

Abstract
Complete cleaning and shaping is the key to successful endodontic treatment. A thorough understanding of the internal anatomy and morphology of the root canal system is an important consideration when performing cleaning and shaping procedures. Mandibular premolars are one of the most difficult teeth to treat endodontically because of aberrant root canal anatomy. This article describes case series of mandibular premolars with variations in root canal anatomy treated successfully by conventional endodontic treatment.
Keywords: Endodontic, mandibular premolars, root canal anatomy
INTRODUCTION
The successful outcome of an endodontic treatment demands the thorough knowledge of the internal anatomy and morphology of the root canal system.[1,2] The risk of missing anatomy during root canal treatment is high because of the complexity of the root canal system. Hoen and Pink[3] reported 42% incidence of missed canals or roots in teeth requiring retreatment.
Variations in root canal morphology were suggested as most likely reason of flare ups and failures. Untreated canals may be associated with a remarkable variety of symptoms ranging from asymptomatic teeth to acute responses to hot and cold stimuli and from slight sensitivity to percussion and/or palpation to acute abscesses.
Slowey et al., (1979)[4] stated that variations in root canal anatomy of mandibular premolars presents an endodontic challenge to treat them successfully. The incidence of roots and root canals in these teeth varies considerably in the literature. Zillich and Dowson[5] in 1973 analysed that 23.1% of mandibular first premolars had two or three root canals radiographically. Vertucci[6] found 25.5% of 400 mandibular premolars had two apical openings and 0.5% of the teeth had three apical openings. Root canal morphology varies in different ethnic groups.
Table 1 highlights literature review indicating variations in roots and root canals in India. The endodontic treatment of mandibular premolars with aberrant canal configuration can be diagnostically and technically challenging. In light of these observations this case series insight different case of mandibular premolars with variable canal pattern treated successfully by conventional endodontic treatment.
Table 1.
Literature review indicating variations in roots and root canals in India

CASE REPORT 1
Mandibular first premolar with Weine's type 3 pattern
A 24-year-old male patient reported to the Department of Conservative dentistry and Endodontics with a chief complaint of pain in mandibular left back tooth region. The medical history was non-contributory. Clinical examination revealed amalgam restorations in relation to left posterior mandibular region. Distal caries were present with respect to left mandibular second premolar. Left mandibular first and second premolars were tender on percussion.
Radiographic examination revealed pulpal involvement and widening of periodontal ligament with respect to mandibular left first and second premolars. Based on the clinical and radiographic findings, a diagnosis of “symptomatic apical periodontitis” was made for these teeth. Endodontic treatment was planned. The preoperative radiograph showed two separate root canals in first premolar (Weine Type 3) and one canal in second premolar [Figure 1a].
Figure 1.
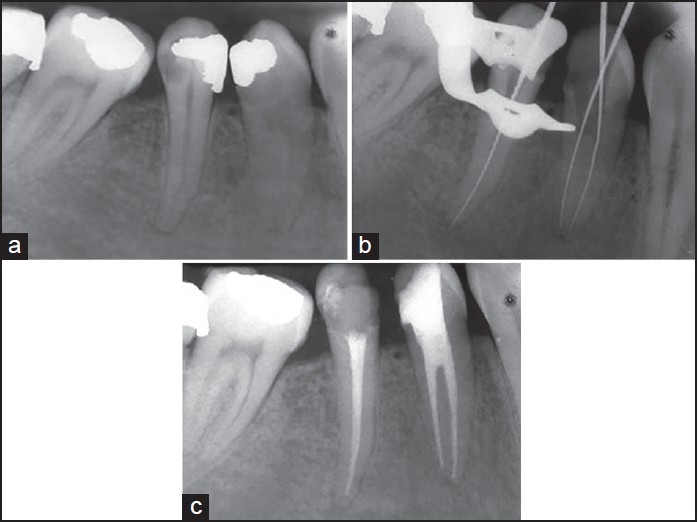
(a) Diagnostic radiograph (b) Working length radiograph (c) Postobturation radiograph
The treatment plan was explained to the patient and after obtaining his consent, the tooth was anesthetized with 2% lidocaine solution by way of inferior alveolar nerve block of the left side. Subsequently, the tooth was isolated with rubber dam. Endodontic access cavity was prepared with round diamond burs in a high-speed air rotor handpiece. Since the tooth was rotated, the access opening was modified accordingly. After extirpation of the pulpal tissue, a working length determination radiograph was obtained with K files placed in the root canals (buccal and lingual canals) [Figure 1b].
Following the working length determination, the root canals were prepared with a crown down technique with copious irrigation using 5% sodium hypochlorite solution. After completion of cleaning and shaping, the root canal system was obturated with cold lateral compaction of gutta percha cones using endomethasone sealer. A post-obturation radiograph was obtained and the coronal access cavity was restored [Figure 1c].
CASE REPORT 2
Mandibular second premolar with 2 roots and 2 root canals
A 28-year-old male patient reported to the Department of Conservative dentistry and Endodontics with a chief complaint of pain in mandibular right back tooth region. The medical history was non-contributory. Clinical examination revealed distal caries with respect to mandibular right second premolar and mesial caries with respect to mandibular right second molar. Both teeth were tender on percussion.
Radiographic examination revealed pulpal involvement and widening of periodontal ligament in relation to mandibular right second premolar and molar. Based on the clinical and radiographic findings, a diagnosis of “symptomatic apical periodontitis” was made for these teeth. Endodontic treatment was planned out.
On the first visit it was decided to perform endodontic treatment of right mandibular second premolar. The preoperative radiograph of the premolar showed two separate roots and canals [Figure 2a]. After anesthetizing the tooth and isolating with rubber dam endodontic access cavity was prepared and enlarged to locate the buccal and palatal orifices. After extirpation of the pulpal tissue, a working length determination radiograph was obtained with K files placed in the root canals [Figure 2b].
Figure 2.
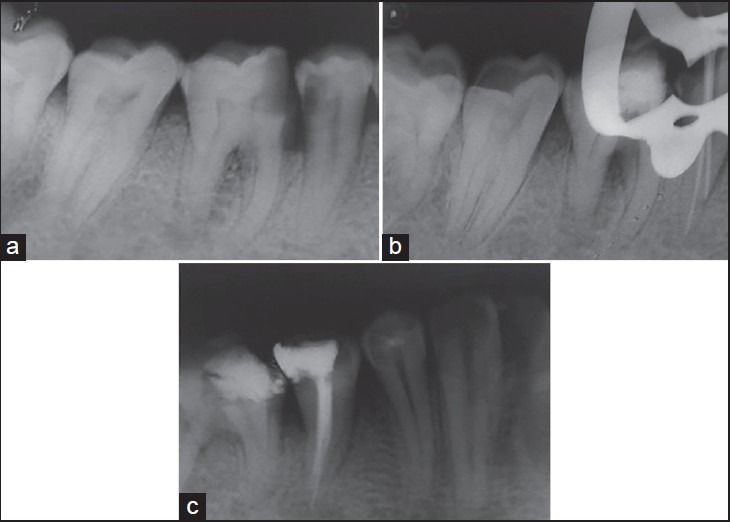
(a) Diagnostic radiograph (b) Working length radiograph (c) Postobturation radiograph
Biomechanical preparation and obturation was done. Radiograph was obtained and the coronal access cavity was restored with respect to mandibular right second premolar [Figure 2c]. The patient did not turn up for the endodontic treatment of mandibular right second molar.
CASE REPORT 3
Mandibular first premolar with 2 roots and 2 root canals
A 38-year-old male patient reported to the Department of Conservative dentistry and Endodontics with a chief complaint of pain in mandibular right back tooth region. The patient already got the treatment started from a general dentist a few days back. Clinical examination revealed temporary restoration with respect to mandibular right first premolar.
Radiographic examination revealed that access opening was already tried by the general dentist [Figure 3a]. It revealed two separate roots and root canals with respect to mandibular right first premolar. Based on the clinical and radiographic findings, a diagnosis of “asymptomatic apical periodontitis” was made for these teeth and endodontic treatment was performed [Figure 3b].
Figure 3.
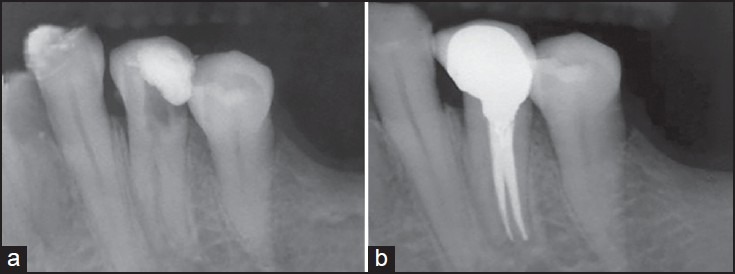
(a) Preoperative radiograph (b) Postoperative radiograph (c) Preoperative radiograph
CASE REPORT 4
Mandibular first premolar with 3 root canals
A 25-year-old female patient reported to the Department of Conservative dentistry and Endodontics for endodontic evaluation of lower right first premolar. Intra oral periapical radiograph revealed aberrant canal pattern with respect to this tooth [Figure 4a].
Figure 4.

(a) Preoperative radiograph (b) Postoperative radiograph
After local anesthesia administration and rubber dam isolation, access opening was performed and canals were located. Biomechanical preparation was done using crown down approach. The canal divided into three different canals at the mid level of root. So the canal was coronally flared till the midroot level for achieving ease of instrumentation. After sealer application in all the canals using lentulospiral, master cones were placed in all the three canals simultaneously and obturated with lateral condensation technique [Figure 4b].
CASE REPORT 5
Mandibular first premolar with Weine's type 3 pattern and second premolar with type 2 pattern
A 48-year-old female patient reported to the Department for elective devitalization of left mandibular first and second premolars. Intra-oral periapical radiograph revealed two root canals in relation to these teeth [Figure 5a]. 1st premolar had type 3 Weine's pattern and 2nd premolar had type 2 pattern.
Figure 5.

(a) Preoperative radiograph (b) Postoperative radiograph
After access opening, canals were located. Biomechanical preparation was done and the teeth were obturated with cold lateral compaction of gutta percha cones using endomethasone sealer [Figure 5b].
In all the five cases, access opening were made wider to obtain the straight line access to all the canals. Adequate coronal flaring and using pre-bent hand files in an exploratory fashion to scout the walls of the root canal often help in the location of the apical bifurcations. During cleaning and shaping minimal preparation was done using hand instrumentation to avoid merging of the canals. Irrigation was done using 3% sodium hypochlorite and saline in all the cases. After thorough application of sealer with lentulospiral obturation was done using lateral condensation in all the cases by placing the master cones simultaneously in all the canals and then proceeding with accessory cones placement.
DISCUSSION
The root canal morphology of mandibular premolars can be highly variable and complex and it is often a challenging task to carry out successful endodontic therapy with such teeth. Ethnicity has a significant influence on aberrant anatomy. Two and three canal premolars are seen frequently in black populations.[10,11]
The primary step in root canal treatment is the identification of the internal morphology of canal system as precisely as possible. The anatomical landmark of the pulp chamber floor may help to identify supplementary root canals or root canal aberrations.[12] The careful tactile exploration of the root canal system with hand files is also imperative. Attention to the colour changes on the pulpal floor and wall during inspection instead of searching for defined places might be helpful to locate the orifices.
To obtain predictable results, high-quality pre-operative radiographs should be obtained at different horizontal angulations and carefully evaluated to detect the presence of extra root canal.[11,12] According to Hasheminia and Hashemi (2005) 11.2% of the mandibular second premolars had 2 or more canals.[13]
The root shape, root position, and relative root outline should be carefully determined from the radiograph. The observations made in a study concluded that broad, flat roots are much more likely to contain multiple canals and intracanal ramifications. In such cases, angled radiographic view will reveal the true dimensions of the root canal.[14] The sudden radiographic disappearance of a canal may be evidence of a dividing canal.
Reports have shown that mandibular premolars are possibly the most difficult teeth to treat endodontically due to wide variation in root canal morphology.[15] One of the most difficult aspects of treating this anatomy is the predictable removal of pulp tissue in the isthmus.
This article describes a series of case reports with aberrant morphology of root canals of mandibular premolars and their successful endodontic management. In case 1, the rotated mandibular first premolar with Weine's type 3 pattern was managed by widening the access cavity and locating the buccal and lingual orifices. In cases 2 and 3, mandibular premolar had two roots and two root canals which were also managed in the same way by enlarging the access cavity and finding the orifices. In case 4, mandibular premolar had a single canal which divided into three different canals at the mid level of root. In case 5, 1st premolar had type 3 Weine's pattern and 2nd premolar had type 2 pattern.
CONCLUSION
Successful and predictable endodontic treatment requires knowledge of biology, physiology, and root canal anatomy. The clinician should be astute enough to identify the presence of unusual numbers of roots and their morphology. A thorough knowledge of root canal anatomy and its variations, careful interpretation of the radiograph, close clinical inspection of the floor of pulp chamber and proper modification of access opening are essential for a successful treatment outcome.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ingle J, Beveridge E. Endodontics. 2nd ed. Philadelphia: Lea & Febiger; 1976. [Google Scholar]
- 2.Hoen MM, Pink FE. Contemporary endodontic retreatments: An analysis based on clinical treatment findings. J Endod. 2002;28:834–6. doi: 10.1097/00004770-200212000-00010. [DOI] [PubMed] [Google Scholar]
- 3.Walton R, Torabinejad M. In: Principles and practice of endodontics. 2nd ed. Rudolph P, editor. Philadelphia: WB Saunders Co; 1996. pp. 166–81. [Google Scholar]
- 4.Slowey RR. Root canal anatomy: Road map to successful endodontics. Dent Clin North Am. 1979;23:555–73. [PubMed] [Google Scholar]
- 5.Zillich R, Dowson J. Root canal morphology of mandibular first and second premolars. Oral Surg Oral Med Oral Pathol. 1973;36:738–44. doi: 10.1016/0030-4220(73)90147-3. [DOI] [PubMed] [Google Scholar]
- 6.Vertucci FJ. Root canal morphology of mandibular premolars. J Am Dent Assoc. 1978;97:47–50. doi: 10.14219/jada.archive.1978.0443. [DOI] [PubMed] [Google Scholar]
- 7.Jain A, Bahuguna R. Root canal morphology of mandibular first premolar in gujarati population — An in vitro study. Dent Res J (Isfahan) 2011;8:118–22. [PMC free article] [PubMed] [Google Scholar]
- 8.Sharma D, Mathur M. A computed tomopraphic study of canal variations in maxillary and mandibular premolar teeth in jaipur population: An in vitro study. People J Sci Res. 2011;4:1–5. [Google Scholar]
- 9.Velmurugan N, Sandhya R. Root canal morphology of mandibular first premolar in Indian population: A laboratory study. Int Endod J. 2009;42:54–8. doi: 10.1111/j.1365-2591.2008.01494.x. [DOI] [PubMed] [Google Scholar]
- 10.Chopra P, Bal CS. Study of root canals and their configuration in buccal roots of maxillary first permanent molar. Indian J Dent Res. 1989;1:3–14. [PubMed] [Google Scholar]
- 11.Trope M, Elfenbein L, Tronstad L. Mandibular premolars with more than one root canal in different race groups. J Endod. 1986;12:343–5. doi: 10.1016/S0099-2399(86)80035-8. [DOI] [PubMed] [Google Scholar]
- 12.De Moor RJ, Calberson FL. Root canal treatment in a mandibular second premolar with three root canals. J Endod. 2005;31:310–3. doi: 10.1097/01.don.0000140578.36109.c0. [DOI] [PubMed] [Google Scholar]
- 13.England MC, Jr, Hartwell GR, Lance JR. Detection and treatment of multiple canals in mandibular premolars. J Endod. 1991;17:174–8. doi: 10.1016/S0099-2399(06)82012-1. [DOI] [PubMed] [Google Scholar]
- 14.Hülsmann M. Mandibular first premolar with three root canals. Endod Dent Traumatol. 1990;6:189–91. doi: 10.1111/j.1600-9657.1990.tb00416.x. [DOI] [PubMed] [Google Scholar]
- 15.Zillich R, Dowson J. Root canal morphology of mandibular first and second pre- molars. Oral Surg Oral Med Oral Pathol. 1973;36:738–44. doi: 10.1016/0030-4220(73)90147-3. [DOI] [PubMed] [Google Scholar]