

Abstract
Background:
Arterialized venous flaps (AVFs) have been used for reconstruction of soft tissue defects throughout the body. Several different revascularization models have been performed, but venous drainage through the arterial system has not been studied. In our total retrograde reverse blood flow (TRRBF) perfusion model, the arterial blood flow enters through the venous system and venous drainage exits through the arterial system.
Methods:
We developed a novel experimental model in rabbit ears to evaluate the capacity of TRRBF perfusion pattern to allow AVF viability. The ears were assigned to 3 groups: group 1, total devascularization without revascularization (n = 3); group 2, TRRBF (n = 12); and group 3, conventional AVF (n = 12). The ears were observed during a 30-day follow-up period, and clinical serial assessment of edema, cyanosis, and necrosis was performed. Tissue oxygenation was determined at the beginning and end of the follow-up. Histological analysis was performed.
Results:
Necrosis was found in 3/3 (100%) ears in group 1, 3/12 (25%) in group 2, and 0/12 (0%) in group 3 (95% CI, 0.505–0.994; P = 0.0001). In group 2, edema was higher (5/12, 41.66%) than in group 3 (0/12, 0%) (95% CI, 0.0135–0.65; P = 0.041). Cyanosis and venous congestion was of greater intensity and duration in group 2 than in group 3 (10.33 ± 4.51 vs 4.5 ± 2.06 d).
Conclusions:
Although evolution is torpid and prolonged in ears with TRRBF, 9/12 (75%) survived, suggesting that TRRBF can be used as a rescue method.
In an arterialized venous flap (AVF), arterial blood flow enters through an afferent vein and venous blood flow exits through an efferent vein.1–3 This type of revascularization was originally introduced in the late eighties. Although it is now infrequently studied, it remains in use. Clinical use of these flaps has been limited because of the high occurrence of partial or total flap necrosis and a slow healing process. Several experimental studies and clinical applications have been performed to evaluate whether different surgical procedures could enhance flap perfusion and flap survival.2,4–15 These experimental procedures include increasing angiogenesis by flap preexpansion,4,7,8 prearterialization technique,4,9,10 and surgical and pharmacological flap delay procedures.2,4,11,16–20 These procedures have been used successfully to increase flap blood flow and tissue oxygenation.
In 2010, Yan et al21 reported guidelines for improving flap survival, which included arterialization through a small afferent vein, increasing venous drainage through multiple efferent veins,22 designing the flap over a venous network, and restraining arteriovenous shunting.23,24 Using these guidelines can increase total flap size and survival area of AVFs.
Three types of AVFs based on perfusion patterns in relation to venous valve orientation were also reported15: anterograde perfusion pattern, retrograde perfusion pattern, and mixed perfusion pattern. The majority of reported AVFs have anterograde perfusion patterns.1–3,9,11–13,15,17,20,22,25–27 Although the majority of evidence suggests that perfusion pattern has no influence on flap survival, there are some reports that retrograde perfusion patterns can enhance flap perfusion. There are also other classification systems, including those based on the number, location, and configuration of flap vessels. These factors may influence flap survival.15,21,23
Yoshimura et al28 were the first to use AVFs clinically, and AVFs have since been used for the reconstruction of soft tissue defects of the upper extremities, face, cranium, and neck.2–4,13,25,27,29–33 Composite flaps have been used for reconstruction of nerves, vessels, and tendons,13,21,34–37 while AVFs have also been used in reconstruction of small hand defects. Small-sized AVFs (1 × 1 cm up to 3 × 10 cm) have a 95–100% survival rate. AVFs with larger surfaces often suffer partial necrosis and have a 40% failure rate. AVFs in all reported series, regardless of flap size, are at risk of sustained postoperative congestion (100%),4,22,29,38 partial flap necrosis (20%), and total flap necrosis (12%).21
There are multiple experimental and clinical models of AVF revascularization, although a total retrograde reverse blood flow (TRRBF) perfusion pattern has never been described. In TRRBF, the arterial blood flow enters the flap through the venous system and the venous drainage exits the flap exclusively through the arterial system. Thus, the aim of this novel experimental study was to evaluate the capacity of a TRRBF perfusion pattern to enhance AVF viability. The chosen experimental model was the rabbit ear because it contains a well-defined vascular pedicle and a valved venous system.2,10,16,17,39,40
MATERIALS AND METHODS
This is a pilot study designed to evaluate whether this form of revascularization may maintain viable tissues. For this reason, 15 healthy female and male New Zealand rabbits, weighing 3–3.50 kg, were used. Twenty-seven ears of these rabbits were used in the experimental surgical model. Anesthesia was induced with an intraperitoneal injection of a mixture of ketamine (80 mg/kg) and epontol (20 mg/kg) with supplemental doses administered as necessary. Preoperative antibiotic prophylaxis was administered with a single intraperitoneal injection of amoxicillin (100 mg/kg). The ears were assigned to 3 groups: group 1, total surgical devascularization (n = 3); group 2, TRRBF using the right ears (n = 12); and group 3, AVF using the left ears (n = 12). The surgery was performed under sterile conditions. Surgical dissection was performed under operating microscope magnification (6×). End-to-end anastomoses using interrupted sutures with 10-0 and 11-0 nylon were performed under microscope magnification (16×). Immediate postoperative lidocaine infiltration was administered in the base of the ears for anesthesia. The same experienced microsurgical surgeon (M.I.) performed all of the surgical procedures. This protocol was approved by the Research in Animals Committee and the Investigation Department of the National Institute of Medical Science and Nutrition “Salvador Zubirán” (CEX-003-94-94-1).
Surgical Technique in Group 1
Initially, a circular incision was made at the base of the ear. Skin, cellular subcutaneous tissue, muscles, and perichondrium were cut. All vascular elements were ligated and cut. The purpose of this incision was to achieve a complete surgical devascularization of the ears. Revascularization procedures were not performed. Wounds were closed using 3-0 silk sutures (Fig. 1).
Fig. 1.
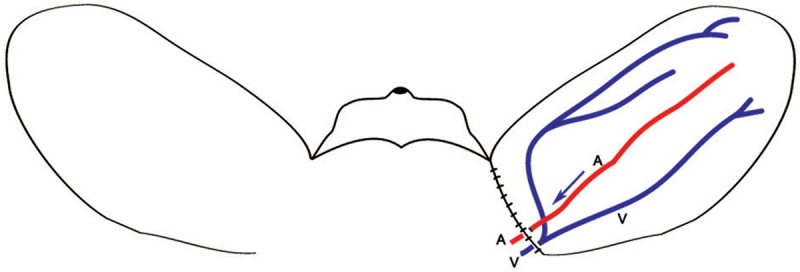
Circular incision for total devascularization of the ear. The artery and the vein within the pedicle are ligated and cut. Revascularization was not performed. A, artery; V, vein.
Surgical Technique in Group 2
A 2-cm incision was made over the vascular pedicle in the dorsal aspect of the right ear. The artery and the main vein were identified, dissected, and isolated within 1.5 cm. Both vessels were cut with scissors. Subsequently, a circular incision was made throughout the base of the ear, as in group 1. Revascularization of the ear was performed as follows: the proximal recipient artery was anastomosed to the central vein of the ear and the proximal recipient vein was anastomosed to the artery of the ear. The patency of both vascular anastomoses was confirmed visually for 20 minutes. Finally, the wound was closed with simple 3-0 silk sutures. This constituted an AVF with TRRBF (Fig. 2, right ear).
Fig. 2.
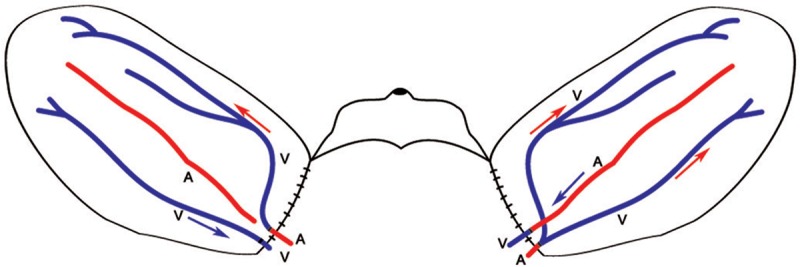
Right ear revascularization with total retrograde reverse blood flow. Left ear revascularization as an arterialized venous flap with retrograde perfusion pattern. Red arrows show the direction of blood flow. Blue arrows show the direction of venous drainage. A, artery; V, vein.
Surgical Technique in Group 3
Identification of vascular elements and surgical devascularization were performed in the left ears as in group 2. Revascularization of the left ear was performed as follows: the proximal recipient artery was anastomosed to the central vein of the ear and the proximal recipient vein was anastomosed to other vein of the ear. The patency of both vascular anastomoses was confirmed visually for 20 minutes. Finally, the wound was closed with simple 3-0 silk sutures. This constituted an AVF with retrograde perfusion pattern (Fig. 2, left ear).
Follow-up and Evaluation
The rabbits were maintained under daily observation for 30 days. The animals were housed in individual boxes with temperature control (20–24°C). Ad libitum access to water and food was provided. Postoperative treatment included intraperitoneal administration of amoxicillin (100 mg/kg) every 24 hours for 3 days and 5 drops of metamizole in the rabbit’s drinking water every 12 hours for analgesia.
Oxygen saturation (PaO2) was determined in all ears with a transcutaneous oximeter placed at the most distal region of the ear. Measurements were taken immediately after anesthesia (day 0) and just before euthanasia (day 30). Both measurements were recorded without supplementary oxygen administration. The purpose of these evaluations was to assess for differences in PaO2 between the different forms of revascularization.
Viability of the ears was evaluated clinically every 24 hours until the end of the study. Tissue viability was determined by the color of the ear. A color scale was established and printed (pink = normal, blue and violet = mild cyanosis, purple = intense cyanosis, and black = necrosis). Observers at each assessment used this printed scale. There were only 2 observers. These changes were registered as: normal = 0, mild cyanosis = 1, severe cyanosis = 2, and necrosis = 3. The duration (in days) of the coloration changes was recorded. The necrotic area was expressed as a percentage of the total ear surface. A graduated pattern was used to assess the necrotic area in the ear. The necrotic tissue was defined when the tissue perfusion was not detected, with loss of firmness and warmth, and when the color skin changed to black. Failure was defined as necrosis of more than 50% of the ear surface. Success with partial necrosis was defined as necrosis of less than 50% of the total ear surface.
Edema of the ears was also recorded. The edema was evaluated using a clinical scale: grade 0 = without edema, grade 1 = bulking edema without the loss of the shape and creases, and grade 2 = bulking and deforming edema with loss of creases. Duration of edema was recorded. The clinical changes of the ears were documented by clinical photography.
At the end of the follow-up, all rabbits were euthanized with an intraperitoneal lethal overdose of sodium pentobarbital. Biopsies of the arterialized vein of the main pedicle were taken. To evaluate tissue biopsy away from the main vessels, full thickness biopsies, including skin, subcutaneous cellular tissue, cartilage, and vascular network, were taken from the middle of the ear in the area located between the central pedicle and the lateral edge of the ear. Ears that showed necrosis were not sent to pathology.
Sections were stained with hematoxylin and eosin and examined. Endothelial hyperplasia was evaluated and classified: grade 1 = vascular occlusion less than or equal to 25%, grade 2 = vascular occlusion between 25% and 50%, grade 3 = vascular occlusion between 50% and 75%, and grade 4 = vascular occlusion greater than 75%.
Statistics
The results were expressed as percentages, means, and standard deviations. Mann–Whitney and Friedman–Kaplan tests were used. In the comparison of proportions we used χ2 tests (with adjustments to several if necessary). Differences were considered significant at P < 0.005. Confidence intervals (CIs) were constructed at 95%. Statistical analysis was performed using Minitab statistical software version 13.1.
RESULTS
The necrosis rates were 3/3 (100%) for group 1, 3/12 (25%) for group 2, and 0/12 (0%) for group 3 (95% CI, 0.505–0.994; P = 0.0001). Necrosis was significantly different between group 2 and group 3 (95% CI, 0.005–0.494; P = 0.046). This statistical difference was small because of the sample size. The χ2 test was used.
O2 Saturation
The difference between initial and final PaO2 measurements was minimal for group 3 and greatest for group 1. The drop of PaO2 measured in group 2 was between groups 1 and 3. There was a significant overall difference in the final PaO2 measurements among groups 1–3 (0, 55.6 ± 41, and 91.3 ± 35, respectively) (95% CI, 2.06–81.3; P = 0.0001). The initial mean PaO2 in group 2 was 94% (90–97%) and the final measure was 84% (73–90%). The initial mean PaO2 in group 3 was 95% (90–99%) and the final measure was 91% (86–99%). For each one of the surviving ears of group 2 and group 3, the difference (delta) between initial PaO2 and final PaO2 was calculated. The mean value of the delta was significantly higher in group 2 than in group 3 (10.44% ± 5.2% vs 3.41% ± 1.78%; 95% CI, 2.99–9.99; P = 0.002).
Viability
In group 1, 3/3 (100%) ears reached the worst possible color grade (necrosis), whereas only 3/12 (25%) of group 2 ears and 0/12 (0%) of group 3 ears reached this grade. There was a significant overall difference between these groups (95% CI, 0.505–0.994; P = 0.00001). Group 1 ears and group 2 ears reached their worst color grade on different days, although this difference was not statistically significant (2.66 ± 0.57 d vs 10.33 ± 4.51 d; 95% CI, –18.93 to 3.63; P = 0.10). This statistical difference was low because of the sample size. In group 2, 3 ears developed partial necrosis (10–20%) of up to 20% of the ear’s total surface. This necrosis was exclusively localized to the proximal region where the vein was arterialized. A 15% necrosis was also seen in the same place in 1 ear from group 3. In group 2, grade 1 and grade 2 ears recovered normal coloration (grade 0) at 10.6 ± 6.09 days. In group 3, grade 1 and grade 2 ears recovered normal coloration (grade 0) at 4.5 ± 2.06 days. Grade 3 coloration (necrosis) never occurred in group 3.
Edema
Edema was not recorded in group 1. In group 2, grade 2 edema occurred in 5/12 (41.66%) ears compared with 0/12 (0%) in group 3 (95% CI, 0.0135–0.65; P = 0.041). In group 2, 2/5 (40%) ears that had grade 2 edema experienced necrosis, while the other three survived (95% CI, −0.40 to 0.80; P = 0.05). Grade 2 edema developed in the early recovery days and evolved with necrosis of the ear. The necrotic ears reached maximum edema at 1.33 ± 0.23 days and the surviving ears at 6 ± 1 days (95% CI, −0.40 to 0.80; P = 0.148).
Histology
The histological results of the surviving ears are shown in Tables 1 and 2. There was no significant difference between the groups. In group 2, the reduction in PaO2 allowed ear survival, but was accompanied by 5 cases of skin atrophy, 2 cases of chronic inflammation, and 2 ears with normal skin characteristics (Table 1). Subendothelial hyperplasia (SH) of the arterialized vein was found in both groups. SH was mostly grade 1. Grade 3 SH was identified in only 1 ear in group 2 compared with 2/12 ears in group 3 (Table 2).
Table 1.
Cutaneous Histology of Viable Ears (Group 1 vs Group 2)

Table 2.
Subendothelial Hyperplasia Grade

DISCUSSION
In all clinical and experimental AVFs, the entry of arterial blood flow occurs through an afferent vein and the venous drainage occurs through one or more efferent veins. AVFs have demonstrated their clinical applicability, therefore expanding the possibilities of transfer and replantation of artery-free tissues.41–44 The physiologic perfusion and survival mechanisms of AVFs remain controversial. Currently, 3 main theories have been postulated as to the physiology of the venous flap. These include “A-V shunting,” “reverse flow,” and “capillary bypass.” Neovascularization and perivenous areolar tissues were also hypothesized to play a role in the survival of venous flaps.4,45
To evaluate the capacity of the TRRBF to allow AVF survival, we developed a novel experimental model in rabbit ears. The experimental model in rabbit ears is ideal, as shown in previous studies.46 Revascularization was performed in previously devascularized ears, mimicking an AVF with a retrograde perfusion pattern and thereby forcing blood flow through the entire venous system of the ear. In this manner, the efferent blood flow exits the flap through the only available efferent vessel, which is the artery of the flap that had been anastomosed to the recipient vein.
Total devascularization of the ear without revascularization procedures caused a 100% necrosis rate (group 1). The 3 ears in the study all showed very similar clinical evolution and complete necrosis at 2.66 ± 0.57 days, suggesting that this would be typical even with a larger sample size. These data suggest that arterial afferent blood flow is required for flap survival. The surgical revascularization performed in AVF ears (group 3) exhibited a significantly lower rate of necrosis than total devascularization without revascularization (group 1) (P = 0.0001).
To our knowledge, AVF with TRRBF has not been previously reported. The position of the venous valves impedes the advancement of retrograde blood flow in the venous system, and thus hinders the perfusion and viability in the distal tissue. We developed our model in this way to evaluate its feasibility. Although a higher necrosis rate was observed in group 2 ears than in group 1 and 3 ears, this rate was within the ranges previously reported with traditional AVFs (0–42.3%).21 Our 100% success rate with AVFs with a retrograde perfusion pattern is identical to the success rates reported by Koch et al6 and Woo and Seul.8
The clinical course of TRRBF ears (group 2) was characterized by edema and cyanosis occurring over a 10-day period, compared with the 4.5-day period observed in the AVF ears (group 3). The edematous and cyanotic period observed in group 3 ears is within the 3- to 6-day period reported by other authors.8 Higher intensity edema and cyanosis was observed in group 2 ears than in group 1 and 3 ears, which is attributable to the high resistance to flow within the artery. These signs were more evident in the vicinity of the arterialized efferent veins, causing partial necrosis proximal to the wound site in 3 ears of the group 2 and 1 ear in group 3. After 2 weeks, necrotic areas healed by secondary intention. The percentage of partial necrosis was similar to the results previously reported.4,44 There was no significant difference in the clinical courses of group 2 and group 3.
The TRRBF ears (group 2) showed a significant reduction in PaO2 at the end of the study when compared with AVFs with retrograde perfusion patterns (group 3). The results observed in group 2 are consistent with previous studies of AVFs examining fibrosis and atrophy as primary endpoints.5,6,15 It was also suggested that the presence of a good recipient bed where revascularization will take place after 3 days might prevent the appearance of alterations like fibrosis and atrophy. In our experimental model, the survival of the ears depended exclusively on the revascularization. However, there was no recipient bed in our model.
Our experimental model did not fulfill the previously reported requirements for improving AVFs survival.4 The arterialization of the flap was performed in the main vein of the ear instead of using a small diameter vein. Additionally, there was only 1 efferent vessel with high resistance to flow. However, the survival rate at the end of the follow-up was 75% for TRRBF. Flap survival increased to 100% when we had endowed ears with an efferent vein with low resistance to flow (P = 0.046). For both groups, the survival rates were similar to those previously reported.4,21,22,29,38
If a total vascular occlusion develops, collateral circulation would already be formed and may allow flap survival. Evaluation of this concept requires long-term follow-up. AVFs with TRRBF have high probabilities of surviving, even though their clinical evolution is torpid and prolonged. In this study, 9/12 ears with TRRBF survived. We demonstrated that if we had not vascularized these ears, they would have been lost. Despite the fact that our sample number is small, we conclude that TRRBF could be used as a rescue method.
Conclusions
This is only a pilot study to evaluate whether this form of revascularization may maintain viable tissues. Our model requires more experimental work. Nevertheless, we consider that reconstructive microsurgeons should be familiarized with TRRBF to have them succeed and should also be familiar with their prolonged clinical evolution.
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Nakayama Y, Soeda S, Kasai Y. Flaps nourished by arterial inflow through the venous system: an experimental investigation. Plast Reconstr Surg. 1981;67:328–334. doi: 10.1097/00006534-198103000-00009. [DOI] [PubMed] [Google Scholar]
- 2.Tan MP, Lim AY, Zhu Q. A novel rabbit model for the evaluation of retrograde flow venous flaps. Microsurgery. 2009;29:226–231. doi: 10.1002/micr.20610. [DOI] [PubMed] [Google Scholar]
- 3.Fukui A, Inada Y, Maeda M, et al. Venous flap—its classification and clinical applications. Microsurgery. 1994;15:571–578. doi: 10.1002/micr.1920150810. [DOI] [PubMed] [Google Scholar]
- 4.Yan H, Brooks D, Jackson WD, et al. Improvement of prearterialized venous flap survival with delay procedure in rats. J Reconstr Microsurg. 2010;26:193–200. doi: 10.1055/s-0030-1247715. [DOI] [PubMed] [Google Scholar]
- 5.Moshammer HE, Schwarzl FX, Haas FM, et al. Retrograde arterialized venous flap: an experimental study. Microsurgery. 2003;23:130–134. doi: 10.1002/micr.10108. [DOI] [PubMed] [Google Scholar]
- 6.Koch H, Scharnagl E, Schwarzl FX, et al. Clinical application of the retrograde arterialized venous flap. Microsurgery. 2004;24:118–124. doi: 10.1002/micr.20011. [DOI] [PubMed] [Google Scholar]
- 7.Mutaf M, Tasaki Y, Fujii T. Expansion of venous flaps: an experimental study in rats. Br J Plast Surg. 1998;51:393–401. doi: 10.1054/bjps.1997.0151. [DOI] [PubMed] [Google Scholar]
- 8.Woo SH, Seul JH. Pre-expanded arterialised venous free flaps for burn contracture of the cervicofacial region. Br J Plast Surg. 2001;54:390–395. doi: 10.1054/bjps.2001.3597. [DOI] [PubMed] [Google Scholar]
- 9.Wungcharoen B, Pradidarcheep W, Santidhananon Y, et al. Pre-arterialisation of the arterialised venous flap: an experimental study in the rat. Br J Plast Surg. 2001;54:621–630. doi: 10.1054/bjps.2001.3675. [DOI] [PubMed] [Google Scholar]
- 10.Fukui A, Inada Y, Murata K, et al. A method for prevention of arterialized venous flap necrosis. J Reconstr Microsurg. 1998;14:67–74. doi: 10.1055/s-2007-1006904. [DOI] [PubMed] [Google Scholar]
- 11.Cho BC, Lee JH, Byun JS, et al. Clinical applications of the delayed arterialized venous flap. Ann Plast Surg. 1997;39:145–157. doi: 10.1097/00000637-199708000-00007. [DOI] [PubMed] [Google Scholar]
- 12.Nichter LS, Jazayeri MA. The physiologic basis for nonconventional vascular perfusion. Plast Reconstr Surg. 1995;95:406–412. doi: 10.1097/00006534-199502000-00026. [DOI] [PubMed] [Google Scholar]
- 13.Inoue G, Maeda N. Arterialized venous flap coverage for skin defects of the hand or foot. J Reconstr Microsurg. 1988;4:259–266. doi: 10.1055/s-2007-1006929. [DOI] [PubMed] [Google Scholar]
- 14.Baek SM, Weinberg H, Song Y, et al. Experimental studies in the survival of venous island flaps without arterial inflow. Plast Reconstr Surg. 1985;75:88–95. doi: 10.1097/00006534-198501000-00020. [DOI] [PubMed] [Google Scholar]
- 15.Woo SH, Kim KC, Lee GJ, et al. A retrospective analysis of 154 arterialized venous flaps for hand reconstruction: an 11-year experience. Plast Reconstr Surg. 2007;119:1823–1838. doi: 10.1097/01.prs.0000259094.68803.3d. [DOI] [PubMed] [Google Scholar]
- 16.Byun JS, Constantinescu MA, Lee WP, et al. Effects of delay procedures on vasculature and survival of arterialized venous flaps: an experimental study in rabbits. Plast Reconstr Surg. 1995;96:1650–1659. doi: 10.1097/00006534-199512000-00019. [DOI] [PubMed] [Google Scholar]
- 17.Cho BC, Lee MS, Lee JH, et al. The effects of surgical and chemical delay procedures on the survival of arterialized venous flaps in rabbits. Plast Reconstr Surg. 1998;102:1134–1143. doi: 10.1097/00006534-199809040-00033. [DOI] [PubMed] [Google Scholar]
- 18.Ueda K, Harada T, Nagasaka S, et al. An experimental study of delay of flow-through venous flaps. Br J Plast Surg. 1993;46:56–60. doi: 10.1016/0007-1226(93)90066-k. [DOI] [PubMed] [Google Scholar]
- 19.Başer NT, Silistreli OK, Sişman N, et al. Effects of surgical or chemical delaying procedures on the survival of proximal predicled venous island flaps: an experimental study in rats. Scand J Plast Reconstr Surg Hand Surg. 2005;39:197–203. doi: 10.1080/02844310510006349. [DOI] [PubMed] [Google Scholar]
- 20.Karacalar A, Ozcan M. Free arterialized venous flap for the reconstruction of defects of the hand: new modifications. J Reconstr Microsurg. 1994;10:243–248. doi: 10.1055/s-2007-1006592. [DOI] [PubMed] [Google Scholar]
- 21.Yan H, Brooks D, Ladner R, et al. Arterialized venous flaps: a review of the literature. Microsurgery. 2010;30:472–478. doi: 10.1002/micr.20769. [DOI] [PubMed] [Google Scholar]
- 22.Inada Y, Fukui A, Tamai S, et al. The arterialised venous flap: experimental studies and a clinical case. Br J Plast Surg. 1993;46:61–67. doi: 10.1016/0007-1226(93)90067-l. [DOI] [PubMed] [Google Scholar]
- 23.Lin YT, Henry SL, Lin CH, et al. The shunt-restricted arterialized venous flap for hand/digit reconstruction: enhanced perfusion, decreased congestion, and improved reliability. J Trauma. 2010;69:399–404. doi: 10.1097/TA.0b013e3181bee6ad. [DOI] [PubMed] [Google Scholar]
- 24.Suzuki Y, Suzuki K, Ishikawa K. Direct monitoring of the microcirculation in experimental venous flaps with afferent arteriovenous fistulas. Br J Plast Surg. 1994;47:554–559. doi: 10.1016/0007-1226(94)90139-2. [DOI] [PubMed] [Google Scholar]
- 25.Suzuki Y, Isshiki N, Ishikawa K, et al. Viability and quantitative dermofluorometry of experimental arterialised and non-arterialised venous flaps. Br J Plast Surg. 1993;46:273–278. doi: 10.1016/0007-1226(93)90001-r. [DOI] [PubMed] [Google Scholar]
- 26.Chen HC, Tang YB, Noordhoff MS. Four types of venous flaps for wound coverage: a clinical appraisal. J Trauma. 1991;31:1286–1293. doi: 10.1097/00005373-199109000-00014. [DOI] [PubMed] [Google Scholar]
- 27.Wolff KD, Telzrow T, Rudolph KH, et al. Isotope perfusion and infrared thermography of arterialised, venous flow-through and pedicled venous flaps. Br J Plast Surg. 1995;48:61–70. doi: 10.1016/0007-1226(95)90098-5. [DOI] [PubMed] [Google Scholar]
- 28.Yoshimura M, Shimada T, Imura S, et al. The venous skin graft method for repairing skin defects of the fingers. Plast Reconstr Surg. 1987;79:243–250. doi: 10.1097/00006534-198702000-00016. [DOI] [PubMed] [Google Scholar]
- 29.Tsai TM, Matiko JD, Breidenbach W, et al. Venous flaps in digital revascularization and replantation. J Reconstr Microsurg. 1987;3:113–119. doi: 10.1055/s-2007-1006973. [DOI] [PubMed] [Google Scholar]
- 30.Inoue G, Maeda N, Suzuki K. Resurfacing of skin defects of the hand using the arterialised venous flap. Br J Plast Surg. 1990;43:135–139. doi: 10.1016/0007-1226(90)90150-x. [DOI] [PubMed] [Google Scholar]
- 31.Yilmaz M, Menderes A, Karaca C, et al. Free arterialized venous forearm flap. Ann Plast Surg. 1995;34:88–91. doi: 10.1097/00000637-199501000-00019. [DOI] [PubMed] [Google Scholar]
- 32.Galumbeck MA, Freeman BG. Arterialized venous flaps for reconstructing soft-tissue defects of the extremities. Plast Reconstr Surg. 1994;94:997–1002. doi: 10.1097/00006534-199412000-00013. [DOI] [PubMed] [Google Scholar]
- 33.Brooks D, Buntic R, Buncke HJ. Use of a venous flap from an amputated part for salvage of an upper extremity injury. Ann Plast Surg. 2002;48:189–192. doi: 10.1097/00000637-200202000-00013. [DOI] [PubMed] [Google Scholar]
- 34.Inoue G, Tamura Y. One-stage repair of both skin and tendon digital defects using the arterialized venous flap with palmaris longus tendon. J Reconstr Microsurg. 1991;7:339–343. doi: 10.1055/s-2007-1006794. [DOI] [PubMed] [Google Scholar]
- 35.Chen CL, Chiu HY, Lee JW, et al. Arterialized tendocutaneous venous flap for dorsal finger reconstruction. Microsurgery. 1994;15:886–890. doi: 10.1002/micr.1920151212. [DOI] [PubMed] [Google Scholar]
- 36.Lin CH, Wei FC, Lin YT, et al. Composite palmaris longus-venous flap for simultaneous reconstruction of extensor tendon and dorsal surface defects of the hand—long-term functional result. J Trauma. 2004;56:1118–1122. doi: 10.1097/01.ta.0000112330.30078.dc. [DOI] [PubMed] [Google Scholar]
- 37.Cho BC, Byun JS, Baik BS. Dorsalis pedis tendocutaneous delayed arterialized venous flap in hand reconstruction. Plast Reconstr Surg. 1999;104:2138–2144. doi: 10.1097/00006534-199912000-00030. [DOI] [PubMed] [Google Scholar]
- 38.Honda T, Nomura S, Yamauchi S, et al. The possible applications of a composite skin and subcutaneous vein graft in the replantation of amputated digits. Br J Plast Surg. 1984;37:607–612. doi: 10.1016/0007-1226(84)90158-9. [DOI] [PubMed] [Google Scholar]
- 39.Boustred AM. The rabbit dorsal flank flap. J Reconstr Microsurg. 1997;13:331–335. doi: 10.1055/s-2007-1006412. [DOI] [PubMed] [Google Scholar]
- 40.Yuen QM, Leung PC. Some factors affecting the survival of venous flaps: an experimental study. Microsurgery. 1991;12:60–64. doi: 10.1002/micr.1920120112. [DOI] [PubMed] [Google Scholar]
- 41.Morris SF, MacGill KA, Taylor GI. Scalp replantation by arterialised venous network flow-through. Br J Plast Surg. 1992;45:187–192. doi: 10.1016/0007-1226(92)90074-8. [DOI] [PubMed] [Google Scholar]
- 42.Sakai S. Arterialised venous groin flap: case report. Br J Plast Surg. 1996;49:90–92. doi: 10.1016/s0007-1226(96)90079-x. [DOI] [PubMed] [Google Scholar]
- 43.Fukui A, Maeda M, Inada Y, et al. Arteriovenous shunt in digit replantation. J Hand Surg Am. 1990;15:160–165. doi: 10.1016/s0363-5023(09)91125-x. [DOI] [PubMed] [Google Scholar]
- 44.Woo SH, Jeong JH, Seul JH. Resurfacing relatively large skin defects of the hand using arterialized venous flaps. J Hand Surg Br. 1996;21:222–229. doi: 10.1016/s0266-7681(96)80103-3. [DOI] [PubMed] [Google Scholar]
- 45.Pittet B, Chang P, Cederna P, et al. The role of neovascularization in the survival of an arterialized venous flap. Plast Reconstr Surg. 1996;97:621–629. doi: 10.1097/00006534-199603000-00021. [DOI] [PubMed] [Google Scholar]
- 46.Lin CH, Wei FC, Mardini S, et al. Microcirculation study of rabbit ear arterial and venous flow-through flaps using a window chamber model. J Trauma. 2004;56:894–900. doi: 10.1097/01.ta.0000076055.67256.b0. [DOI] [PubMed] [Google Scholar]