

Giant cell arteritis (GCA) has a predilection for the extracranial branches of the carotid artery. Classic manifestation of the disease is scalp tenderness and jaw claudication and the temporal artery may appear swollen and pulseless. The disease may affect all organs but the most feared complication is sudden, irreversible blindness. Furthermore, polymyalgia rheumatica is often associated with GCA. The aetiology of both disorders is currently unknown.[1,2]
GCA is reported to have an uneven geographical distribution.[3] From a Danish perspective it is a relatively common disorder with more than 300 annual inpatient contacts from a background population of five million people [Figure 1].[4,5] However, GCA is thought to be rare in the developing countries and in patients of Asian background.[3]
Figure 1.
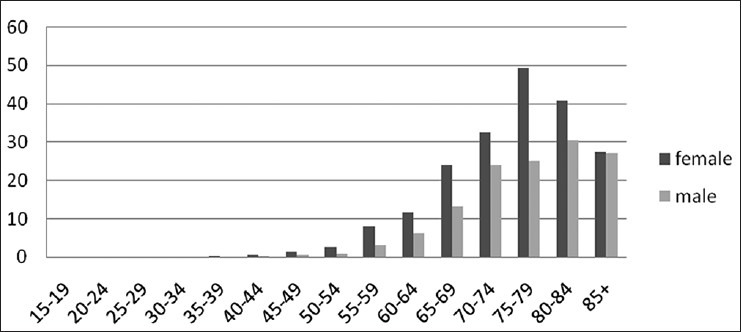
The age-specific rate of Inpatient contacts due to GCA in Denmark in the period 2009-2012. Source
GCA is easy to diagnose and must be suspected in the patients aged over 50 years, with an increased erythrocyte sedimentation rate, and general symptoms of myalgia or headache. The gold-standard for GCA diagnosis is still the temporal artery biopsy, but clinicians need to be aware that false negative results may occur. It is of importance to diagnose GCA since the treatment with glucocorticoids often lead to rapid improvement. The standard treatment regimen is a high-dose glucocorticoid therapy (60 mg/day) which is gradually reduced over several months.[2]
In conclusion, the diagnosis and the treatment of GCA should be common knowledge to all neurologists, and symptoms of this disease must not be misinterpreted as tension type headache or opticneuritis.[6,7]
References
- 1.Weyand CM, Goronzy JJ. Medium and large-vessel vasculitis. N Engl J Med. 2003;349:160–9. doi: 10.1056/NEJMra022694. [DOI] [PubMed] [Google Scholar]
- 2.Mackie SL, Pease CT. Diagnosis and management of giant cell arteritis and polymyalgia rheumatica: Challenges, controversies and practical tips. Postgrad Med J. 2013;89:284–92. doi: 10.1136/postgradmedj-2012-131400. [DOI] [PubMed] [Google Scholar]
- 3.Lee JL, Naguwa SM, Cheema GS, Gershwin ME. The geo-epidemiology of temporal (giant cell) arteritis. Clin Rev Allergy Immunol. 2008;35:88–95. doi: 10.1007/s12016-008-8075-0. [DOI] [PubMed] [Google Scholar]
- 4.The National Registry of Patients. Ref Type: Online Source. 2012 [Google Scholar]
- 5.Statistics Denmark. Ref Type: Online Source. 2012 [Google Scholar]
- 6.Horwitz H, Friis T, Modvig S, Roed H, Tsakiri A, Laursen B, et al. Differential diagnoses to MS: Experiences from an optic neuritis clinic. J Neurol. 2014;261:98–105. doi: 10.1007/s00415-013-7166-x. [DOI] [PubMed] [Google Scholar]
- 7.Rana AQ, Saeed U, Khan O, Qureshi AM, Paul D. Giant cell arteritis or tension-type headache. A differential diagnostic dilemma? J Neurosci Rural Pract. 2014;4:409–411. doi: 10.4103/0976-3147.140005. [DOI] [PMC free article] [PubMed] [Google Scholar]