

INTRODUCTION
Diabetes counseling is an integral part of diabetes care. Termed in current practice as diabetes self-management education and support (DSME), this therapeutic intervention helps enhance the effective of diabetes pharmacotherapy as well. Modern standards allow providers of DSME to determine how best to deliver diabetes education to their target population. They clearly mention that “needs of the individual participant will determine which parts of the curriculum will be provided” to him or her. The curriculum is expected to be “dynamic and reflect current evidence and practice guidelines”. Core topics include “using medications safely and for maximum therapeutic effectiveness”.[1]
Recent developments in diabetes pharmacotherapeutics allow a greater number of permutations and combinations with which one can manage diabetes. The use of newer, non-traditional drugs, however, comes with unique challenges as well. One such clinical situation has been described by Sethi et al. in this issue.[2] The exemplar described by the authors underscores the need for detailed history taking, and also for adequate patient education while prescribing any medication.
The importance of person-centered and medication-relevant counseling cannot be underestimated. The unique features of medication-related counseling have been discussed earlier with respect to glucagon-like peptide 1 receptor agonists.[3]
The sodium glucose transporter 2 inhibitor (SGLT2i) are a newly developed and approved class of oral anti-diabetic drugs (OADs). These compounds offer fresh options to achieve good glycemic control, without the adverse effects noticed with some of the conventional OADs. The rational use of these drugs requires an understanding of their mechanism of action, and comprehensive explanation of their usage. This editorial describes salient DSME points which must be covered in all persons taking SGLT2i therapy. Although dapagliflozin and canagliflozin are not yet available in all countries, and empagliflozin still awaits approval, physicians across the world must be aware of these facts. In today's world of enhanced mobility and communication, diabetes is no bar for travelling, and physicians may be called upon to manage people who have been prescribed such therapy in other countries.
GLUCOSURIA
SGLT2i work to achieve euglycemia by increasing glucosuria. Excretion of glucose in the urine is enhanced by inhibiting reabsorption of glucose in the proximal convoluted tubules.[4] Patients prescribed SGLT2i, and their family members, must be counseled about this mechanism and the resultant high urine glucose or urine sugar reading. This counseling must extend to health care providers such as laboratory technologists and diabetes nurses, who deal with routine biochemical reports on a daily basis.
Glucosuria has conventionally been viewed as a marker of hyperglycemia or poor control. With SGLT2i therapy, however, glucosuria becomes a marker of drug effectiveness. This simple fact may create confusion and cause distress if not explained in advance. It may be helpful to write a brief note, indicating that glucosuria may be expected with treatment, on prescriptions containing SGLT2i.
Urine glucose estimation should not be used to monitor persons on SGLT2i. Plasma glucose values and HbA1c can be used for monitoring as per current guidelines.
GENITAL INFECTIONS
By their mechanism of action, SGLT2i increase the glucose load in the urinary tract. While this has not been shown to increase the risk of urinary tract infections (UTIs), it does pre-dispose patients to genital tract infections (GTIs). These are usually fungal in nature, and can present as vulvitis in woman, and balanaposthitis or balanitis in men.[5] Uncircumcised men are more prone to fungal GTIs. It must be noted that fungal GTIs can be a presenting symptom of diabetes, are a clinical feature of poorly controlled diabetes, and may also be sexually transmitted diseases (STDs). Not every person on SGLT2i with GTI, therefore, will have this infection as a direct consequence of drug therapy. Achieving euglycemia, in fact, will reduce the predisposition to all infections.
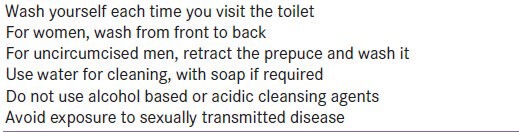
GTIs can easily be prevented and managed.[6] Detailed counseling about maintenance of perineal hygiene should be included in all diabetes education sessions, irrespective of which therapy is prescribed. Ideally, such counseling should pre-empt infection, rather than be a reactive measure. Important points related to perineal hygiene are listed in Table 1. Repeated counseling regarding perineal hygiene will be necessary for persons on SGLT2i.
Table 1.
Counseling tips for perineal hygiene
In case a fungal GTI does develop, it can easily be managed by local or systemic means, which can be patient-initiated or physician-initiated. Local measures such as antifungal creams and powders are often effective, as are oral antifungal agents. Many persons in hot, humid climates such as South Asia use antifungal powders for local perineal application on a prophylactic basis. Anerobic coverage may be required for GTIs which do not respond to antifungal treatment. Subjects who are unable to visit healthcare facilities regularly, or who are at high risk of developing GTIs (for e.g. immune-compromised persons) may be counseled regarding the rational use of patient –initiated antifungal therapy.[7]
FLUID/ELECTROLYTE BALANCE
SGLT2i create an osmotic diuresis which has the potential to cause volume depletion and hypotension. Clinical trial data reveals that this is an uncommon adverse event. The extra diuresis causes by SGLT2i is about 350-400 ml per day, which is equal to one extra void. This urine output is spread throughout the day, and does not cause nocturia.[8]
However, the South Asia clime presents health challenges in the form of heat exhaustion, hypovolemia and electrolyte imbalance. There is a theoretical risk of worsening of fluid electrolyte homeostasis with SGLT2i treatment.
Counselling must include advice to maintain adequate fluid and electrolyte intake, and awareness about symptoms of dyselectrolytemia. One should also ensure that SGLT2i are not coprescribed with loop diuretics.[9] There is no need to monitor serum electrolytes or renal function tests in persons on chronic SGLT2i management.
CONCLUSIONS
The role of the diabetes care professional team member has expanded in recent years. Diabetes care providers such as educators, nurses and pharmacists are expected to keep abreast of advances in diabetes pharmacology. The use of the modern class of SGLT2i creates new opportunities for diabetes management.[10] However, their optimal use requires concurrent counseling regarding the mechanism of action, monitoring and followup of patients on SGLT2i. This fact is underscored by recent research, which reveals that safe use of medication is a major part of diabetes counseling.[11]
Integrating the points mentioned in this communication as part of routine diabetes counseling and education, especially in persons on SGLT2i, will help ensure appropriate glycemic management.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Haas L, Maryniuk M, Beck J, Cox CE, Duker P, Edwards L, et al. National standards for diabetes self-management education and support. Diabetes Care. 2013;36:S100–8. doi: 10.2337/dc13-S100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kelwade J, Sethi BK, Nagesh V, Vaseem A. A case of pseudo-ketoacidosis. Indian J Endocrinol Metab. 2014;18:743. doi: 10.4103/2230-8210.139228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kalra S, Kalra B. Counselling patients for GLP-1 analogue therapy: Comparing GLP-1 analogue with insulin counselling. N Am J Med Sci. 2012;4:638–40. doi: 10.4103/1947-2714.104315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hummel CS, Lu C, Loo DD, Hirayama BA, Voss AA, Wright EM. Glucose transport by hman renal NA+/D-glucose cotransporters SGLT1 and SGLT2. Am J Physiol Cell Physiol. 2011;300:C14–21. doi: 10.1152/ajpcell.00388.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Johnsson KM, Ptaszynska A, Schmitz B, Sugg J, Parikh SJ, List J. Vulvovaginitis and balanitis in patients with diabetes treated with dapagliflozin. J Diabetes Complications. 2013;27:479–84. doi: 10.1016/j.jdiacomp.2013.04.012. [DOI] [PubMed] [Google Scholar]
- 6.Wilding J, Woo V, Soler NG, Pahor A, Sugg J, Rohwedder K, et al. Long-term efficacy of dapagliflozin in patients with type 2 diabetes mellitus receiving high doses of insulin. Dtsch Med Wochenschr. 2013;138:27–38. doi: 10.1055/s-0032-1305284. [DOI] [PubMed] [Google Scholar]
- 7.Jovanovic R, Congema E, Nguyen HT. Antifungal agents vs. boric acid for treating chronic mycotic vulvovaginitis. J Reprod Med. 1991;36:593–7. [PubMed] [Google Scholar]
- 8.Scheen A. Evaluating SGLT2 inhibitors for type 2 diabetes: Pharmacokinetic and toxicological considerations. Expert Opin Drug Metab Toxicol. 2014;10:647–63. doi: 10.1517/17425255.2014.873788. [DOI] [PubMed] [Google Scholar]
- 9.Kilov G, Leow S, Thomas M. SGLT2 inhibition with dapagliflozin--a novel approach for the management of type 2 diabetes. Aust Fam Phys. 2013;42:706–10. [PubMed] [Google Scholar]
- 10.Poudel RR. Renal glucose handling in diabetes and sodium glucose cotransporter 2 inhibition. Indian J Endocrinol Metab. 2013;17:588–93. doi: 10.4103/2230-8210.113725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Halkoaho A, Kangasniemi M, Niinimäki S, Pietilä AM. Type 2 diabetes patients’ perceptions about counselling elicited by interview: Is it time for a more health-oriented approach? Eur Diabetes Nurs. 2014;11:13–8. [Google Scholar]