

Abstract
Background:
Curved lower legs cause psychological stress for women. In evaluating the shape, if thickness is the main contributing factor of leg aesthetic, then lipoplasty or calf reducing procedures will be the option. If the legs are slender and have no muscle hypertrophy but still have some indentation or bulges on both sides and lack an aesthetic shape what will be the options? The answer to the question is discussed in detail in this article.
Methods:
Twenty-two patients, operated over a period of 5 years from 2007 to 2012, were included in the study. A novel technique has been introduced. This method requires release of fascia covering muscles of the inner leg bulge via endoscopic approach and simultaneous calf augmentation with calf implant, liposuction, and structural fat grafting to optimize the results.
Results:
Patients were followed on a regular basis with a mean follow-up of 31 months. The procedure was well tolerated with minimal discomfort during the postoperative period. Increase in diameter of proximal and distal lower legs was measured at least 6 months after surgery. Mean diameter change of proximal lower legs was 2.16 cm and 1.77 cm in distal lower legs.
Conclusions:
A novel endoscopic approach for lower leg contouring is discussed. Endoscopic fasciotomy technique with calf implant and structural fat grafting for improved lower leg aesthetics is a simple, effective, reliable, and predictable technique for calf contouring.
Unaesthetic lower legs cause psychological stress for women. Fashions change seasonally and clothes that expose leg contours have a definitive impact on women’s wishes to be able to comfortably wear these fashions by obtaining surgical improvement if possible.
The tibia, fibula, and muscles around these bones and the adipose tissues that cover them circumferentially shape the lower leg. Regarding the adipose tissue component, excess or lack of fat in the lower leg along with muscle excess or deficiency plays a dominant role on the overall shape of this area. It is sometimes the fascia that covers the gastrocnemius and soleus muscle that restricts them from adequately filling the leg convex contour. We recognize that there is a bony component contributing to this shape as well, but that element is beyond the scope of this article.
Treatment options for lower leg contour deformities may vary. Calf implants are one of the options. The first calf augmentation with implants by Carlsen1 in 1979 was carved from silastic foam. Contouring of the lower leg has progressed greatly since the early days of liposuction.2–6 Sometimes a circumferential liposuction of knees, calves, and ankles seems to be the best option to slenderize the legs where they are unaesthetically thick.7 If the main problem is not fat but rather hypertrophied gastrocnemius muscle, a calf reduction procedure may be the appropriate surgical approach.8 And for some of the others, contouring with a calf implant is the most direct and simple technique for leg improvement.9
In this article, a novel technique has been introduced for the lower leg contour deformities. This method requires release of fascia covering muscles of the inner leg bulge via endoscopic approach and simultaneous calf augmentation with calf implant, liposuction, and structural fat grafting to optimize the results.
PATIENTS AND METHODS
Twenty-two patients, operated over a period of 5 years from 2007 to 2012, were included in the study. Patients were seen for preoperative consultation before their surgery. All patients were informed of the nature of the surgery and the risks and benefits and agreed to participate in the study.
Patient Selection
Each patient was evaluated on the basis of certain criteria. Patients who wanted a calf contouring with medial crural contour deficiency and/or anterior crural contour deficiency and/or lateral crural contour excess were included in the study. Size of the implants, severity of contour deformity, and quality of the tissue were evaluated. Preoperative evaluation was completed with final calf contour assessment; ancillary options for liposuction and fat grafting were also analyzed and discussed with the patients (Figs. 1A, B).
Fig. 1.
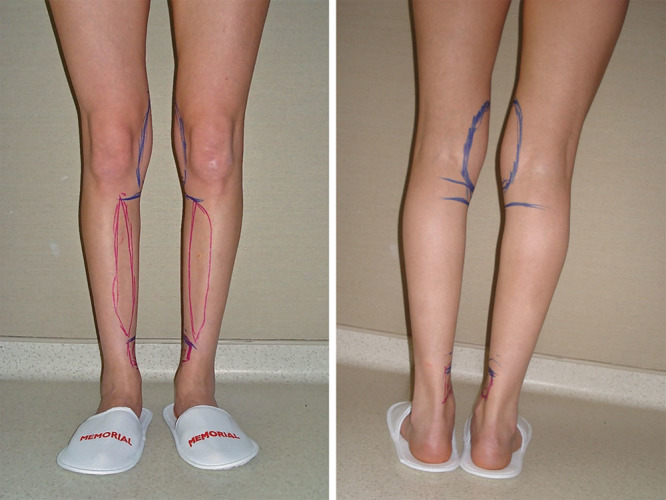
A and B, Preoperative marking. Area for suction-assisted lipectomy (blue circles), structural fat grafting (red markings), and fascial release and implant placement (blue horizontal lines show the lower and upper end of implant to be inserted) were marked.
Preoperative Marking
The key mandatory part of the marking was preoperative judgment about which additions and/or subtractions would result in optimal improved lower leg contour. Keeping these principles in mind, the marking and planning started with the patient in standing position.
The fat pad of the inner knee and outer lower leg was marked for suction-assisted lipectomy. The lack of slight convexity on the inner part of proximal lower leg was outlined as well. The transition line of the indentation of the inner lower leg was also marked.
The most medial border of the popliteal crease incision was also marked while the patient was still in the standing position. Marking for the implant pocket was based on the certain anatomic references. The superior marking was placed just at the medial border of the proximal lower leg where a maximum of convexity was desired. The marking for the inferior border was placed at the lowest medial border cephalic (but not posterior) to the medial malleolus where a final lower fullness should be achieved (Figs. 1A, B).
The next critical marking was where to locate the implant. At this point, the reflection of shape and size of the implant was discussed with the patient thoroughly. Shapes and sizes of the implants were taken into consideration while the patient was in the standing position to help select the shape and size to best fit the patient’s expectations. As a convention, the implant was intended to augment the upper 80% of the medial lower leg surface anatomy.
Surgical Technique
A standard endoscopic setup, including video camera and monitor, light source, and other endoscopic instruments, was utilized in the operating room. A 10-mm diameter, 20-cm long, 30-degree rigid endoscope and a built-in endoscopic retractor (Snowden-Pencer, Tucker, GA) were used for each procedure.
The operation was performed under general anesthesia with the patient in prone position. A transverse incision measuring 4 cm in the popliteal crease was made and the plane above the crural fascia was dissected bluntly down to the medial gastrocnemius muscle, which had been carefully marked preoperatively with the patient in a standing position and raised heel position for identification of precise areas of planned fascial release to allow the muscle to enhance the deficient medial contour. Particular care was undertaken during manipulations in this area to avoid injury to the lessor saphenous vein that lies in the posterior lateral part of this region and to the medial cutaneous nerve of the calf. The subfascial plane was also dissected under endoscopic visual control and the fascia in this area was released with scissors under direct endoscopic vision up to the mid calf area (Fig. 2). After this point, a curved hook blade was used to serially score the fascia in a longitudinal direction and so as to render it lax. This maneuver made the tight compressive fascia much looser. This fascia was seen to be very thick over the medial compartment, and once this had been serially scored, the muscle was free to gently expand and compliment the curves in the medial calf that were deficient (Fig. 3). The identical procedure was carried out on the opposite side. Following this, inspection revealed a very nice symmetry with respect to release of the fascia in the predetermined region.
Fig. 2.

A transverse incision measuring 4 cm in the popliteal crease was made and the plane above the crural fascia was dissected bluntly down to the medial gastrocnemius muscle. The subfascial plane is also dissected under endoscopic visual control and the fascia in this area was released via scissors under direct endoscopic vision till mid calf area.
Fig. 3.
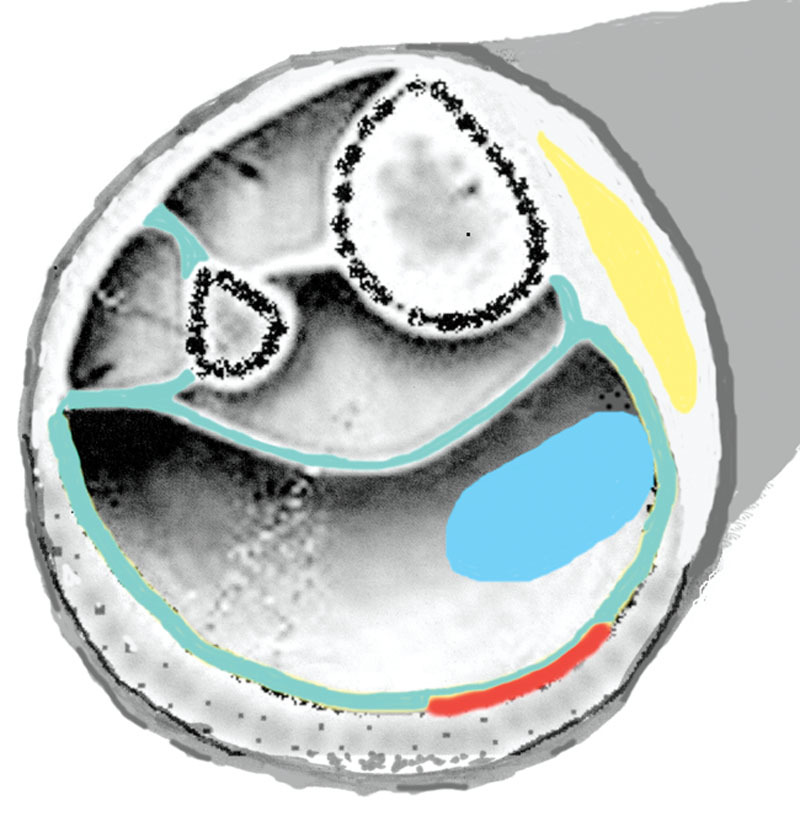
Schematic representation of fascial compartments of leg at mid-leg level. Turquoise lines show fascial network of the lower leg where the most posterior line shows the superficial fascia that covers soleus and gastrocnemius muscles. Red line shows where approximately fasciotomy is done. The location of structural fat grafting is shown in yellow and implant in blue. Please note that the implant was located in somewhere middle of the superficial compartment to simulate the pocket between soleus and gastrocnemius muscles.
The next step was to create a submuscular pocket. After fascial release, the tendon of the semitendinosus muscle was seen and dissection proceeded medial to the tendon. By blunt dissection, the medial edge of the medial head of the gastrocnemius was exposed. An entry plane was created between the medial gastrocnemius and soleus. The dissection was further continued using a blunt dissector until the cavity was capacious enough to fit the selected implant. Because the dissection plane was relatively avascular, the dissection time was reduced and complications were avoided. After the dissection was completed, a sizer was placed to confirm optimal implant selection. The implants chosen were silicone gel-filled symmetrical and asymmetrical calf implant models sized from 120 to 220 cm3 (Euro Silicone, France).
After temporary implant insertion, the area for liposuction and fat grafting was meticulously addressed. After that, the implant was explanted to prevent further surgical procedures from causing harm to the implant. Suction-assisted lipectomy with 20 cm3 syringe of the premarked areas was performed, yielding pure fat while preserving the fat tissue for grafting.
Harvested fat tissues were centrifuged at 3000 rpm for 3 minutes. Centrifuged fat grafts were applied to the marked area. The structural fat grafting technique of Coleman10 was used. After liposuction and structural fat grafting, the submuscular pocket for implant insertion was checked for bleeding. The placement of the implant in the pocket was made based on the preoperative markings.
Finally, the incisions were closed. First the fascia was closed by 3/0 polydioxanone. This was followed by deep dermal reapproximation using 3/0 monocryl. Final skin closure was completed using 4/0 nylon.
Hypafix was applied for contour shaping followed by elastic bandage wrapping from toes to several centimeters above the knee, and following this, medium thrombo embolic deterrent hose thigh-high were applied carefully to each leg for gentle compression.
Patients were counseled about excessive walking and sitting for the day after surgery.
Overall satisfaction 1 year after calf contouring was rated on a scale of 1 (poor), 2 (fair), 3(good), 4 (very good), and 5(excellent).
RESULTS
Patients were followed up on a regular basis with a mean follow-up of 31 months.
The procedure was well tolerated with minimal discomfort in the postoperative course.
There were no major complications. No hematoma, infection, or skin sloughs were observed throughout early follow-up. Postoperative swelling and edema were limited, and edema nearly completely subsided by 3 weeks following surgery. There were no major motor or sensory disturbances in the lower legs. No permanent paresthesia was seen in any of the cases.
Late complications were limited. There was a wound dehiscence in one case (5%) and implant displacement in another (5%). The case involving implant displacement involved use of a short implant (13.9 cm length with 150 cm3 volume). The implant was subsequently replaced with a longer one. Rupture, leaking, or palpability of implants were not observed. No capsular contracture or compartment syndrome occurred.
Change in diameter of proximal and distal lower legs was measured at least 6 months after surgery. Mean diameter change of the proximal lower legs was 2.16 cm and 1.77 cm in the distal lower legs.
Overall satisfaction rate was highly satisfactory. Eighty-one percent of the patients rated their results. The results were as follows: 82% rated as “excellent” to “good”; 18% rated as good (Figs. 4A, B and 5A, B). The result of endoscopic fasciotomy was clearly noticeable at the end of the surgery. No functional impairment was seen postoperatively. Comparing the convexity at the inner lower leg, a filling effect of the muscle was seen when the patient was on a raised heel position (Figs. 5A, B and Table 1).
Fig. 4.
A, Preoperative view shows the indentation of the inner part of proximal lower leg. B, Postoperative view of lower legs. A satisfactory filing effect is seen in the proximal medial lower leg.
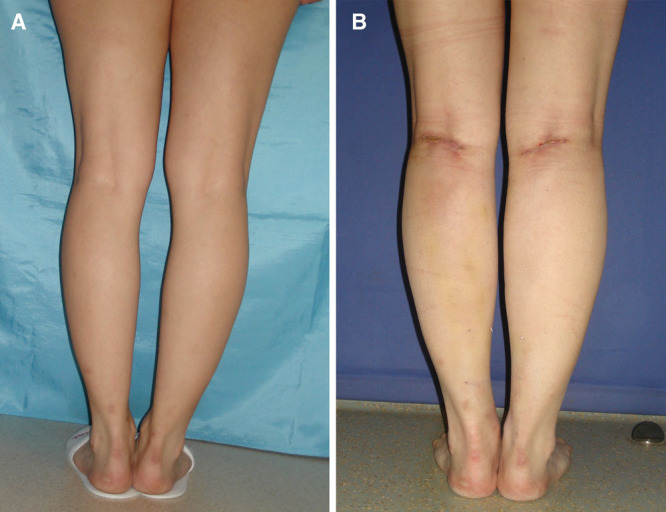
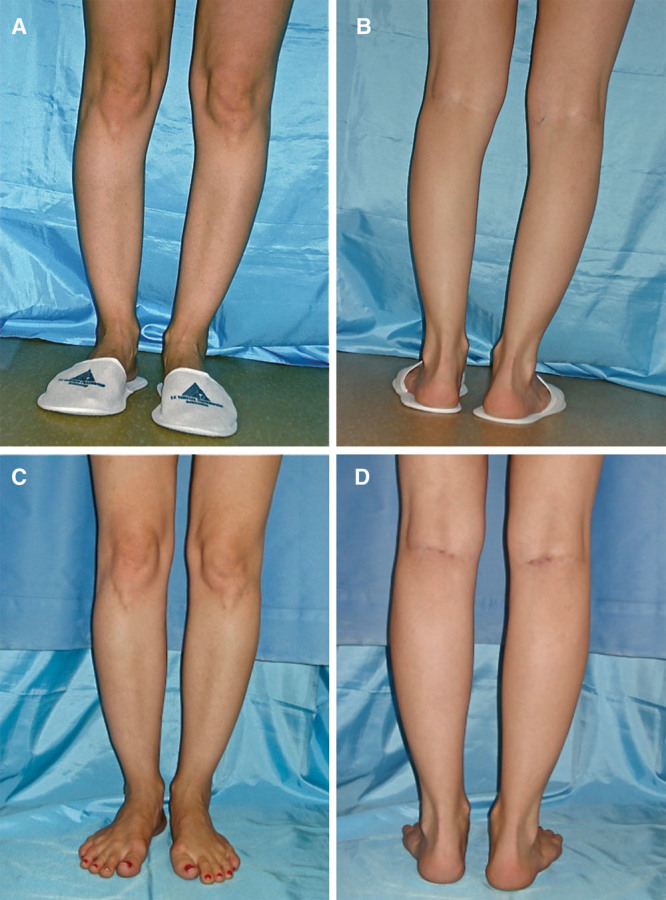
Fig. 5.
A and B, Preoperative views of a patient. C and D, Postoperative views of the patient. Patient was treated with endoscopic fasciotomy, augmentation with implant, and structural fat grafting.
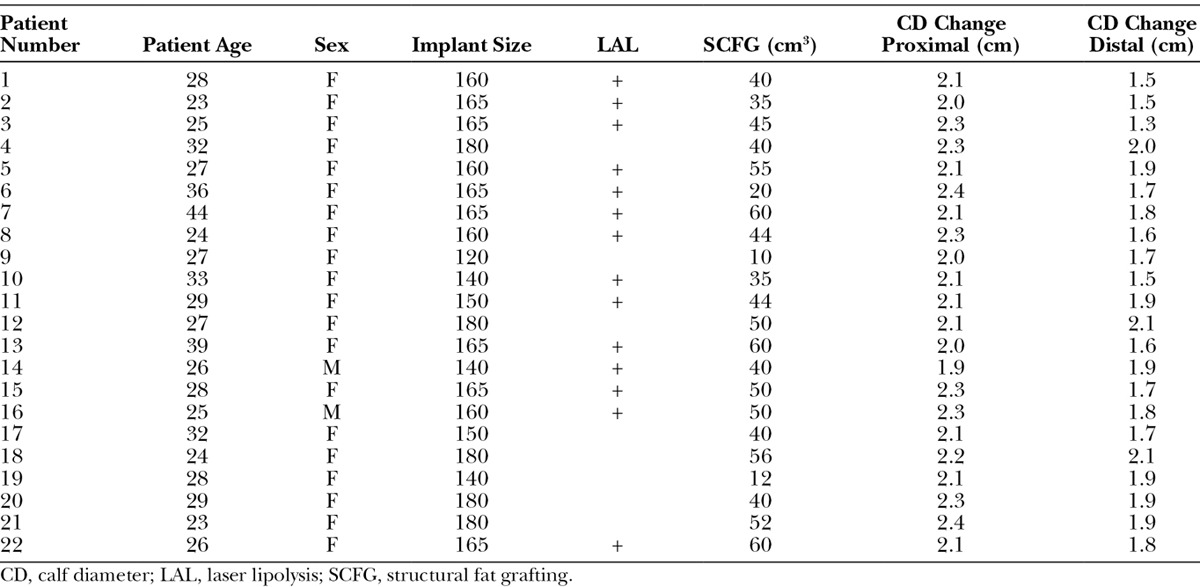
Table 1.
Data About 20 Patients, Including Patient Age, Sex, Implant Size, Whether Laser Lipolysis Done (Denoted as +), Amount of Structural Fat Grafting Done in cm3, and Calf Diameter Increase in Proximal and Distal Lower Leg in cm
DISCUSSION
The muscles around the tibia and fibula largely comprise the anatomic silhouette of the lower leg. Besides the bone, the gastrocnemius and soleus muscles and the fat tissue primarily determine the contour of the lower leg. In particular, the inner leg bulge is caused by the medial belly of the gastrocnemius muscle lying posteriorly on top of the soleus muscle.9 The ratio of leg thickness is mostly dependent on calf muscles. Although the soleus is the more important postural muscle at the ankle, the gastrocnemius muscle, being more superficial and proximal, contributes more to the surface contour of the calf.
It is well known that the aesthetics of the attractive leg was based on the ratios of leg length, thickness, and shape.6,11,12 Interest in calf contouring has caused the development of different techniques dependent on 3 ratios of leg aesthetic where every case needs to be evaluated on an individual basis. First, procedures based on length have led to the use of distraction osteogenesis that has many risks and disadvantages and is not feasible if done only for aesthetic purposes. Second, the procedures based on thickness has led to the development of various techniques including circumferential liposuction,7 ultrasound-assisted lipoplasty,6 autologous fat grafting,13–16 selective neurectomy,8 and partial resection of gastrocnemius muscle.11 Although the reason for thickness of the leg is considerably accumulated amount of fat tissue, naturally the success seems to be related with liposuction or ultrasound-assisted lipectomy.5,6 If the thickness indicates muscular hypertrophy, it seems reasonable to indicate calf reduction procedures.8,11
As stated above, every case needs to be handled individually based on these 3 ratios of length, thickness, and shape. From our standpoint, shape, carrying the characteristics of former two, is the most determinant ratio in selecting which technique is best. In evaluating the shape, if thickness is the main contributing factor of leg aesthetics, then lipoplasty or calf reducing procedures will be the option. Our question was the case in which legs are slender and lack muscular definition but still have noticeable indentations and/or bulges.
In these cases, we suggest a combination of liposuction, structural fat grafting, and calf implant insertion combined with a novel procedure: endoscopic fasciotomy. The ideal candidate has both indentation and bulges in the lower leg. The indentations are mostly due to the lack of gastrocnemius bulge in that area while there is fat accumulation attached to the convexity of the lateral aspect of the lower leg. Here, fasciotomy ensured the correction of medial indentation accentuated with implant and structural fat grafting. Therefore, combining fasciotomy, calf implant, and structural grafting-based augmentation and lipoplasty revealed a satisfactory appearance (Figs. 6A–D, 7A, B, and 8A, B).
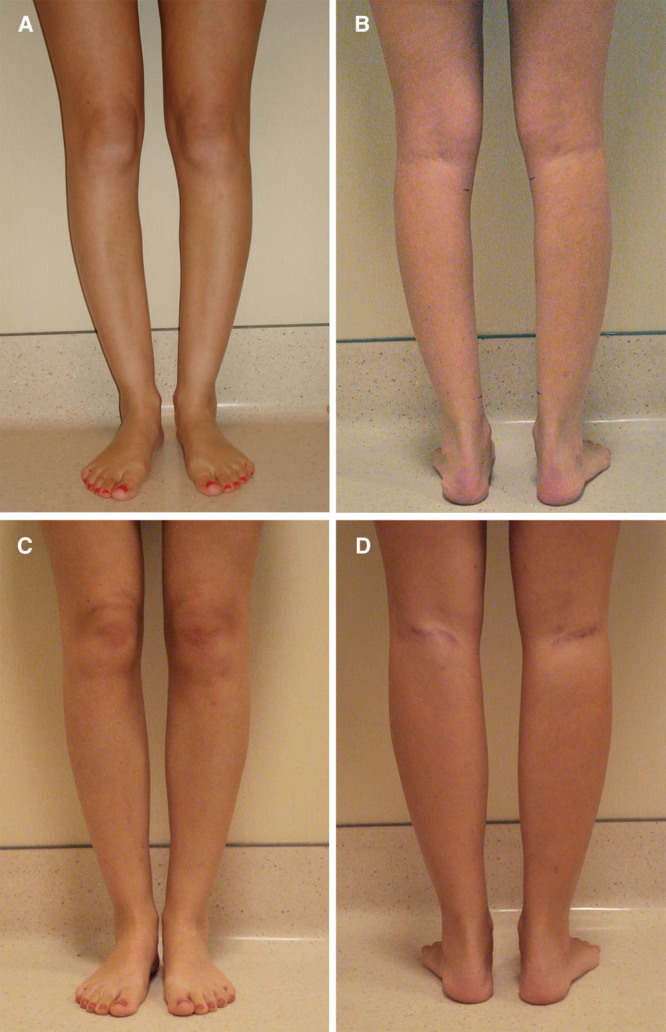
Fig. 6.
A and B, Preoperative views of another patient. C and D, Postoperative views of the patient. Patient was treated with endoscopic fasciotomy, augmentation with implant, and structural fat grafting. Pocket for implant was submuscular.
Fig. 7.
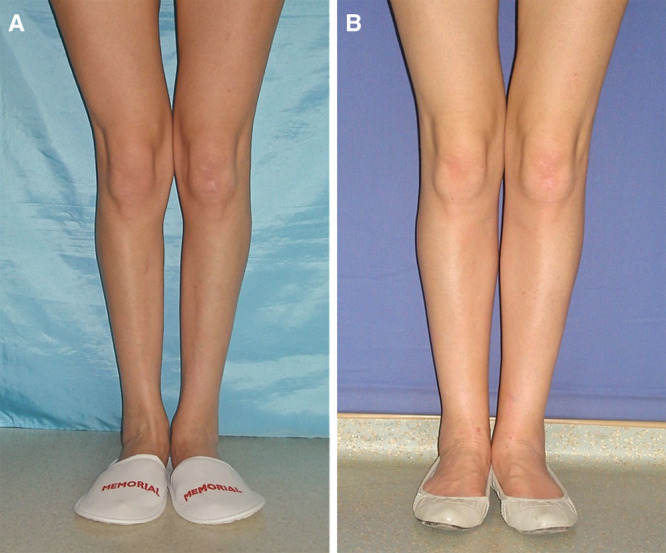
Preoperative view (A) and postoperative view (B) of a patient 1 y after surgery.
Fig. 8.
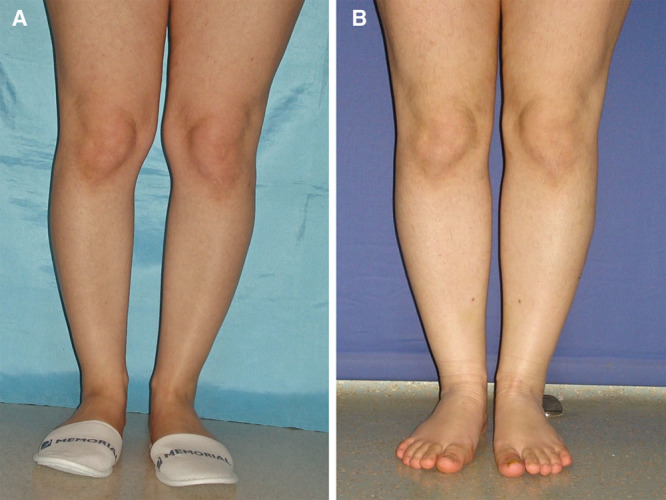
Preoperative (A) and postoperative (B) view of a patient. Please note the satisfactory bulging in all medial contour of the lower leg including proximal and distal parts close to the medial malleolus.
All implants were placed in a submuscular plane in this technique. Although subfascial placement technique is more popular13–16 than submuscular plane,17 we preferred submuscular plane, as it is safe and simple. In subfascial technique, it is crucial to dissect with extreme care to avoid harm to the lesser saphenous vein and the lateral cutaneous sural nerves. In the technique of submuscular placement, the dissection can be made far away from the union of the gastrocnemius muscles where there are no vessels or nerves that could be damaged. Staying above the soleus muscle gives an extra space to avoid the aforementioned vital structures. Submuscular placement resulted in a more natural calf shape as ample muscle tissues cover the implant and prevent the palpability of the implant itself. Besides, continuous movement of muscles ensures a massage effect on implant that might play a role on capsule formation as capsular contracture was not seen in this series.
Calf augmentation with fat transplantation, as an alternative to implants, has been reported in recent literature.13,18–20 Regenerative cell-based strategies such as those encompassing the use of stem cells hold tremendous promise for augmentation of the soft tissue space. From this perspective, stem cell-rich fat grafting for lower leg contouring is an effective and promising technique. Combining the Coleman10 technique with fat grafting is believed to yield satisfactory results by means of fat viability. Increased fat tissue viability is the key for volume durability. It is difficult to estimate a percentage for fat graft survival in this series, but our satisfaction ratio of almost 82% rated as “excellent” to “good” may be an indirect evaluation of volume durability.
Endoscopic release of crural fascia provides many advantages. Selective release of precisely planned areas allows the muscle to gently enhance the medial contour that was deficient and the fascia to better encompass the inserted silicone implant. Under endoscopic vision, an injury to nerves and vessels and other anatomic structures are avoided. Under direct vision, superficial cutaneous branches of sural nerves and lesser saphaneous vein are seen. Therefore, any sensorial or motor disturbances and hematoma are avoided. Selective release of fascia enables to avoid extensive dissection and therefore provides less postoperative edema and discomfort.
CONCLUSIONS
As a conclusion, the contour of the lower leg has been a subject of cosmetic surgery for years. Although the demand for this surgery is increasing, the number of surgeons performing this procedure is conspicuously small. In this article, personal experience is presented. We have shown that lower leg contouring augmentation combined with endoscopic fasciotomy, structural fat grafting, and liposuction to the lower leg is a very powerful aesthetic tool in the appropriate candidate. Endoscopic fasciotomy technique with calf implant and structural fat grafting for improved lower leg aesthetics is a simple, effective, reliable, and predictable approach for calf recontouring.
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Carlsen LN. Calf augmentation—a preliminary report. Ann Plast Surg. 1979;2:508–510. doi: 10.1097/00000637-197906000-00009. [DOI] [PubMed] [Google Scholar]
- 2.Illouz YG. Surgical remodeling of the silhouette by aspiration lipolysis or selective lipectomy. Aesthetic Plast Surg. 1985;9:7–21. doi: 10.1007/BF01570678. [DOI] [PubMed] [Google Scholar]
- 3.Illouz YG, De Villar YT. Body Sculpturing by Lipoplasty. New York: Churchill-Livingstone; 1989. pp. 270–280. [Google Scholar]
- 4.Reed LS. Lipoplasty of the calves and ankles. Clin Plast Surg. 1989;16:365–368. [PubMed] [Google Scholar]
- 5.Mladick RA. Lipoplasty of the calves and ankles. Plast Reconstr Surg. 1990;86:84–93. discussion 94. [PubMed] [Google Scholar]
- 6.Madick RA. Advances in liposuction contouring of calves and ankles. Plast Reconstr Surg. 1999;104:823–831. [PubMed] [Google Scholar]
- 7.Ersek RA, Salisbury AV. Circumferential liposuction of knees, calves, and ankles. Plast Reconstr Surg. 1996;98:880–883. doi: 10.1097/00006534-199610000-00024. [DOI] [PubMed] [Google Scholar]
- 8.Kim GI, Hwong SH, Lew JM, et al. Endoscope-assisted calf reduction in Orientals. Plast Reconstr Surg. 2000;106:713–718. [PubMed] [Google Scholar]
- 9.Aiache A. Leg contouring with calf implants. Clin Plast Surg. 1996;23:737–749. [PubMed] [Google Scholar]
- 10.Coleman SR. Structural fat grafting: more than a permanent filler. Plast Reconstr Surg. 2006;118(3 Suppl):108S–120S. doi: 10.1097/01.prs.0000234610.81672.e7. [DOI] [PubMed] [Google Scholar]
- 11.Lemperle G, Exner K. The resection of gastrocnemius muscles in aesthetically disturbing calf hypertrophy. Plast Reconstr Surg. 1998;102:2230–2236. doi: 10.1097/00006534-199811000-00064. [DOI] [PubMed] [Google Scholar]
- 12.von Szalay L. Calf augmentation: a new calf prosthesis. Plast Reconstr Surg. 1985;75:83–87. doi: 10.1097/00006534-198501000-00018. [DOI] [PubMed] [Google Scholar]
- 13.Guerrerosantos J. Autologous fat grafting for body contouring. Clin Plast Surg. 1996;23:619–631. [PubMed] [Google Scholar]
- 14.de la Pen˜a-Salcedo JA, Soto-Miranda MA, Lopez-Salguero JF. Calf implants: a 25-year experience and an anatomical review. Aesthetic Plast Surg. 2012;36:261–270. doi: 10.1007/s00266-011-9812-y. [DOI] [PubMed] [Google Scholar]
- 15.Dini M, Innocenti A, Lorenzetti P. Aesthetic calf augmentation with silicone implants. Aesthetic Plast Surg. 2002;26:490–492. doi: 10.1007/s00266-002-1016-z. [DOI] [PubMed] [Google Scholar]
- 16.Pereira LH, Nicaretta B, Sterodimas A. Bilateral calf augmentation for aesthetic purposes. Aesthetic Plast Surg. 2012;36:295–302. doi: 10.1007/s00266-011-9799-4. [DOI] [PubMed] [Google Scholar]
- 17.Kalixto MA, Vergara R. Submuscular calf implants. Aesthetic Plast Surg. 2003;27:135–138. doi: 10.1007/s00266-002-0071-9. [DOI] [PubMed] [Google Scholar]
- 18.Stampos M, Xepoulias P. Fat transplantation for soft tissue augmentation in the lower limbs. Aesthetic Plast Surg. 2001;25:256–261. doi: 10.1007/s002660010132. [DOI] [PubMed] [Google Scholar]
- 19.Pereira LH, Sterodimas A. Composite body contouring. Aesthetic Plast Surg. 2009;33:616–624. doi: 10.1007/s00266-009-9348-6. [DOI] [PubMed] [Google Scholar]
- 20.Veber M, Jr, Mojallal A. Calf augmentation with autologous tissue injection. Plast Reconstr Surg. 2010;125:423–424. doi: 10.1097/PRS.0b013e3181c49724. author reply 424. [DOI] [PubMed] [Google Scholar]