

Abstract
Aim:
The aim of this in vitro study was to evaluate the effects of different ultrasonic surgical-tips and power-settings on micro-leakage of root-end filling material.
Materials and Methods:
The root canals were instrumented using rotary-files and were filled with tapered gutta-percha and root canal sealer using a single-cone technique. The apical 3 mm of each root was resected and the roots were divided into six experimental groups; negative and positive control groups. Root-end cavities were prepared with diamond-coated, zirconum-nitride-coated and stainless-steel ultrasonic retro-tips at half-power and high-power settings. The time required to prepare the root-end cavities for each group was recorded. Root-end cavities were filled with Super-EBA. Leakage values of all samples evaluated with glucose penetration method on 7, 14, 21 and 28th days. The results were statistically analyzed with Kruskal-Wallis and Hollander-Wolfe tests.
Results:
The mean time required to prepare retro cavities using diamond-coated surgical tip at high-power setting was significantly less than other groups (P < 0.01). There were no statistically significant differences in the glucose penetration between the groups at first and second weeks (P > 0.01). Diamond-coated surgical tip showed the least leakage at high-power setting at 3rd and 4th weeks (P < 0.01).
Conclusions:
Under the conditions of this study, cavity preparation time was the shortest and the leakage of the root-end filling was the least when diamond-coated retro-tip used at high-power setting.
Keywords: Root-end surgery, sealing ability, ultrasonic retro-tips
INTRODUCTION
The success rate of conventional endodontic therapy is 85-95%.[1] If conventional endodontic treatment is unsuccessful, non-surgical root canal retreatment will eliminate the problem.[2,3] Retreatment of root canal is not possible because of natural, restorative or iatrogenic obstructions, endodontic surgery is indicated.[4] Root-end surgery includes surgical debridement of pathological peri-radicular tissue, root-end resection, root-end cavity preparation and filling of the root-end cavity to seal the root canal effectively.[5]
Traditionally, the root-end cavity is prepared with burs used with low-speed handpiece. Cavity preparation with burs has some disadvantages including limited operative field and root-end bevel, which increases the number of exposed dentinal tubules on the root-end surface.[4,6] Ultrasonic surgical tips have been introduced as an alternative to the burs for root-end cavity preparation[7], and was able to solve some of these problems.[6] Ultrasonic root-end preparation allows cleaner and deeper cavity centered in the root canal and reduced bevel angle.[4,6]
There are several ultrasonic surgical tips with different shapes and sizes. The first tips that were produced for endodontic apical surgery were made of stainless steel. Some tips have special surface coatings to increase their cutting efficiency. Diamond-coated ultrasonic tips are very efficient for removing gutta-percha from the root-end cavity.[8] Diamond-coated retro-tips abrade dentin more quickly and have been developed to minimize dentinal fractures. Therefore, the root-end cavity preparation time is shorter with diamond-coated retro-tips.[9] Also, zirconum-nitride-coated tips are very efficient and provide good vision.[8]
The recommended power setting on ultrasonic units to prepare the root-end cavity varies from medium to high.[10] Lot of studies evaluated the effects of power settings of ultrasonic units on root-end cavity preparation. Some authors reported that the power setting of ultrasonic unit alter the occurrence of cracks and chipping.[11,12,13]
In this in vitro study, glucose penetration method which was developed by Xu et al. (2005) and modified by De-Deus et al. (2008) was used to asses the sealing ability of root-end fillings.[14,15] Glucose leakage method has an advantage that the specimens are not destroyed and the amount of glucose that leaked through the root-canal filling could be determined quantitatively.[14]
The purpose of this in vitro study was to evaluate the effects of three different ultrasonic retro-tips (diamond-coated, zirconum nitride-coated and stainless steel) and the power settings (high and half) of ultrasonic device on the root-end cavity preparation time and sealing ability of root-end filling.
MATERIALS AND METHODS
A total of 100 extracted, single-rooted human teeth were selected for this study. Soft tissue, calculus and bone remnants on the root surface were removed with periodontal curettes. The coronal parts of the teeth were sectioned at the cemento-enamel junction with a low-speed diamond saw, under continuous water spray, to obtain a root length of about 15 mm and the working length was determined 1 mm short of anatomical apex with K file. The root canals were instrumented with a crown-down technique using ProTaper rotary files up to file F3 at the working length. The root canals were irrigated with 2.5% sodium hypochlorite solution after each instrument. A final rinse with 3 ml of 17% ethylenediaminetetraacetic acid (EDTA), 2.5% NaOCl and distilled water was performed to remove the smear layer. The roots were randomly divided into 6 experimental groups with 15 teeth each and two control groups (negative and positive) with 5 teeth each. The root canals were dried with paper-points and filled with ProTaper F3 gutta-percha and AH Plus root canal sealer using a single-cone technique. The specimens in positive control group were filled with ProTaper F3 gutta-percha without root canal sealer. The specimens were stored at 37°C and 100% humidity for 7 days. The apical 3 mm of each root was resected perpendicular to the long axis of the root using fissure bur in a high-speed hand piece with continuous water spray. Root-end preparation of each group was performed under internal-water cooling as follows;
Group one: Root-end cavities having depth of 3 mm were prepared with a diamond-coated ultrasonic surgical tip S12 90ND (Satelec/Acteon, Merignac, France) at high-power setting of ultrasonic device. (DC-HiP)
Group two: Root-end cavities having depth of 3 mm were prepared with a diamond-coated ultrasonic surgical tip S12 90ND at half power setting of ultrasonic device. (DC-HaP)
Group three: Root-end cavities having depth of 3 mm were prepared with a zirconum nitride-coated ultrasonic surgical tip ProUltra (Dentsply, Maillefer, Ballaigues, Switzerland) at high-power setting of ultrasonic device. (ZNC-HiP)
Group four: Root-end cavities having depth of 3 mm were prepared with a zirconum nitride-coated ultrasonic surgical tip ProUltra at half power setting of ultrasonic device. (ZNC-HaP)
Group five: Root-end cavities having depth of 3 mm were prepared with a stainless steel ultrasonic surgical tip UT-3-S (SybronEndo/Analytic, Orange, CA, USA) at high-power setting of ultrasonic device. (SS-HiP)
Group six: Root-end cavities having depth of 3 mm were prepared with a stainless steel ultrasonic surgical tip at half-power setting of ultrasonic device. (SS-HaP)
Positive Control: Root-end cavities having depth of 3 mm were prepared with a diamond-coated ultrasonic surgical tip at half-power setting of ultrasonic device.
Negative control: Root-end cavities having depth of 3 mm were prepared with a diamond-coated ultrasonic surgical tip at half-power setting of ultrasonic device.
The time required to complete the root-end cavity preparation having depth of 3 mm was recorded. Endodontic plugger was placed into the root-end cavities to prepare standardized cavity width and depth. Root-end cavities in experimental and negative control groups were dried with air and filled with zinc oxide-eugenol based Super-EBA (Bosworth Co, Skokie, IL) regular set-filling material. In the positive control group, root-end cavities were not filled. The specimens were stored at 37°C and 100% humidity for 7 days to allow the complete setting of root-end filling.
In the positive control and experimental groups, the root surface was coated twice with nail varnish except the apical and coronal surfaces. In the negative control group, all root surfaces were coated twice with nail varnish.
Evaluation of leakage
All samples were placed into a modified glucose leakage model. The coronal 7 mm of the roots were embedded in acrylic resin to form a cylinder around the samples. The acrylic resin block around the root was individually connected to a 16-cm long plastic pipette with a silicone tube of which diameter was 5 mm. The assembly was then placed in a sterile glass bottle with a screw cap. In total, 3 ml of 0.2% NaN3 was injected into the glass bottle so that the root samples were immersed in the solution. Cyanoacrylate adhesive was used to seal all interfaces. The tracer used in the present study was a 1 mol L-1 glucose solution. About 5 ml of 1 mol L-1 glucose solution containing 0.2% NaN3 was injected into the plastic pipette until the level of the solution was 14 cm higher than the coronal surface of the root, which created a hydrostatic pressure of 1.5 kPa or 15 cm H2 O.[14] To assure an open system, 22-gauge needle was used in the screw cap. The specimens were placed into an incubator at 37°C temperature during test period.
A total of 100 μL of the solution was drawn from the glass bottle by using a micropipette at 7, 14, 21 and 28th days. The same amount of 0.2% NaN3 was added to the glass bottle reservoir to maintain a constant volume of 3 ml. The samples were then analyzed with a Glucose kit (Flex, Siemens) in a spectrophotometer at a wavelength 340 nm. Concentration of glucose in the lower chamber was calculated in mmol/L.
Statistical analysis
The time needed for each preparation and glucose leakage results were statistically analyzed with nonparametric Kruskal-Wallis test followed by Hollander-Wolfe test. The P values less than 0.01 were considered significant.
RESULTS
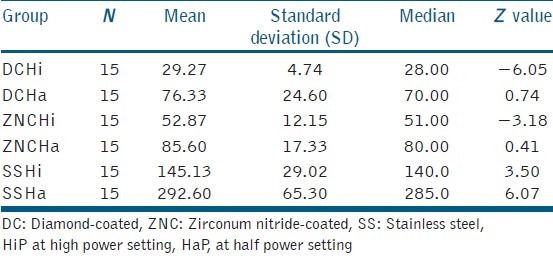
The mean, standard deviation, median and Z values of the preparation time in each group are shown in Table 1. The diamond-coated retro tip-High power group required the least time and the stainless steel retro tip-Half power group required the most time for root-end cavity preparation (P < 0.01). There were no differences between the zirconum nitride-coated retro tip-Half power and diamond-coated retro tip-Half power groups when the cavity preparation time was evaluated. Zirconum nitride-coated retro tip-High power group prepared the root-end cavities more quickly than diamond-coated retro tip-Half power group. High-power setting of ultrasonic unit allowed faster root-end preparation than half power setting.
Table 1.
Preparation time (second) needed for each group
Glucose leakage
The negative control group showed no leakage during the experimental period. The positive control group leaked immediately. In glucose leakage test, there were no statistically significant differences between the groups at first and second weeks (P > 0.01).
There were statistically significant differences between the experimental groups at third week (P < 0.01). Diamond-coated retro tip-High power group showed the least leakage. The most leakage values were found in Zirconum nitride-coated retro tip-High power group. Diamond-coated retro tip-Half power group showed more leakage than diamond-coated retro tip-High power group. There were no statistical differences between the other groups at third week.
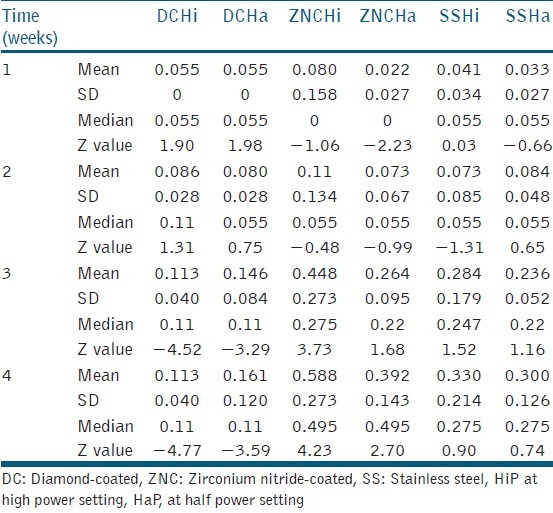
At 4th week, the differences between the groups were significant (P < 0.01). Diamond-coated retro tip-High power group showed the least leakage and Zirconum nitride-coated retro tip-High power group showed the most leakage values. Zirconum nitride-coated retro tip-Half power group showed less leakage than Zirconum nitride-coated retro tip-High power group. There was no difference between the stainless steel groups. Diamond-coated tips showed more leakage when they were used at half-power settings. Mean glucose leakage values of each group were shown in Figure 1. The mean, standard deviation, median and Z values of glucose leakage at each week are shown in Table 2.
Figure 1.
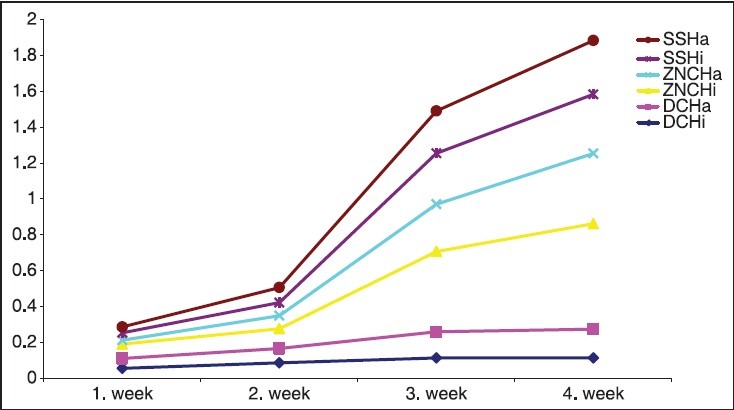
Graphical presentation of mean glucose leakage values
Table 2.
Glucose leakage (mmol/L) along root-end fillings
DISCUSSION
Ultrasonic root-end cavity preparation techniques have gained popularity.[16] The disadvantage of ultrasonic retro-tips is the occurrence of cracks on the root surface during the root-end cavity preparation.[1] Diamond-coated and zirconum nitride-coated retro-tips were produced to improve the performance of ultrasonic retro-tips.[16] Diamond coating will abrade dentin using the side of the instrument's tip rather than the chipping effect of uncoated instruments. This may help to minimize or prevent the incidence of cracking during retrograde cavity preparation.[17]
In the study of Frank et al. (1996), stainless steel retro-tips produced higher number of infractions when used at high-power setting of ultrasonic device.[11] Layton et al. (1996) used stainless steel retro-tips and found no significant differences in the number of teeth with cracks when comparing the high-power and low-power settings of ultrasonic unit. However, ultrasonic root-end preparation with stainless steel retro-tip at high power resulted in a significantly greater number of canal cracks per tooth than the root-end preparation at low-power setting.[12] Conversely, Gray et al. (2000) reported that different power settings of an ultrasonic unit did not significantly affect the occurrence of cracks and chipping using stainless steel retro-tips.[18] Min et al. (1997) found no differences in the crack length or depth when using stainless steel tips at high-power and low-power settings.[19]
Peters et al. (2001) and Ishikawa et al. (2003) showed that diamond-coated retro-tips needed a shorter root-end cavity preparation time than stainless steel retro-tips.[7,10] Navarre & Steiman (2002) reported that zirconum nitride-coated retro-tip prepared root-end cavity faster than the stainless steel tip.[9] In this present study, diamond-coated retro-tips needed less time than the stainless steel and zirconium nitride-coated retro-tips.
Sealing abilities of root-end filling materials have been evaluated with several methods such as dye leakage[3], bacterial penetration[4], radioactive isotopes[20], electrochemical[21] and fluid filtration.[3] Dye leakage method often yielded a large variation of the result. To reproduce and compare this method could be hard.[14,22] In bacterial penetration method, maintaining aseptic conditions during the experiment can be difficult and results might be different with the bacterial species used.[14] In the fluid filtration method, the measurement time, the applied pressure, the diameter and the length of the bubble might influence[14,23] the results. In this study, glucose leakage method in which glucose solution was chosen as the tracer was used to evaluate the micro leakage. The molecular size and physicochemical properties of tracer may affect the results. In this method, glucose was selected as the tracer because of its small molecular size and being a nutrient for bacteria as well.[14]
Ishikawa et al. reported that diamond-coated, stainless steel and zirconum nitride-coated retro-tips showed similar dye leakage values.[7] In the study of Rainwater et al., (2000) there was no significant difference in dye leakage between diamond-coated and stainless steel ultrasonic retro-tips.[24] In this in vitro study, there were no statistically different glucose leakage values between the tested groups at first and second week. However, diamond coated-high power group showed better sealing ability than other groups at fourth and third weeks when evaluated with glucose leakage method. Gondim et al. (2002) reported that no significant differences in chipping and cracking area were detected among treatments with diamond-coated, stainless steel and zirconum nitride-coated tips, but stainless steel retro-tips showed a greater number of teeth with cracking and a larger chipping area, probably due to the longer preparation time needed.[25] Chipping of the cavity margin may affect the leakage of the root-end filling material.[16] Navarre & Steiman (2002) observed no root-end fractures with stainless steel or zirconum nitride-coated tips and showed that the remaining debris was approximately equal with both tips.[9] Microscopic evaluation of root-end cavity surface showed slightly rough cavity margins with zirconum nitride-coated retro-tips and smoother and more rounded margins with stainless steel retro-tips. This remaining debris and rough margins have an effect on clinical success, which is yet to be determined.[9]
Differences between ultrasonic devices could change the vibratory pattern.[16,26] Variation in oscillation of the retro-tip according to the tip design might affect the test results.[16] Different leakage methods and observation times, ultrasonic units and retro-tips might be responsible for the different results of these studies.
CONCLUSION
Under the conditions of this in vitro study, root-end filling showed the best sealing ability when the root-end cavities were prepared with diamond-coated ultrasonic surgical tips at high- power setting. Also, the required cavity preparation time that is important for the cooperation between the surgeon and patient, was the shortest with diamond-coated retro-tip at high-power setting of ultrasonic device.
Footnotes
Source of Support: This study which is a doctoral thesis of Dr. Betul Gunes, was financially supported by BAP coordination of Selcuk University Konya/Turkey. Authors would like to thank to Dr. Ismail Keskin for statistical analysis. This study was presented in the FDI2013 congress.
Conflict of Interest: None declared.
REFERENCES
- 1.Khabbaz MG, Kerezoudis NP, Aroni E, Tsatsas V. Evaluation of different methods for the root-end cavity preparation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:237–42. doi: 10.1016/j.tripleo.2004.02.062. [DOI] [PubMed] [Google Scholar]
- 2.Ruddle CJ. Micro-endodontic nonsurgical retreatment. Dent Clin North Am. 1997;41:429–54. [PubMed] [Google Scholar]
- 3.Taschieri S, Del Fabbro M, Francetti L, Testori T. Effect of root-end resection and root-end filling on apical leakage in the presence of core-carrier root canal obturation. Int Endod J. 2004;37:477–82. doi: 10.1111/j.1365-2591.2004.00827.x. [DOI] [PubMed] [Google Scholar]
- 4.Chailertvanitkul P, Saunders WP, Saunders EM, MacKenzie D. Polymicrobial coronal leakage of super EBA root-end fillings following two methods of root-end preparation. Int Endod J. 1998;31:348–53. doi: 10.1046/j.1365-2591.1998.00164.x. [DOI] [PubMed] [Google Scholar]
- 5.Gutmann JL, Harrison JW. Surgical endodontics. 1st ed. Boston: Blackwell Scientific Publications; 1991. [Google Scholar]
- 6.Rosales-Leal JI, Olmedo-Gaya V, Vallecillo-Capilla M, Luna-del Castillo JD. Influence of cavity preparation technique (rotary vs. ultrasonic) on microleakage and marginal fit of six end-root filling materials. Med Oral Patol Oral Cir Bucal. 2011;16:e185–9. doi: 10.4317/medoral.16.e185. [DOI] [PubMed] [Google Scholar]
- 7.Ishikawa H, Sawada N, Kobayashi C, Suda H. Evaluation of root-end cavity preparation using ultrasonic retrotips. Int Endod J. 2003;36:586–90. doi: 10.1046/j.1365-2591.2003.00676.x. [DOI] [PubMed] [Google Scholar]
- 8.Stropko JJ, Doyon GE, Gutmann JL. Root-end management: Resection, cavity preparation, and material placement. Endod Topics. 2005;11:131–51. [Google Scholar]
- 9.Navarre SW, Steiman HR. Root-end fracture during retropreparation: A comparison between zirconium nitride-coated and stainless steel microsurgical ultrasonic instruments. J Endod. 2002;28:330–2. doi: 10.1097/00004770-200204000-00018. [DOI] [PubMed] [Google Scholar]
- 10.Peters CI, Peters OA, Barbakow F. An in vitro study comparing root-end cavities prepared by diamond-coated and stainless steel ultrasonic retrotips. Int Endod J. 2001;34:142–8. doi: 10.1046/j.1365-2591.2001.00367.x. [DOI] [PubMed] [Google Scholar]
- 11.Frank RJ, Antrim DD, Bakland LK. Effect of retrograde cavity preparations on root apexes. Endod Dent Traumatol. 1996;12:100–3. doi: 10.1111/j.1600-9657.1996.tb00105.x. [DOI] [PubMed] [Google Scholar]
- 12.Layton CA, Marshall JG, Morgan LA, Baumgartner JC. Evaluation of cracks associated with ultrasonic root-end preparation. J Endod. 1996;22:157–60. doi: 10.1016/S0099-2399(96)80091-4. [DOI] [PubMed] [Google Scholar]
- 13.Waplington M, Lumley PJ, Walmsley AD. Incidence of root face alteration after ultrasonic retrograde cavity preparation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83:387–92. doi: 10.1016/s1079-2104(97)90247-x. [DOI] [PubMed] [Google Scholar]
- 14.Xu Q, Fan MW, Fan B, Cheung GS, Hu HL. A new quantitative method using glucose for analysis of endodontic leakage. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99:107–11. doi: 10.1016/j.tripleo.2004.06.006. [DOI] [PubMed] [Google Scholar]
- 15.De-Deus G, Soares J, Leal F, Luna AS, Fidel S, Fidel RA. Similar glucose leakage pattern on smear-covered, EDTA-treated and BioPure MTAD-treated dentin. J Endod. 2008;34:459–62. doi: 10.1016/j.joen.2008.01.005. [DOI] [PubMed] [Google Scholar]
- 16.Taschieri S, Testori T, Francetti L, Del Fabbro M. Effects of ultrasonic root end preparation on resected root surfaces: SEM evaluation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:611–8. doi: 10.1016/j.tripleo.2004.04.004. [DOI] [PubMed] [Google Scholar]
- 17.Brent PD, Morgan LA, Marshall JG, Baumgartner JC. Evaluation of diamond-coated ultrasonic instruments for root-end preparation. J Endod. 1999;25:672–5. doi: 10.1016/S0099-2399(99)80353-7. [DOI] [PubMed] [Google Scholar]
- 18.Gray GJ, Hatton JF, Holtzmann DJ, Jenkins DB, Nielsen CJ. Quality of root-end preparations using ultrasonic and rotary instrumentation in cadavers. J Endod. 2000;26:281–3. doi: 10.1097/00004770-200005000-00007. [DOI] [PubMed] [Google Scholar]
- 19.Min MM, Brown CE, Jr, Legan JJ, Kafrawy AH. In vitro evaluation of effects of ultrasonic root-end preparation on resected root surfaces. J Endod. 1997;23:624–8. doi: 10.1016/S0099-2399(97)80174-4. [DOI] [PubMed] [Google Scholar]
- 20.Haikel Y, Wittenmeyer W, Bateman G, Bentaleb A, Allemann C. A new method for the quantitative analysis of endodontic microleakage. J Endod. 1999;25:172–7. doi: 10.1016/S0099-2399(99)80136-8. [DOI] [PubMed] [Google Scholar]
- 21.Alhadainy HA, Elsaed HY, Elbaghdady YM. An electrochemical study of the sealing ability of different retrofilling materials. J Endod. 1993;19:508–11. doi: 10.1016/S0099-2399(06)81492-5. [DOI] [PubMed] [Google Scholar]
- 22.Wu MK, Wesselink PR. Endodontic leakage studies reconsidered. Part I. Methodology, application and relevance. Int Endod J. 1993;26:37–43. doi: 10.1111/j.1365-2591.1993.tb00540.x. [DOI] [PubMed] [Google Scholar]
- 23.Pommel L, Camps J. Effects of pressure and measurement time on the fluid filtration method in endodontics. J Endod. 2001;27:256–8. doi: 10.1097/00004770-200104000-00003. [DOI] [PubMed] [Google Scholar]
- 24.Rainwater A, Jeansonne BG, Sarkar N. Effect of ultrasonic root-end preparation on microcrack formation and leakage. J Endod. 2000;26:72–5. doi: 10.1097/00004770-200002000-00003. [DOI] [PubMed] [Google Scholar]
- 25.Gondim E, Jr, Figueiredo Almeida de Gomes BP, Ferraz CC, Teixeira FB, de Souza-Filho FJ. Effect of sonic and ultrasonic retrograde cavity preparation on the integrity of root apices of freshly extracted human teeth: Scanning electron microscopy analysis. J Endod. 2002;28:646–50. doi: 10.1097/00004770-200209000-00005. [DOI] [PubMed] [Google Scholar]
- 26.Ahmad M, Roy RA, Kamarudin AG, Safar M. The vibratory pattern of ultrasonic files driven piezoelectrically. Int Endod J. 1993;26:120–4. doi: 10.1111/j.1365-2591.1993.tb00553.x. [DOI] [PubMed] [Google Scholar]