

Abstract
It is known that, unilateral thoracic paravertebral block (TPVB) applications performed with general anesthesia provide satisfactory conditions for open cholecystectomy increase the quality of post-operative analgesia and patient comfort and decrease the frequency of post-operative nausea and vomiting. In this case report, the TPVB was presented which was performed for two patients with high risk of anesthesia who have been planned to undergo open cholecystectomy.
Keywords: Analgesia, anesthesia, open cholecystectomy, paravertebral block, thoracic
INTRODUCTION
Open cholecystectomy surgery is a surgical procedure often requires general anesthesia and endotracheal intubation.[1,2] This procedure may also be performed by applying a high thoracic epidural block, combined spinal-epidural and spinal anesthesia. The anesthesiologists mostly concern for the complications, which will be able to occur in patients with severe heart disease and chronic obstructive pulmonary disease (COPD). Both thoracic epidural anesthesia and general anesthesia may be applied for this type of medical problems encountered.
Thoracic paravertebral block (TPVB) provides high quality analgesia and great advantages in many types of surgery.[2,3,4] TPVB is an alternative method to general anesthesia and thoracic epidural block due to provide safe anesthesia with more stable hemodynamic response than thoracic epidural block and characterized by a low side-effect profile. It has been purposed to present application of unilateral TPVB for patients with serious comorbidities who were planned open cholecystectomy and considered as could not be tolerated hemodynamic responses of general anesthesia or neuroaxial blocks.
CASE REPORTS
Case 1
In an 84-year-old, 68 kg, 180 cm tall male patient's electrocardiography (ECG) normal sinus rhythm was observed. In his echocardiography, 30% ejection fraction, mild mitral and aortic regurgitation were determined. Unilateral TPVB was planned in order to anesthesia for American Society of Anesthesiologists’ (ASA) III patient with moderate COPD (the pulmonary function tests within the normal range) before surgical incision. The patient was monitored by taking regional anesthesia treatment room. The patient's heart rate (HR); 65 beats/min, non-invasive arterial blood pressure (BP); 103/65 mmHg, fingertip arterial oxygen saturation (SpO2) was 95%. Oxygen was given with 2 L/min flow by mask and total of 2 mg dose of intravenous midazolam with increasing doses and 50 μg dose of fentanyl were administered in order to sedation.
Injection sites were determined at left lateral decubitus position. Under aseptic conditions, local anesthesia with 2% lidocaine was performed to skin and subcutaneous tissues. From 2.5 cm right lateral to Th7 vertebrae by using 18-gauge 80-mm atraumatic neurostimulator (Contiplex E, B. Braun Melsungen AG, Germany) block needle, after touched 3 cm depth of transverse ledge by directing the needle to 2 cm caudally, paravertebral space was entered [Figure 1]. With the help of neurostimulator, after observing the contraction of the abdominal muscles at 0.5 mA and aspiration, “single shot” 20 mL dose of 0.5% levobupivacaine was injected and the catheter was inserted. After the supine position of patient's, bradycardia (40 beats/min) occurred at 5 min, 0.5 mg atropine was administered intravenously. After administration of atropine HR; 66 beats/min, BP; 107/56 mmHg and SpO2 was 97%. Sensory block was determined by applying pick prick and hot-cold test for Th4 and Th9 dermatomes.
Figure 1.
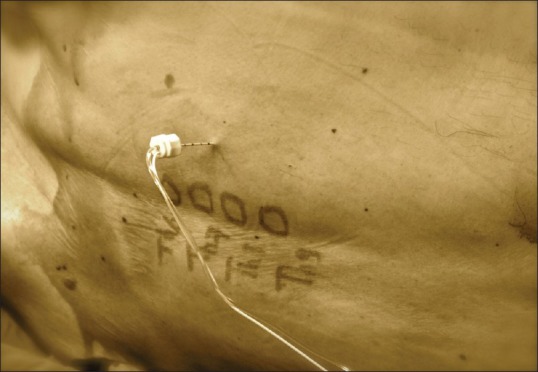
Thoracic paravertebral block applied with neurostimulator
The patient was applied standard monitoring by taking to the operation room after 25 min of the block administration. Twenty minutes after the surgical procedure, due to BP was measured as 65/44 mmHg, 5 mg dose of ephedrine was administered intravenously and BP was measured as 103/68 mmHg. Continuation of the operative procedure, the patient's vital signs were within normal limits.
The surgical procedure lasted 75 min. Additional sedation and analgesia were not required during the surgical procedure. The patient was followed for 30 min at the post-operative recovery room and referred to the surgical ward due to the patient's hemodynamic and respiratory parameters were measured within normal limits. The patient did not have post-operative nausea and vomiting and pain after surgery. Nine hours after surgery, due to visual analog scale (VAS) was 5, 1 g dose of paracetamol was administered intravenously. Additional analgesic treatment was not required. Post-operative 3th day, the patient was discharged without any problem.
Case 2
The second case describes about a 59-year-old male patient, with weighing 78 kg and height 178 cm. His ECG sinus rhythm was observed. According to the findings of echocardiography, left atrium was dilated and ejection fraction was 60%. In the cranial computed tomography of the patient with left hemiparesis at upper and lower extremities, right total MCA (middle cerebral artery) infarction signs were seen related with previous cerebrovascular event. There were no pathologic signs in the other systemic examination and routine laboratory tests. Pre-operative evaluation of patients was ASA III. Before open cholecystectomy, TPVB was planned in order to anesthesia for the patient.
The patient was monitored by taking regional anesthesia treatment room. The patient's HR; 90 beats/min, arterial BP; 150/100 mmHg, SpO2 was 93%. Oxygen was given with 2 L/min flow by mask and total of 2.5 mg dose of intravenous midazolam with increasing doses and 75 μg dose of fentanyl were administered in order to sedation.
Injection sites were determined in a sitting position. Under aseptic conditions, 2% lidocaine was administered to skin and subcutaneous tissues. From 2.5 cm right lateral to Th7 vertebrae by using 18-gauge 80-mm atraumatic neurostimulator (Contiplex E, B. Braun Melsungen AG, Germany) block needle, after touched 2.5 cm depth of transverse ledge, paravertebral space was entered in 4 cm of depth. With the help of neurostimulator, after observing the contraction of the abdominal muscles at 0.5 mA and aspiration, “single shot” 20 ml dose of 0.5% levobupivacaine was injected and the patients was lied in the supine position and the catheter was inserted to paravertebral region.
After application of block, HR; 63/min, BP; 140/100 mmHg, SpO2 was 92%. Unilateral sensory block was determined by applying pick prick and hot-cold test for the right side Th4 and Th8 dermatomes.
After 25 min from block application, the patient was taken to the operation room and after the application of standard monitoring, propofol infusion of 2 mg/kg/h was started. Fifteenth minute of the operative procedure, during hepatic retraction, the patient felt pain, therefore 100 mcg fentanyl and 100 mg of propofol (a total of 180 mg doses of propofol during the operation) were administered intravenously. HR of the patients after the sedoanalgesia 56 beats/min, BP; 114/68 mmHg and SpO2 were measured as 97%.
The surgical procedure lasted 75 min. The patient was followed for 30 min at the post-operative recovery room and referred to the surgical ward due to the patient's hemodynamic and respiratory parameters were measured within the normal limits. The patient did not have post-operative nausea and vomiting and pain after surgery. Twelve hours after the surgery, due to VAS was 5, 1 g dose of paracetamol was administered intravenously. Additional analgesic treatment was not required. On the 6th post-operative day, he was discharged without any problem.
DISCUSSION
There are some regional methods can provide surgical anesthesia for patients with cardiopulmonary diseases who will be performed open cholecystectomy. Thoracic epidural block, which is the most common method as a regional anesthesia among these methods besides providing bilateral symmetric anesthesia, creates sympathetic block and accompanying hemodynamic instability. Furthermore, terrible fears of complications such as epidural hematoma in patients using anticoagulation causes to avoid the anesthetists to perform the application of thoracic epidural block.
The number of scientific publications about TPVB application for cholecystectomy is very limited and the results are controversial.[1,5,6] It has been reported that the applications of unilateral TPVB with general anesthesia provide satisfactory conditions for open cholecystectomy, increase the quality of post-operative analgesia and patient comfort and decrease the frequency of post-operative nausea and vomiting than in patients under only general anesthesia. In their study Giesecke et al.[5] have investigated the effects of peri-operative stress response of paravertebral block in patients undergoing open cholecystectomy and demonstrated that a significant reduction in circulatory and hormonal response. For eight patients with cardiopulmonary disease under open cholecystectomy, the epidural type catheter has been placed at the level of Th7. Twenty milliliters of 2% ropivacaine was injected by catheter. Surgery has lasted between 45 and 100 min. Only for three patients during retraction of the hepatic capsule, intra-operative remifentanyl infusion was needed. Except that, nausea-vomiting, headache, restlessness have not occurred. Additional bolus injection of propofol was needed due to our patients’ discomfort during the hepatic retraction. Except this short episode of the intra-operative period, additional anesthetic and analgesic requirements, nausea and vomiting and restlessness were not observed. Paracetamol 1 g was administered intravenously for two patients in the post-operative period. Opioids were not required.
Naja et al.[6] have been reported that there were no difference between post-operative nausea and vomiting, time to first micturition, defecation and oral feeding in their prospective study comparing TPVB applications with neurostimulator before and after the laparoscopic cholecystectomy. It has been understood that pre-operative TPVB has created a difference understood as preemptive when the data of this study about post-operative analgesic consumption has been examined. It has been reported that in the post-operative rest, during motion and coughing; VAS scores was below two, only 1 patient need pre-operative pethidine in the first 6 h.
In many studies have been reported that with paravertebral block provides effective post-operative analgesia which can take up to 38 h.[2,7] Especially for breast surgery, there are some clinics have reported that they use paravertebral block instead of general anesthesia as an unique anesthetic technique routinely.[2]
In the first patient, bilateral sensory block and hemodynamic responses have suggested that the spread of local anesthetics epidural space. The most important problem of single shot is inadequate block, prevertebral and epidural spread as a result of the possibility of sagittal spread of the local anesthetic.[8] Some authors may rule out this problem with multilevel injection. Concerning to the complete or partial loss of the sense of the adjacent (consecutive) dermatomes with single paravertebral injection, the vertical radiographic spread of local anesthetic injection can be displayed with the help of radiopaque substance.[8,9] Some patients still suffer from significant pain due to unidentified or anticipated spread of paravertebral injections administered during the pre-operative period.[6]
The limitation of this study is few number cases. Randomized controlled trials are needed for more precisely judgment. As a result, we suggest that paravertebral block may be carefully performed anesthesia in the patients with high risk of anesthesia who will be undergone open cholecystectomy albeit it is a rare complication and high success rate.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Paleczny J, Zipser P, Pysz M. Paravertebral block for open cholecystectomy. Anestezjol Intens Ter. 2009;41:89–93. [PubMed] [Google Scholar]
- 2.Karmakar MK. Thoracic paravertebral block. Anesthesiology. 2001;95:771–80. doi: 10.1097/00000542-200109000-00033. [DOI] [PubMed] [Google Scholar]
- 3.Coveney E, Weltz CR, Greengrass R, Iglehart JD, Leight GS, Steele SM, et al. Use of paravertebral block anesthesia in the surgical management of breast cancer: Experience in 156 cases. Ann Surg. 1998;227:496–501. doi: 10.1097/00000658-199804000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Eid HE. Paravertebral block: An overview. Curr Anaesth Crit Care. 2009;20:65–70. [Google Scholar]
- 5.Giesecke K, Hamberger B, Järnberg PO, Klingstedt C. Paravertebral block during cholecystectomy: Effects on circulatory and hormonal responses. Br J Anaesth. 1988;61:652–6. doi: 10.1093/bja/61.6.652. [DOI] [PubMed] [Google Scholar]
- 6.Naja MZ, Ziade MF, Lönnqvist PA. General anaesthesia combined with bilateral paravertebral blockade (T5-6) versus general anaesthesia for laparoscopic cholecystectomy: A prospective, randomized clinical trial. Eur J Anaesthesiol. 2004;21:489–95. doi: 10.1017/s026502150400612x. [DOI] [PubMed] [Google Scholar]
- 7.Batra RK, Krishnan K, Agarwal A. Paravertebral block. J Anaesthesiol Clin Pharmacol. 2011;27:5–11. [PMC free article] [PubMed] [Google Scholar]
- 8.Naja MZ, Ziade MF, El Rajab M, El Tayara K, Lönnqvist PA. Varying anatomical injection points within the thoracic paravertebral space: Effect on spread of solution and nerve blockade. Anaesthesia. 2004;59:459–63. doi: 10.1111/j.1365-2044.2004.03705.x. [DOI] [PubMed] [Google Scholar]
- 9.Naja ZM, El-Rajab M, Al-Tannir MA, Ziade FM, Tayara K, Younes F, et al. Thoracic paravertebral block: Influence of the number of injections. Reg Anesth Pain Med. 2006;31:196–201. doi: 10.1016/j.rapm.2005.12.004. [DOI] [PubMed] [Google Scholar]