [36], [37]. Second, non-English databases were not included in our systematic searching; therefore, data from papers published in other languages might have been missed. Excluding non-English publications may generally have little effect on meta-analysis outcomes, but it is difficult to predict the importance of non-English language trials for individual systematic reviews [60]. Third, some trials had multiple interventions compared against a single control condition, and the outcomes from these trials were treated as separate findings in the meta-analysis, perhaps giving undue weights to these multi-intervention trials. However, sensitivity analyses revealed stable overall trends even when these trials were excluded. Finally, we only included RCTs; three quasi-experimental studies were excluded [51], [52], [61], because this design might overestimate intervention efficacy based on previous meta-analytic review [15].
Strengths of our approach are also worthy of mention. We adjusted for baseline differences among intervention groups, we combined continuous and categorical outcomes, and we assessed the impact on UVAI by HIV serostatus of sexual partners. The evaluation for HNUP provides additional information for developing public health programs. In summary, our meta-analysis suggests that prevention interventions are efficacious, particularly in the short-term, at reducing UVAI. Positive prevention approaches should be included in HIV prevention programs even as the research community seeks to improve their efficacy. Booster intervention sessions may be needed to achieve long-term impact on reducing unprotected sex among PLWHA in future risk reduction programs.
Supporting Information
69 excluded studies and exclusion reasons.
(DOCX)
PRISMA Checklist.
(DOC)
Data Availability
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper.
Funding Statement
This work was primarily sponsored by U.S. National Institutes of Health grants R01AI094562 and R34AI091446. This work was also supported by grants from the Ministry of Science and Technology of China (2012ZX10001-002) and Chinese State Key Laboratory for Infectious Disease Develop Grant (2012SKLID103). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Marks G, Burris S, Peterman TA (1999) Reducing sexual transmission of HIV from those who know they are infected: the need for personal and collective responsibility. AIDS 13: 297–306. [DOI] [PubMed] [Google Scholar]
- 2. Bunnell R, Mermin J, De Cock KM (2006) HIV prevention for a threatened continent: implementing positive prevention in Africa. JAMA 296: 855–858. [DOI] [PubMed] [Google Scholar]
- 3. Kennedy CE, Medley AM, Sweat MD, O'Reilly KR (2010) Behavioural interventions for HIV positive prevention in developing countries: a systematic review and meta-analysis. Bull World Health Organ 88: 615–623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Global HIV Prevention Working Group (2004) HIV prevention in the era of expanded treatment access. Available: http://www.kff.org/hivaids.
- 5. Wechsberg WM, Golin C, El-Bassel N, Hopkins J, Zule W (2012) Current interventions to reduce sexual risk behaviors and crack cocaine use among HIV-infected individuals. Curr HIV/AIDS Rep 9: 385–393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Handford CD, Tynan AM, Rackal JM, Glazier RH (2006) Setting and organization of care for persons living with HIV/AIDS. Cochrane Database Syst Rev: CD004348. [DOI] [PMC free article] [PubMed]
- 7. Ko NY, Liu HY, Lai YY, Pai YH, Ko WC (2013) Case management interventions for HIV-infected individuals. Curr HIV/AIDS Rep 10: 390–397. [DOI] [PubMed] [Google Scholar]
- 8. Centers for Disease Control and Prevention (CDC) (2003) Advancing HIV prevention: new strategies for a changing epidemic–United States, 2003. MMWR 52: 329–332. [PubMed] [Google Scholar]
- 9.Mah TL, Halperin DT (2010) Concurrent sexual partnerships and the HIV epidemics in Africa: evidence to move forward. AIDS Behav 14: 11–16; 34–17. [DOI] [PubMed]
- 10.Rotheram-Borus MJ, Swendeman D, Comulada WS, Weiss RE, Lee M, et al. (2004) Prevention for substance-using HIV-positive young people: telephone and in-person delivery. J Acquir Immune Defic Syndr 37 S68–77. [DOI] [PMC free article] [PubMed]
- 11. Purcell DW, Latka MH, Metsch LR, Latkin CA, Gomez CA, et al. (2007) Results from a randomized controlled trial of a peer-mentoring intervention to reduce HIV transmission and increase access to care and adherence to HIV medications among HIV-seropositive injection drug users. J Acquir Immune Defic Syndr 46 Suppl 2 S35–47. [DOI] [PubMed] [Google Scholar]
- 12. McKirnan DJ, Tolou-Shams M, Courtenay-Quirk C (2010) The Treatment Advocacy Program: a randomized controlled trial of a peer-led safer sex intervention for HIV-infected men who have sex with men. J Consult Clin Psychol 78: 952–963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Teti M, Bowleg L, Cole R, Lloyd L, Rubinstein S, et al. (2010) A mixed methods evaluation of the effect of the protect and respect intervention on the condom use and disclosure practices of women living with HIV/AIDS. AIDS Behav 14: 567–579. [DOI] [PubMed] [Google Scholar]
- 14. Golin CE, Earp JA, Grodensky CA, Patel SN, Suchindran C, et al. (2012) Longitudinal Effects of SafeTalk, a Motivational Interviewing-Based Program to Improve Safer Sex Practices Among People Living with HIV/AIDS. AIDS Behav 16: 1182–1191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Crepaz N, Lyles CM, Wolitski RJ, Passin WF, Rama SM, et al. (2006) Do prevention interventions reduce HIV risk behaviours among people living with HIV? A meta-analytic review of controlled trials. AIDS 20: 143–157. [DOI] [PubMed] [Google Scholar]
- 16. Naar-King S, Wright K, Parsons JT, Frey M, Templin T, et al. (2006) Healthy choices: motivational enhancement therapy for health risk behaviors in HIV-positive youth. AIDS Educ Prev 18: 1–11. [DOI] [PubMed] [Google Scholar]
- 17. Gilbert P, Ciccarone D, Gansky SA, Bangsberg DR, Clanon K, et al. (2008) Interactive “Video Doctor” counseling reduces drug and sexual risk behaviors among HIV-positive patients in diverse outpatient settings. PLoS ONE 3: e1988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Sikkema KJ, Wilson PA, Hansen NB, Kochman A, Neufeld S, et al. (2008) Effects of a coping intervention on transmission risk behavior among people living with HIV/AIDS and a history of childhood sexual abuse. J Acquir Immune Defic Syndr 47: 506–513. [DOI] [PubMed] [Google Scholar]
- 19. Williams JK, Wyatt GE, Rivkin I, Ramamurthi HC, Li X, et al. (2008) Risk reduction for HIV-positive African American and Latino men with histories of childhood sexual abuse. Arch Sex Behav 37: 763–772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Myers JJ, Shade SB, Rose CD, Koester K, Maiorana A, et al. (2010) Interventions delivered in clinical settings are effective in reducing risk of HIV transmission among people living with HIV: results from the Health Resources and Services Administration (HRSA)'s Special Projects of National Significance initiative. AIDS Behav 14: 483–492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Rose CD, Courtenay-Quirk C, Knight K, Shade SB, Vittinghoff E, et al. (2010) HIV intervention for providers study: a randomized controlled trial of a clinician-delivered HIV risk-reduction intervention for HIV-positive people. J Acquir Immune Defic Syndr 55: 572–581. [DOI] [PubMed] [Google Scholar]
- 22. Rosser BR, Hatfield LA, Miner MH, Ghiselli ME, Lee BR, et al. (2010) Effects of a behavioral intervention to reduce serodiscordant unsafe sex among HIV positive men who have sex with men: the Positive Connections randomized controlled trial study. J Behav Med 33: 147–158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Wolitski RJ, Kidder DP, Pals SL, Royal S, Aidala A, et al. (2010) Randomized trial of the effects of housing assistance on the health and risk behaviors of homeless and unstably housed people living with HIV. AIDS Behav 14: 493–503. [DOI] [PubMed] [Google Scholar]
- 24. Lovejoy TI, Heckman TG, Suhr JA, Anderson T, Heckman BD, et al. (2011) Telephone-administered motivational interviewing reduces risky sexual behavior in HIV-positive late middle-age and older adults: a pilot randomized controlled trial. AIDS Behav 15: 1623–1634. [DOI] [PubMed] [Google Scholar]
- 25. Johnson BT, Carey MP, Chaudoir SR, Reid AE (2006) Sexual risk reduction for persons living with HIV: research synthesis of randomized controlled trials, 1993 to 2004. J Acquir Immune Defic Syndr 41: 642–650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, et al. (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med 6: e1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6: e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Medley A, Kennedy C, O'Reilly K, Sweat M (2009) Effectiveness of peer education interventions for HIV prevention in developing countries: a systematic review and meta-analysis. AIDS Educ Prev 21: 181–206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wang N, Sun X, Yin L, Liu H, Ruan Y, et al. (2013) Meta-analysis of interventions for reducing number of sexual partners and drug and alcohol abuse among people living with HIV/AIDS. J AIDS Clin Res 4: pii: 14272. [DOI] [PMC free article] [PubMed]
- 30. Richardson JL, Milam J, McCutchan A, Stoyanoff S, Bolan R, et al. (2004) Effect of brief safer-sex counseling by medical providers to HIV-1 seropositive patients: a multi-clinic assessment. AIDS 18: 1179–1186. [DOI] [PubMed] [Google Scholar]
- 31.Cox DR (1970) Analysis of binary data. New York: Chapman & Hall/CRC.
- 32. Sanchez-Meca J, Marin-Martinez F, Chacon-Moscoso S (2003) Effect-size indices for dichotomized outcomes in meta-analysis. Psychol Methods 8: 448–467. [DOI] [PubMed] [Google Scholar]
- 33. Becker BJ (1988) Synthesizing standardized mean-change measures. Br J Math Stat Psychol 41: 257–278. [Google Scholar]
- 34. Patterson TL, Shaw WS, Semple SJ (2003) Reducing the sexual risk behaviors of HIV+ individuals: outcome of a randomized controlled trial. Ann Behav Med 25: 137–145. [DOI] [PubMed] [Google Scholar]
- 35. Morin SF (2007) The Healthy Living Project Team (2007) Effects of a behavioral intervention to reduce risk of transmission among people living with HIV: the healthy living project randomized controlled study. J Acquir Immune Defic Syndr 44: 213–221. [DOI] [PubMed] [Google Scholar]
- 36. Cornman DH, Kiene SM, Christie S, Fisher WA, Shuper PA, et al. (2008) Clinic-based intervention reduces unprotected sexual behavior among HIV-infected patients in KwaZulu-Natal, South Africa: results of a pilot study. J Acquir Immune Defic Syndr 48: 553–560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Kalichman SC, Cherry C, Kalichman MO, Amaral CM, White D, et al. (2011) Integrated behavioral intervention to improve HIV/AIDS treatment adherence and reduce HIV transmission. Am J Public Health 101: 531–538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Higgins J, Green S, (editors) (2011) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. Available: www.cochrane-handbook.org.
- 39. Normand SL (1999) Meta-analysis: formulating, evaluating, combining, and reporting. Stat Med 18: 321–359. [DOI] [PubMed] [Google Scholar]
- 40. DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7: 177–188. [DOI] [PubMed] [Google Scholar]
- 41.Lipsey M, Wilson D (2001) Practical meta-analysis: Thousand Oaks, CA: Sage.
- 42.Deeks J, Altman D, Bradburn M (2002) Statistical methods for examining heterogeneity and combining results from several studies in a meta-analysis. In: Egger M, Davey Smith G, Altman D, editors. Systematic reviews in health care: meta-analysis in context. London: BMJ Publications. 285–312 p.
- 43.Rothstein HR, Sutton AJ, Borenstein M (2005) Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments: Chichester, England: Wiley.
- 44.R/S plus Software can be downloaded free. Available: http://127.0.0.1:13917/doc/html/index.html.
- 45. Cleary PD, Van Devanter N, Steilen M, Stuart A, Shipton-Levy R, et al. (1995) A randomized trial of an education and support program for HIV-infected individuals. AIDS 9: 1271–1278. [DOI] [PubMed] [Google Scholar]
- 46. Kalichman SC, Rompa D, Cage M, DiFonzo K, Simpson D, et al. (2001) Effectiveness of an intervention to reduce HIV transmission risks in HIV-positive people. Am J Prev Med 21: 84–92. [DOI] [PubMed] [Google Scholar]
- 47. Margolin A, Avants SK, Warburton LA, Hawkins KA, Shi J (2003) A randomized clinical trial of a manual-guided risk reduction intervention for HIV-positive injection drug users. Health Psychol 22: 223–228. [PubMed] [Google Scholar]
- 48. Sorensen JL, Dilley J, London J, Okin RL, Delucchi KL, et al. (2003) Case management for substance abusers with HIV/AIDS: a randomized clinical trial. Am J Drug Alcohol Abuse 29: 133–150. [DOI] [PubMed] [Google Scholar]
- 49. Wingood GM, DiClemente RJ, Mikhail I, Lang DL, McCree DH, et al. (2004) A randomized controlled trial to reduce HIV transmission risk behaviors and sexually transmitted diseases among women living with HIV: The WiLLOW Program. J Acquir Immune Defic Syndr 37 Suppl 2 S58–67. [DOI] [PubMed] [Google Scholar]
- 50.Wolitski RJ, Gomez CA, Parsons JT (2005) Effects of a peer-led behavioral intervention to reduce HIV transmission and promote serostatus disclosure among HIV-seropositive gay and bisexual men. AIDS 19 S99–109. [DOI] [PubMed]
- 51. Grinstead O, Zack B, Faigeles B (2001) Reducing postrelease risk behavior among HIV seropositive prison inmates: the health promotion program. AIDS Educ Prev 13: 109–119. [DOI] [PubMed] [Google Scholar]
- 52. Rotheram-Borus MJ, Lee MB, Murphy DA, Futterman D, Duan N, et al. (2001) Efficacy of a preventive intervention for youths living with HIV. Am J Public Health 91: 400–405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Kelly JA, Murphy DA, Bahr GR, Kalichman SC, Morgan MG, et al. (1993) Outcome of cognitive-behavioral and support group brief therapies for depressed, HIV-infected persons. Am J Psychiatry 150: 1679–1686. [DOI] [PubMed] [Google Scholar]
- 54. Kang M, Brinthaupt TM (2009) Effects of group and individual-based step goals on children's physical activity levels in school. Pediatr Exerc Sci 21: 148–158. [DOI] [PubMed] [Google Scholar]
- 55. Paul-Ebhohimhen V, Avenell A (2009) A systematic review of the effectiveness of group versus individual treatments for adult obesity. Obes Facts 2: 17–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Chen YQ, Masse B, Wang L, Ou SS, Li X, et al. (2012) Statistical considerations for the HPTN 052 Study to evaluate the effectiveness of early versus delayed antiretroviral strategies to prevent the sexual transmission of HIV-1 in serodiscordant couples. Contemporary clinical trials 33: 1280–1286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Jia Z, Ruan Y, Li Q, Xie P, Li P, et al. (2012) Antiretroviral therapy to prevent HIV transmission in serodiscordant couples in China (2003–11): a national observational cohort study. Lancet. [DOI] [PubMed]
- 58. MacNeil JM, Mberesero F, Kilonzo G (1999) Is care and support associated with preventive behaviour among people with HIV? AIDS care 11: 537–546. [DOI] [PubMed] [Google Scholar]
- 59. Saleh-Onoya D, Reddy PS, Ruiter RA, Sifunda S, Wingood G, et al. (2009) Condom use promotion among isiXhosa speaking women living with HIV in the Western Cape Province, South Africa: a pilot study. AIDS Care 21: 817–825. [DOI] [PubMed] [Google Scholar]
- 60. Juni P, Holenstein F, Sterne J, Bartlett C, Egger M (2002) Direction and impact of language bias in meta-analyses of controlled trials: empirical study. Int J Epidemiol 31: 115–123. [DOI] [PubMed] [Google Scholar]
- 61. da Silveira MF, dos Santos IS (2006) Impact of an educational intervention to promote condom use among the male partners of HIV positive women. J Eval Clin Pract 12: 102–111. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
69 excluded studies and exclusion reasons.
(DOCX)
PRISMA Checklist.
(DOC)
Data Availability Statement
The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper.