

Abstract
Background:
Endotracheal intubation is important to carry out various surgical procedures. The estimation of endotracheal tube size is governed by narrowest diameter of the upper airway. The objective of the study was to assess the narrowest tracheal diameter by ultrasound for selection of the appropriate size endotracheal tube.
Materials and Methods:
After the approval of institution ethical committee and written informed consent, 112 patients aged 3 to 18 years of both genders with normal airways, scheduled for surgery under general anesthesia and intubation, were enrolled for this prospective clinical observational study. Preanesthetic ultrasonography of the subglottic region was performed by experienced ultrasonologist with a high-resolution linear array transducer in sniffing position for every patient and the subglottic tracheal diameter was estimated to select the appropriate-size endotracheal tube. The endotracheal tube, calculated on the basis of physical indices and by ultrasound, was statistically correlated with the appropriate size endotracheal tube used clinically for intubation.
Results:
The ultrasound guided selection criterion has estimated the appropriate-sized endotracheal tube better than physical indices (age or height)-based formulas. The estimated endotracheal tube size by ultrasound was significantly correlated with the clinically used endotracheal tube.
Conclusion:
Ultrasonography may be used for the assessment of the subglottic diameter of trachea in children to estimate the appropriate size endotracheal tube for intubation.
Keywords: Endotracheal tube, subglottic diameter, ultrasound, upper airway
INTRODUCTION
Endotracheal intubation is essential for airway maintenance and adequate ventilation to carry out various surgical procedures usually without any complications. The oversized endotracheal tube relative to trachea or over-inflated cuff between tube and anatomic structures, may damage the tracheal mucosa by friction and compressions, can cause airway edema, postextubation stridor, subglottic stenosis, or cartilaginous ischemia, especially in children.[1] On the other hand, the smaller endotracheal tube will increase the resistance to gas flow and risk of aspiration, insufficient ventilation, and poor monitoring of end tidal gases.[2] The level of the cricoid cartilage plays an important role for selection of the appropriate size endotracheal tube being the narrowest diameter of upper airway.[3]
The cervical radiograph and age-based physical indices do not reflect the actual tracheal diameter for selection of endotracheal tube and repeated laryngoscopies are often necessary to identify the proper endotracheal tube for intubation in each patient. To avoid excessive airway instrumentation and minimizing the risk of trauma, the preanesthetic assessment of tracheal diameter is essential to select the appropriate endotracheal tube.[4,5]
Recent studies have documented that the anatomical structures in the supra-glottic, glottis, and subglottic regions can be determined by ultrasonography. The ultrasonography could be a reliable, safe, and noninvasive pain free modality for evaluation of the upper airway's narrowest transverse diameter at the subglottic region and may be helpful to estimate the proper size endotracheal tube. Ultrasound offers a number of advantages compared to other competitive imaging modalities.[6,7,8] The aim of this study was to assess the narrowest transverse diameter of trachea at the subglottic region by ultrasound to estimate the appropriate-sized endotracheal tube.
MATERIALS AND METHODS
After approval of Institutional Ethical Committee and written informed consent, 112 consecutive patients of both genders aged 3 to 18 years with normal airway were enrolled for this prospective study from November 2010 to October 2011. These patients were scheduled for surgery requiring general anesthesia with endotracheal intubation. The patients suffering from any respiratory disease that might cause airway narrowing, pre-exiting laryngeal or tracheal pathology, any lesion that could cause airway deformity due to fibrosis or difficult airway was anticipated were excluded from the study. Exclusion criterions were used to minimize statistical bias due to inherited or acquired abnormalities that might cause narrowing of the airway.
Technique of ultrasonography
The subglottic diameter was estimated with high resolution B-mode ultrasonography (Toshiba- Apilo) with a linear probe of small footprint (40 mm length, frequencies 7 to 15 MHz) positioned on the midline with their head extended and neck flexed (the sniffing position) [Figure 1]. The standard scanning plane was predetermined to prevent any examination bias and artifacts. The patients were instructed to take a slow inspiration at constant flow during the measurement period to minimize respiratory-induced changes in upper airway dimensions. Ultrasonography, performed by an experienced person, began with location of the true vocal cords, seen as paired hyperechoic linear structures with respiratory and swallowing mobility and then moved caudally to visualize the cricoid arch to avoid any confusion between the cricoid cartilage and the tracheal ring. The transverse air column diameter was measured at the cephalic half of the cricoid cartilage that is narrower than the caudal part and was considered as tracheal diameter. The larynx is situated below the hyoid bone, and the ring-shaped trachea, located inferior to the cricoid cartilage, can be easily visualize by ultrasound in vertical or transverse section[8,9,10] [Figure 2].
Figure 1.

Patient's position and USG technique
Figure 2.

Measurement of tracheal diameter by USG at the subglottic region
General anesthesia was induced with propofol (2 mg kg1) and muscular relaxation was achieved with rocuronium (0.08 mg kg1) to facilitate the endotracheal intubation under direct laryngoscopy. The predetermined-sized endotracheal tube, estimated by ultrasonography, was used. Endotracheal tube size was considered optimal when the tracheal leak was detected at an inflation pressure of 10-20 cm H2O.[11] The cuff leak test was done by one of the authors. If there was resistance to ETT passage into the trachea, or there was no audible leak when the lung were inflated to a pressure of 20 to 30 cm H2O, the tube was exchanged with one that was 0.5 mm smaller. But if a leak occurred at an inflation pressure of less than 10 cm of H2O, the ETT was exchanged for one with the 0.5 mm larger tube.
The relationship between calculated external diameters of the endotracheal tube from physical indices of age-based formulas, predetermined by ultrasound and clinically used ETT for intubation during general anesthesia was done.
Statistical analysis
The results obtained in the study were presented in tabulated manner and analyzed using Microsoft Excel and SPSS 10.0 for windows. Statistical significance in mean difference was done using student t-test. The BlandAltman method and linear regression were used to compare the ETT diameter predicted from age-based formula, estimated tracheal diameter by ultrasound and clinically optimally used ETT diameter. The results were expressed as mean diameter ± SD. P < 0.05 was considered statistically significant with 95% confidence.
RESULTS
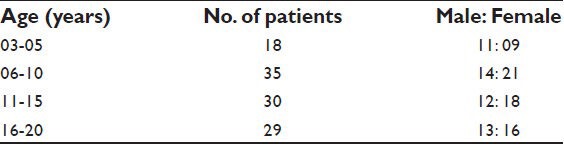
The demographic and morphometric characteristics of all 112 patients were comparable [Table 1]. All patients underwent ultrasonography without technical difficulty and the procedure never exceeded more than 3 min to measure the tracheal diameter adequately. We were able to visualize all relevant anatomic structures of upper airway in all the patients by a linear probe of small footprint (40 mm length, frequencies 7 to 15 MHz) positioned on the midline with their head extended and neck flexed. The predetermined ultrasound technique has made a comparable study possible through the unanimous anatomical-section plane by different investigators.
Table 1.
Demographic data of patients
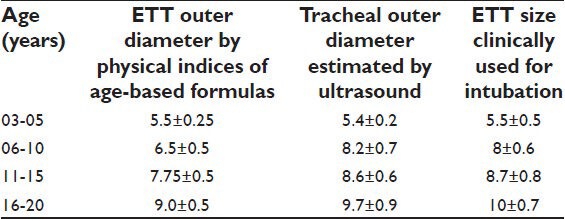
The clinically optimal verses predicted diameter of ETT with age-based formulas was only 35% for cuffed tubes while there was a strong corelation between subglottic tracheal diameters estimated by ultrasonography and clinically used endotracheal tube for intubation [Table 2]. By the Bland Altman analysis, the rate of agreement between clinically optimal and ultrasound guided endotracheal tube was 98% (P < 0.001).
Table 2.
Correlation and comparative evaluation of the endotracheal tube
DISCUSSION
Endotracheal intubation is most commonly performed procedure, but can lead to complications due to improper size of the endotracheal tube. The smaller diameter tubes are easier to insert and require less force to adapt to the patient's airway but are associated with higher resistance, difficulty in passing a suction catheter and increased risk of occlusion, aspiration, and kinking with insufficient ventilation. The larger tubes are associated with higher incidence of postoperative sore throat, may damage the tracheal mucosa, can cause airway edema, postextubation stridor, subglottic stenosis due to inflated cuff.[1,2] Moreover, there is great variation in size and shapes of trachea and the correlation between age, height, weight, body surface area and tracheal shape or size is poor. At present, the endotracheal tube is selected according to age and height based formulas, which generally predicted either smaller or larger sizes than proved clinically optimal and there is disparity between age- and height-based formulas and clinically used optimal ETT size.[12,13,14,15]
This study has revealed the potential utility of ultrasound to measure the transverse diameter of upper airway at subglottic region for selection of the appropriate-sized endotracheal tube. The tracheal diameter measurement consistently was difficult due to the blurred visualization of the vocal cord by ultrasound therefore the subglottic diameter was assessed.[6] The study showed that direct measurement of subglottic diameter by ultrasonography has significant advantages in predicting the optimal ETT size. This study has shown the higher correlation between clinically used endotracheal tubes and predetermined endotracheal tubes by ultrasonography than predicted endotracheal tube by age and height based formulas.
The measurement of tracheal diameter may be performed using noninvasive methods such as chest x-ray, CT, MRI, or ultrasonography and invasively by endoscopy. The optimal ETT size could be selected from the measurement of the tracheal diameter on chest radiography. A good correlation in tracheal diameter between computed tomography and chest radiography indicates that the CT could give a representative measurement of tracheal diameter.[16] But the high-quality laryngeal images provided by CT and MRI are not routinely obtained because of cost and feasibility and the assessment of laryngeal dimensions may be overestimated as shape of the subglottic area is frequently un-cylindrical.[17]
Recent report on the feasibility of ultrasonography to examine the subglottic diameter showed a strong correlation between ultrasonography and magnetic resonance image (MRI) measurements of the transverse subglottic diameter, suggests that ultrasound could predict the subglottic diameter adequately.[18] This noninvasive tool does not require strict immobility, especially in infants, as opposed to MRI or CT scan, for which infants are often anesthetized. Ultrasonography is operator dependent technique but it is relatively simple to learn. The age dependent physiological calcification of the larynx does create an acoustic shadow but in our patients calcifications of the cricoid arch did not disturb the measurement.
CONCLUSION
Ultrasonography is a safe reliable noninvasive reproducible method for preanesthetic estimation of the subglottic tracheal diameter for selection of appropriately size endotracheal tube for clinical use and our study validates the reliability of ultrasound to measure subglottic diameter to avoid intubation related complications of either trauma or inefficient ventilation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Weiss M, Dullenkopf A, Gysin C, Dillier CM, Gerber AC. Shortcomings of cuffed paediatric tracheal tubes. Br J Anaesth. 2004;92:78–88. doi: 10.1093/bja/aeh023. [DOI] [PubMed] [Google Scholar]
- 2.Roy WL. Intraoperative aspiration in a paediatric patient. Can Anaesth Soc J. 1985;32:639–41. doi: 10.1007/BF03011411. [DOI] [PubMed] [Google Scholar]
- 3.Randestad A, Lindholm CE, Fabian P. Dimensions of the cricoid cartilage and the trachea. Laryngoscope. 2000;110:1957–61. doi: 10.1097/00005537-200011000-00036. [DOI] [PubMed] [Google Scholar]
- 4.Oshodi A, Dysart K, Cook A, Rodriguez E, Zhu Y, Shaffer TH, et al. Airway injury resulting from repeated endotracheal intubation: Possible prevention strategies. Pediatric Crit Care Med. 2011;12:117–8. doi: 10.1097/PCC.0b013e3181dbeb28. [DOI] [PubMed] [Google Scholar]
- 5.Sherman JM, Nelson H. Decreased incidence of subglottic stenosis using an “appropriate-sized” endotracheal tube in neonates. Pediatr Pulmonol. 1989;6:183–5. doi: 10.1002/ppul.1950060311. [DOI] [PubMed] [Google Scholar]
- 6.Lakhal K, Delplace X, Cttier JP, Tranquart F, Sauvagnae X, Mercier C, Fusciardi J, Laffon M. The feasibility of ultrasound to assess subglottic diameter. Anesth Anal. 2007;104:611–4. doi: 10.1213/01.ane.0000260136.53694.fe. [DOI] [PubMed] [Google Scholar]
- 7.Shibasaki M, Nakajima Y, Shimizu F, Shime N. Prediction of Pediatric Endotracheal Tube Size by Ultrasonography. Anesthesiology. 2010;113:819–24. doi: 10.1097/ALN.0b013e3181ef6757. [DOI] [PubMed] [Google Scholar]
- 8.Carp H, Bundy A. A preliminary study of the ultrasound examination of the vocal cords and larynx. Anesth Analg. 1992;75:639–40. doi: 10.1213/00000539-199210000-00042. [DOI] [PubMed] [Google Scholar]
- 9.Strauss S. Sonographic appearance of cricoid cartilage calcification in healthy children. Am J Roentgenol. 2000;174:223–8. doi: 10.2214/ajr.174.1.1740223. [DOI] [PubMed] [Google Scholar]
- 10.Raghavendra B, Horii S, Reede DL, Rumancik WM, Persky M, Bergeron T. Sonographic anatomy of the larynx, with particular reference to the vocal cords. J Ultrasound Med. 1987;6:225–30. doi: 10.7863/jum.1987.6.5.225. [DOI] [PubMed] [Google Scholar]
- 11.Schwartz RE, Stayer SA, Pasquariello CA. Tracheal tube leak test-is there inter-observer agreement? Can J Anaesth. 1993;40:1049–52. doi: 10.1007/BF03009476. [DOI] [PubMed] [Google Scholar]
- 12.Bourne TM, Barker I. External diameter of paediatric tracheal tubes. Anaesthesia. 1993;48:83–9. [Google Scholar]
- 13.Malhotra SK, Dutta A. Paediatric endotracheal tubes: the advantage of outer diameter. Anaesth Analg. 2001;93:801–2. doi: 10.1097/00000539-200109000-00053. [DOI] [PubMed] [Google Scholar]
- 14.Eck JB, Dc Lisle, Dear G, Phillips BG, Ginsberg B. Prediction of tracheal tube size in children using multiple variables. Paediatric Anaesthesia. 2002;12:495–8. doi: 10.1046/j.1460-9592.2002.00894.x. [DOI] [PubMed] [Google Scholar]
- 15.Hofer CK, Ganter M, Tucci M, Klaghofer R, Zollinger A. How reliable is length based determination of body weight and tracheal tube size in paediatric age group: The Broselow tape reconsidered. Br J Anaesth. 2002;88:283–5. doi: 10.1093/bja/88.2.283. [DOI] [PubMed] [Google Scholar]
- 16.Kormano M, Yrjana J. The posterior tracheal band: Correlation between computed tomography and chest radiography. Radiology. 1980;136:689–94. doi: 10.1148/radiology.136.3.7403548. [DOI] [PubMed] [Google Scholar]
- 17.Eckel HE, Sittel C, Zorowka P, Jerke A. Dimensions of the laryngeal framework in adults. Surg Radiol Anat. 1994;16:31–6. doi: 10.1007/BF01627918. [DOI] [PubMed] [Google Scholar]
- 18.Hatfield A, Bodenham A. Ultrasound: An emerging role in anaesthesia and intensive care. Br J Anaesth. 1999;83:789–800. doi: 10.1093/bja/83.5.789. [DOI] [PubMed] [Google Scholar]