

Abstract
General anesthesia and neuraxial blockade have their own advantages and disadvantages over each other when used for hip surgery. Single shot lumbar plexus block can be the choice of the anesthetic technique for postrenal transplant, immunocompromised, postspinal surgery patient to undergo dynamic hip screw surgery.
Keywords: Compromised patient, hip surgery, lumbar plexus block
INTRODUCTION
The lumbar plexus block is used for postoperative analgesia after hip and knee surgery all over the world and accepted as a simple and relatively safe procedure.[1] This procedure can be used as the sole anesthetic method for lower limb surgery involving hip, knee, and anterior thigh.
CASE REPORT
A 57-year-old gentleman with body weight of 60 kg having type-2 diabetes mellitus, hypertension, post-transplant recipient of renal allograft done 3 months ago was posted for right-sided dynamic hip screw fixation [Figure 1]. He was on tab Tacrolimus 3 mg and tab Prednisolone 12.5 mg once daily as immunosuppressant and Human insulin mixtard. For the last 12 days, he had been suffering from diarrhea that was not being controlled despite medical therapy. We had to choose the best anesthetic procedure for him. Thus lumbar plexus block was chosen unanimously.
Figure 1.

X ray showing right hip fracture
During pre anesthetic check up, the patient was conscious, oriented having anemia, dehydration and hypotension with blood pressure ranging from 86-90/50-60 mm hg. Chest infection was evident by the presence of bilateral rhonchi and crepitations, chest x-ray showing hilar congestions. His pulse rate was 101/min. He was a febrile. Echocardiography showed mild mitral regurgitation, grade 1 diastolic dysfunction with ejection fraction of 58%. Electrocardiogram (EKG) showed sinus tachycardia with left axis deviation. Blood investigations were: Hemoglobin 9.5 gm/dL, total leucocyte count 4500/cumm, platelet count 2 lac/cumm, Prothrombin time 13.9, International Normalised Ratio 1.23, Activated Partial Thromboplastine Time 34 (control 25), urea 48 mg/dL, creatinine 1.58 mg/dL, postprandial sugar 148 mg/dL, serum sodium 128 mmol/lt, serum potassium was 5 mmol/lt, Chloride-97 mmol/lt and urine output 70 mL/h.
Further enquiry revealed he had undergone spinal fixation surgery at the level of lumbar 1 and 2 vertebrae 8 months ago [Figure 2]. The patient was optimised with one unit packed cell, crystalloids, nebulization, and intravenous antibiotics. His hemoglobin increased to 10.6 gm/dL. Blood pressure improved to 95-100/65-70 mmHg and partial haemoglobin saturation (SPO2) 97% with O2 through face mask @ 1 L/min.
Figure 2.
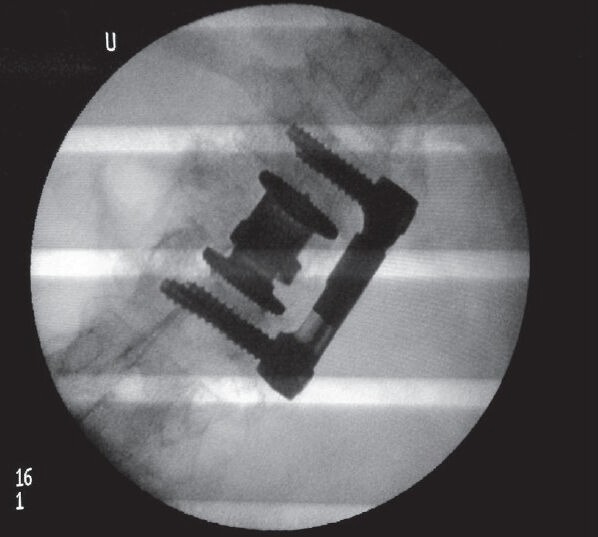
X-ray showing lumbar spine fixed with prosthesis
In operation theatre, we attached monitors (EKG, SPO2). Arterial blood pressure and central venous pressure monitoring were also done. The patient was put in the left lateral position with O2 flow 2 L/min through face mask. Landmarks were identified for the posterior approach of the lumber plexus block. The spinous processes of Lumbar 4,5 vertebrae vertebrae were identified. A parallel line to the spinous process line was then drawn, originating from the posterior superior iliac spine (parasagittal line). Next, a vertical line was drawn at the level of the highest point on the iliac crest (intercrestal line). The intersection of the intercrestal line with the parasagittal line determined the site of introduction of the needle [Figure 3]. A single bolus lumbar plexus block[2] was given using 100 mm 21 gauge insulated needle with nerve stimulator (1.5 mA, 2 Hz, 0.1 ms) with 10 mL of 2% Xylocaine and 20 mL of 0.5% Bupivacaine. The stimulation of the femoral nerve produced a quadriceps contraction and a patella snap. After appropriate positioning of the needle maintaining the motor response with a current of less than 0.5 mA and negative aspiration for blood, 2 mL of 2% xylocaine was slowly injected. The patient was asked to move feet to verify that the injection is not intrathecal. Then each 5 mL of local anesthetic was injected slowly alternating with repeated aspiration for blood. Sensory block was elicited by ice packs. Complete sensory and motor blockade were achieved within 25 min after the procedure. Two milliliter of Midazolam and 25 μg of Fentanyl were used as sedatives. The procedure was completed within one hour and 15 min without appreciable blood loss. Patient remained haemodynamically stable throughout the procedure. In the recovery room return of motor block was found after 3 h and sensory after 31/2 h from the time of injection.
Figure 3.

Landmarks for lumbar plexus block
DISCUSSION
We approached the lumbar plexus block to avoid hemodynamic disturbances due to neuraxial blockade[3] as well as ambiguity of neuraxial block after spine surgery and prolonged systemic effects of intravenous anesthetics after general anesthesia and simultaneously avoided airway handling. This was dynamic hip screw fixation for which small incision was required involving lateral aspect of hip supplied by lateral femoral cutaneous branch of femoral nerve that was effectively blocked. Obturator and accessory obturator nerves (if any) were also blocked perfectly apart from femoral nerve supplying hip joint.[4] The sciatic nerve block was not necessary as neither posterior extension of incision nor any hip movement was required as in other type of hip surgeries.
We had to opt for general anesthesia for failure of block or prolonged surgery as continuous nerve block was not done to avoid probable drug toxicity in the view of compromised status. Hence, single bolus lumbar plexus block was perhaps the best option[5] in anesthetizing this patient with these co-morbidities and depressed immunity.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Winnie AP, Ramamurthy S, Durrani Z, Radonjic R. Plexus blocks for lower extremity surgery. Anaesthesiol Rev. 1974;1:11–6. [Google Scholar]
- 2.Stevens RD, van Gessel E, Flory N, Fournier R, Gamulin Z. Lumbar plexus block reduces pain and blood loss associated with total hip arthroplasty. Anesthesiology. 2000;93:115–21. doi: 10.1097/00000542-200007000-00021. [DOI] [PubMed] [Google Scholar]
- 3.Eyrolle L, Zetlaoui P, Belbachir A, Rosencher N, Conseiller C. Regional anesthesia for femoral neck fracture surgery: Comparison of lumbar plexus block and spinal anesthesia. Br J Anaesth. 1998;80:A383. [Google Scholar]
- 4.GRAY's Anatomy. 40th ed. Chapter 81. London U.K: Churchill Livingstone Elsevier; 2008. Hip-Innervation. [Google Scholar]
- 5.Eker HE, Kocum A, Kocum T, Turkoz A, Arslan G. Severe Aortic Stenosis: Combined Lumbar Plexus, Sciatic and Iliohypogastric Nerve Block with 0.25% Levobupivacaine for Reduction of Hip Fracture. Internet J Anesthesiol. 19 No.2. Available from: http://www.ispub.com:80/journal/the-internet-journal-of-anesthesiology/vol-19-No2 . [Google Scholar]