

Abstract
Gynaecological cancer centres have been established nationwide in Germany since 2008 according to the certification system of the German Cancer Society (Deutsche Krebsgesellschaft e. V. [DKG]) and the German Society for Gynaecology and Obstetrics (Deutsche Gesellschaft für Gynäkologie und Geburtshilfe e. V. [DGGG]). However, patient access to the certified gynaecological cancer centres is currently only possible through direct referrals. A longitudinal structure with the corresponding long-term documentation of both the high-grade precursors as well as the cancers does not exist as yet. According to the aims of the National Cancer Plan, a corresponding structure for the cancer entity “cervix carcinoma” should be established. The foundations for such a structure are appropriate diagnostic units that are responsible, after nationwide screening, for clarification according to guideline-conform principles. On the basis of the vote of the certification commission for gynaecological cancer centres under the chairmanship of the DKG, the Working Group for Gynaecological Oncology (Arbeitsgemeinschaft Gynäkologische Onkologie e. V. [AGO]), the Committee on Cervical Pathology and Colposcopy (Arbeitsgemeinschaft Zervixpathologie & Kolposkopie [AG-CPC]) and the DGGG the certification system for gynaecological dysplasia has been established. As a general principle, a distinction is made between the certification of a consulting practice for gynaecological dysplasia and a gynaecological dysplasia facility in order to integrate both outpatient and inpatient health-care facilities into the certification system. In analogy to the further catalogue of requirements from the DKG, quantitative and qualitative minimum numbers are demanded. Furthermore, the requirements of the certification process include a summary of patient information, the applied guidelines, continuing and further training, interdisciplinary cooperation in tumour boards, contents or, respectively, procedure descriptions for consulting practices and the trial participations. Central components of the questionnaire are quality indicators that can be used as specific and measurable elements to evaluate the quality of treatment. After successful pilot certification, finalisation of the updated version of the questionnaire and a completed specialist auditor training course for the certification of gynaecological dysplasia, it will be possible to establish a nationwide treatment system for dysplasia within certified structures.
Key words: dysplasia, certification, gynaecological dysplasia units, gynaecological cancer centres, national cancer plan, screening
Abstract
Zusammenfassung
Die Gynäkologischen Krebszentren wurden nach dem Zertifizierungssystem der Deutschen Krebsgesellschaft e. V. (DKG) und der Deutschen Gesellschaft für Gynäkologie und Geburtshilfe e. V. (DGGG) in Deutschland seit dem Jahr 2008 flächendeckend etabliert. Der Patientinnenzugang zu den zertifizierten Gynäkologischen Krebszentren erfolgt jedoch aktuell nur durch Direkteinweisungen. Eine longitudinale Struktur mit entsprechender Langzeitdokumentation sowohl der hochgradigen Vorstufen wie auch der Karzinome existiert derzeit nicht. Nach den Zielen des Nationalen Krebsplans soll eine entsprechende Struktur für die Karzinomentität Zervixkarzinom etabliert werden. Grundlage für eine solche Struktur sind entsprechende Diagnostikeinheiten, die nach flächendeckendem Screening die Abklärung nach leitlinienkonformen Vorgaben durchführen. Ausgehend von dem Votum der Zertifizierungskommission für Gynäkologische Krebszentren ist unter Federführung der DKG, der Arbeitsgemeinschaft Gynäkologische Onkologie e. V. (AGO), der Arbeitsgemeinschaft Zervixpathologie & Kolposkopie (AG-CPC) und der DGGG das Zertifizierungssystem der Gynäkologischen Dysplasie entstanden. Grundsätzlich wird zwischen der Zertifizierung einer Gynäkologischen Dysplasie-Sprechstunde und der einer Gynäkologischen Dysplasie-Einheit unterschieden, um sowohl den ambulanten als auch den stationären Versorgungsbereich in das Zertifizierungssystem zu integrieren. Analog zu den weiteren Anforderungskatalogen des Zertifizierungssystems der DKG werden quantitative und qualitative Mindestmengen gefordert. Darüber hinaus sind in dem Zertifizierungsverfahren Anforderungen an die Patientinneninformation, die verwendeten Leitlinien, Fort- und Weiterbildung, interdisziplinäre Zusammenarbeit in Tumorkonferenzen, Inhalte bzw. Verfahrensbeschreibungen der Sprechstunden und die Studienteilnahme zusammengefasst. Zentraler Bestandteil des Erhebungsbogens sind Qualitätsindikatoren, die als spezifische und messbare Elemente zur Bewertung der Behandlungsqualität verwendet werden können. Nach erfolgten Pilotzertifizierungen, Finalisierung der aktualisierte Version des Erhebungsbogens und einem durchgeführten Fachauditorenlehrgang für die Zertifizierung der Gynäkologischen Dysplasie kann zeitnah eine flächendeckende Versorgung der Dysplasie in zertifizierten Strukturen erreicht werden.
Schlüsselwörter: Dysplasie, Zertifizierung, gynäkologische Dysplasie-Einheit, gynäkologische Krebszentren, nationaler Krebsplan, Screening
Introduction
On July 1, 1971 the Federal Committee of Physicians and Health announced for the first time their guidelines for the early detection of cancer diseases. At present the subcommittee “method evaluation” of the Federal Joint Committee is formulating the relevant legal requirements in the corresponding cancer screening guidelines (KFE-RL).
With regard to cervical cancer women have the possibility from the age of 20 years of an annual genital examination; this involves specific questions, inspection of the uterus and endocervix with vaginal smear and cytological examination (PAP test) as well as a digital gynaecological inspection of the vagina. In the present system this is carried out in an opportunistic manner. The underlying yearly participant rates currently lie between 43 and 53 % 4, 5 or, respectively, are not even stated when there is large discrepancy between the young and the elderly age groups.
This has been noticed by the control group of the national cancer plan – that was initiated in 2008 by the Federal Ministry for Health (Bundesgesundheitsministerium für Gesundheit [BMG]), the German Cancer Society (Deutsche Krebsgesellschaft e. V. [DKG]), the German Cancer Help (Deutsche Krebshilfe e. V. [DKH]) and the Union of the Germany Tumour Centres (Arbeitsgemeinschaft Deutscher Tumorzentren [ADT]) – a further improvement was suggested within the field of action 1 for cervical cancer screening. Together with the organised invitation system it should be considered whether the integration of additional strategies, such as a nationwide HPV vaccination, or the integration of additional diagnostic procedures, such as, e.g., HPV diagnostics, could be included as components of such screening or, respectively, prevention strategies.
In the absence of S3 guidelines on cervical cancer in 2008, the control group had to focus on the European guidelines. At the same time, however, to avoid the need to adapt these guidelines that were not appropriate for the German health-care system and were not sufficiently evidence based, but instead to establish a corresponding independent guideline with a high evidence level and a high scientific quality, the oncological guideline program of the DKG, DKH and Committee of the Medical and Scientific Specialist Societies (Arbeitsgemeinschaft Medizinisch Wissenschaftlicher Fachgesellschaften [AWMF]) approved two guidelines:
S3 Guideline on the Prevention of Cervical Cancer (AWMF-Nr. 015-027OL),
S3 Guideline on the Diagnosis, Therapy and Follow-up of Patients with Cervical Cancer (AWMF-Nr. 032-033OL).
The latter will be completed in September 2014 and the former probably in the spring of 2015. At the same time the S3 guideline on HPV-associated neoplasms and preventative vaccinations will be revised so that at the beginning of 2015 the corresponding, high-value, evidence-based S3 guidelines on the primary and secondary prevention of cervical cancer will be available for women patients. On the basis of these guidelines the quality indicators for quality assurance that were established in the course of benchmark projects or, respectively, the certification systems will be available for use.
In October 2008, the gynaecological cancer centres were implemented in Germany according to the certification systems of the DKG and the Germany Society for Gynaecology and Obstetrics (Deutsche Gesellschaft für Gynäkologie und Geburtshilfe e. V. [DGGG]). As of 30. 06. 2014, a total of 107 certified centres have been certified in 109 locations.
Patient access to the certified gynaecological cancer centres at present is solely by direct referral in the absence of a systematic longitudinal health-care chain like those existing, e.g., in the course of screening for other cancers. In the screening for breast cancer the implementation of the mammography screening, the establishment of assessment conferences in the presence of the physician responsible for the programme or, respectively, the surgeon who will take on the further treatment and the certified breast centre constitutes a health-care chain of certifying structures. Similar structures should also be established for the two cancer entities cervical cancer and colon cancer. This has been suggested in the field of action 1, target 2 of the national cancer plan. The foundations for such a structure within the framework of care for female patients with genital cancer are appropriate diagnostic facilities that can carry out the guideline-conform clarification (gynaecological dysplasia consulting practice or, respectively, gynaecological dysplasia units) after nationwide screening (Fig. 1).
Fig. 1.

Concept for Cervical Cancer Screening.
This longitudinal structure for a uniform certified management with appropriate long-term documentation of both high-grade precursors as well as the cancers does not exist in Germany at present. The current certification of gynaecological dysplasia units and consulting practices is carried out by the Working Group of Cervical Pathology and Colposcopy (Arbeitsgemeinschaft Zervixpathologie & Kolposkopie [AG-CPC]).
Previous Certification Structures of Gynaecological Dysplasia and Current Further Training Structures of AG-CPC
History
In 2005 the AG-CPC under its then president Prof. J. Heinrich inaugurated a system for further training in colposcopy and for certification of facilities in the field of clarification of conspicuous findings of the cervix, vagina and vulva. Previously there had been an extensive and long-standing discussion on the structure and contents of the course system to be offered (basic course, advanced course, diploma in colposcopy).
On the basis of the minimum requirements for facilities performing colposcopy demanded by the European Society for Colposcopy (EFC), the corresponding certification structures were created (dysplasia consulting practices, dysplasia centres).
In 2007 the directors of AG-CPC appointed a certification commission. This finalised and unified the criteria for certification of dysplasia consulting practices and dysplasia centres as well as the corresponding colposcopy courses.
The aim was and still is to improve the supply of qualified clarification structures as well as the recognition of those interested in colposcopy. This made it possible for them to present their work to the outside world. Management of and therapy for remarkable findings in the course of cancer screening of the female genital organs are becoming more work-intensive and differentiated with the patients more forcefully demanding a greater say in the processes. These positive results of the public discussion about screening strategies in general and of the cervix in particular demand specialist knowledge, time and a responsible utilisation of material resources. Thus, diplomas and certification of the continuation of specialist training effectively go beyond that formally required by the regulations. Conversely, a corresponding proven and quality documented ability should be recognised by the health insurances. This demand has been placed but can only be realised by means of demonstrated quality and necessity. Colposcopy diplomas and certification of facilities should provide the foundation for this.
Course system of AG-CPC
In 2011 the professional association of gynaecologists and the AG-CPC harmonised their concepts for further training in colposcopy. This involved a common approach in the performance of basic courses leading towards the colposcopy diploma and recognition of the certification system of the AG-CPC.
Basic courses can be offered not only as first courses for beginners but also as advanced or refresher courses. The aim is to differentiate between normal and remarkable colposcopy findings. The minimum course duration is 8 hours. Course leaders must possess the colposcopy diploma, consultants in dysplasia are preferred.
The advanced course carries an appreciably higher scientific standard than the basic course. The aim is to acquire the fundamental ability to head a dysplasia consultancy practice. The minimum duration here is 16 hours. At least 6 months must pass between participation in a basic course and participation in an advanced course. Course teachers must be the head of an AG-CPC certified dysplasia consultancy. Covered topics must in general take current scientific knowledge into consideration which differentiates them from the requirements of the basic courses.
The examination for the colposcopy diploma is linked to proof of participation in at least one basic course and one advanced course, whereby the advanced course must always be subsequent to the basic course. The diploma is valid in Germany and other countries that have specifically declared an interest in this diploma (at present Austria). It does not correspond to the European colposcopy diploma but has been presented to the EU for approval.
From todayʼs perspective it can be stated that the AG-CPC concept has proved its value. In 2008 12 basic courses and 3 advanced course were held in Germany. In 2013 there were 28 and 9 courses, respectively. Up to 16. 05. 2014 1097 colposcopy diplomas have been awarded (from 1506 examinations – failure rate 27.16 %).
Previous certification structures in gynaecological dysplasia
The previous dysplasia centres of AG-CPC differ from dysplasia consultancy practices by their higher number of examined cases, therapy options, additional scientific reputations and training as well as a benchmarking. This structure is supported by Austria. Altogether 127 dysplasia consulting practices and 9 dysplasia centres have been certified.
With the implementation of gynaecological cancer centres in Germany the health-care structures were again scrutinised. In this context the possibility of a second clarification structure besides that established and offered by AG-CPC arose. At the same time it could not be clearly envisaged how the specifically German medical specialties should be incorporated in the proposed health-care structures. Both problems were recognised by all responsible persons in the various organisations; and the merger took place accordingly. With the now presented concept of a joint certification system a harmonisation of the two problem situations has been realised.
Between screening for cervical cancer (general practitioner field) and, if necessary a need for oncological therapy (hospital field), the diagnostic field (dysplasia consultancies/dysplasia units) is in demand, this is principally in line with the AG-CPC concept and falls into the general practitioner or clinical sectors. This procedure strengthens the quality of oncological care (cooperation of the diagnostic unit with a gynaecological cancer centre) and the consultancy practitioner who, within the framework of a qualified follow-up care after the patientʼs cancer screening, is explicitly incorporated in the concept. Thus the often raised criticism of mammography screening concerning a separation from the practicing gynaecological care field does not apply.
In summary it can be concluded that this health-care structure is exclusively provided for the field of specialists in gynaecology and their qualification. The qualification can be achieved in all fields. It strengthens all sectors of management for the afflicted patients (cooperation) and as a final objective raises the quality of treatment (avoiding over therapy, preventing under therapy).
The Certification System of the German Cancer Society (Deutsche Krebsgesellschaft e. V.)
The current certification system of the German Cancer Society (Deutsche Krebsgesellschaft e. V. [DKG]) exists since 2003 and on the basis of the national cancer plan follows the aim to establish certified networks which, from the view point of the patient, encompass the entire health-care chain (Fig. 2) 7. The interdisciplinary, interprofessional and above all the cross-sectorially working treatment partners are jointly certified and present their results in annual audits. Together with the auditors, specialists working in oncology with a special training in the performance of audit procedures, these results are analysed. In possibly necessary cases, i.e., of remarkable findings remaining after the analysis, improvement measures will be defined and their efficacy will be checked in the subsequent audit. In this way together with the certification system an effectively working quality assurance and improvement instrument in the sense of a classical plan-do-check-act cycle will be implemented in clinical routine.
Fig. 2.

Certified gynaecological cancer centres and dysplasia units/consultancy practices.
Nationwide and encompassing all tumours, 914 centres have been designated by the DKG, among them are 107 gynaecological cancer centres 6. The certification system for gynaecological cancer centres has been in operation since 2008 and exhibits over the course of time a continuous development of the number of certified centres (Fig. 3, Table 1). In the 107 gynaecological cancer centres, 9746 female patients with the primary diagnosis of a genital cancer have been treated. This corresponds to 39.4 % of the nationwide incidence from the field of gynaecological oncology (cervical cancer, endometrial cancer, ovarian cancer, vulvar cancer). A detailed evaluation in 2013 revealed that 32.3 % of the female patients with the primary diagnosis of cervical cancer were treated in the centres 1. Through integration of the gynaecological dysplasia consultancy practices and dysplasia units in the certification system of the German Cancer Society (Deutsche Krebsgesellschaft e. V.) the professional societies have also succeeded in including the elementary field of screening in the quality assurance chain in the sense of the patientsʼ best interest.
Fig. 3.
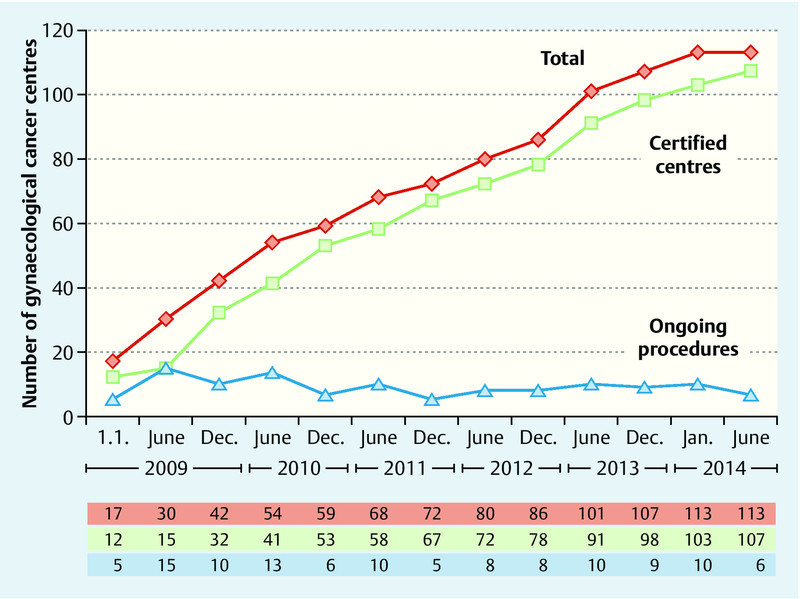
Development of the certification system for gynaecological cancer centres (as of 30. 06. 2014).
Table 1 Development of the certification system for gynaecological cancer centres and further certification system of the German Cancer Society (Deutsche Krebsgesellschaft e. V.) (as of 30. 06. 2014).
| Organ cancer centre | Module | Oncological centre | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Breast | Gastric | Gyn. | Skin | Lungs | Prostate | Head and neck tumours | Neuro.-tumours | Pancreas | ||
| 1 = GEKID data for 2010; 2 = limited to malignant melanoma; 3 = head and neck tumors, new malignant neoplasms of the mouth and throat C00–C14, larynx C32 | ||||||||||
| Current first certification | 4 | 15 | 6 | 2 | 1 | 4 | 3 | 3 | 9 | 8 |
| Certified centres | 219 | 259 | 107 | 42 | 37 | 93 | 22 | 13 | 57 | 65 |
| Certified locations | 274 | 268 | 109 | 42 | 42 | 94 | 24 | 14 | 58 | 75 |
| Primary cases altogether | 51 813 | 24 576 | 9 746 | 9 439 | 14 333 | 20 492 | 3 686 | 2 715 | 2 421 | – |
| Primary cases per centre | 237 | 95 | 91 | 225 | 387 | 220 | 168 | 209 | 43 | – |
| Primary cases per location | 189 | 92 | 89 | 225 | 341 | 218 | 154 | 194 | 42 | – |
| Newly diagnosed cancers 1 | 69 270 | 62 956 | 23 748 | 18 917 2 | 48 986 | 64 467 | 16 820 3 | – | 14 949 | – |
| Overall share 1 | 72.9 % | 38.5 % | 39.4 % | 47.9 % | 28.4 % | 31.0 % | 20.0 % | – | 15.8 % | – |
| Locations abroad | 8 | 4 | 5 | 2 | 2 | 3 | 1 | 1 | 2 | 2 |
Certification system for gynaecological dysplasia
Based on the vote of the certification commission for gynaecological cancer centres and under the chairmanship of the DKG, the Working Group for Gynaecological Oncology (Arbeitsgemeinschaft Gynäkologische Onkologie e. V. [AGO]), the AG-CPC and the DGGG, a certification system for gynaecological dysplasia has now been created. The work of these health-care structures was focused not only on anatomic structures of the uterine cervix but also on the vaginal entrance and the adjacent anatomic structures of the labia majora and labia minora. Both types of cancer, that is vulvar and cervical cancer, belong to the same histological type and to a large part have the same aetiology. Thus is it reasonable to focus the efforts of screening not solely on the uterine cervix and its precursors.
The certification of gynaecological dysplasia is based on the fulfilment of medical requirements and characteristics that are described in the framework of the questionnaire on gynaecological dysplasia and on a specialist on-site audit in which the structures and processes are considered 8.
As a general principle a distinction is made between the certification of a gynaecological dysplasia consultancy practice, which is related to an individual, and a gynaecological dysplasia unit, which is related both to personnel and the facilities, in order to integrate both outpatient as well as inpatient health-care aspects in the certification system.
The requirements differ considerably between the two structures and are described in more detail below. The two forms have in common that a cooperation with a gynaecological cancer centre certified by the DKG must be in operation when the consultancy or, respectively, unit is not itself part of a gynaecological cancer centre. Through this cooperation on the one hand the further interdisciplinary therapeutic planning for the patient with the diagnosis of an invasive cancer in the course of a tumour board is assured and on the other hand an exchange of experience between the structures takes place.
The questionnaire on gynaecological dysplasia consists of three chapters: basic data with a description of the medical expertise (chapter A), the individual requirements in detail (chapter B) and also the characteristics with mention of the required values (chapter C).
The specialist for gynaecology and obstetrics named by the facility must possess a colposcopy diploma from the AG-CPC, in the dysplasia units he or she in addition must have the specialist designation for gynaecological oncology or if necessary a corresponding cooperation must be in operation.
In analogy to the further requirements catalogue of the certification system of the DKG, qualitative and quantitative minimum numbers, for example, the number of documented differential colposcopies and that of histologically confirmed intraepithelial neoplasms, are required. For dysplasia units there is also a minimum requirement for the number of documented excisions (Table 2). Furthermore, the questionnaire also contains a summary of the requirements for patient information, the guidelines employed, further and continuing training, interdisciplinary work in tumour boards, contents or, respectively, procedural descriptions of the consultations and participation in clinical trials.
Table 2 Requirements of the questionnaire on gynaecological dysplasia (excerpt).
Number of documented differential colposcopies with abnormal findings in the cervix, vagina and vulva per year
gynaecological dysplasia consultancies
|
Number of documented and histologically confirmed intraepithelial neoplasms or invasive gynaecological dysplasias
consultancy
|
Number of documented excisions (= therapeutic intervention in the sense of the RIO-classification 2011; excl. biopsies) per year
gynaecological dysplasia unit
|
Quality indicators and interface to European system
Central components of the questionnaire are quality indicators or, respectively, characteristics that can be used as specific and measurable elements for the evaluation of treatment quality 3.
In contrast to the other requirements of the questionnaire, the implementation of which is presented as free text by the certified units, the quality indicators provide with their number and characteristic definitions an unambiguous and thus evaluable result (Table 3). The results of the quality indicators are analysed annually and give a transparent overview of the quality of treatment in the certified units and consultancies. The evaluations show the health-care providers the development of their own results and processes over the course of time, but they can also be considered in a cross-sectional comparison with the results of other certified units per treatment year. In this way the health-care providers have a very good instrument available with which, in the course of certification processes with the auditors, as well as with their own colleagues, they can reflect on the structures and processes and if necessary initiate measures or restructuring procedures. The quality indicators encompass the fields of tumour boards and quality of the gynaecological indications and treatments or, respectively, therapeutic performance.
Table 3 Quality indicators in the questionnaire on gynaecological dysplasia.
| No. | numerator | denominator | nominal value | |
|---|---|---|---|---|
| 1 | consultancy/unit presentation tumour board | number of presented patients with an invasive cancer in the TB of the gynaecological cancer centre | all patients with an invasive cancer | ≥ 90 % |
| 2 | consultancy participation in interdisciplinary tumour boards | number of participations in TB of the gynaecological centre | – | ≥ 4 part./year |
| unit participation in interdisciplinary tumour boards | number of participations in TB of the gynaecological centre | – | ≥ 8 part./year | |
| 3 | unit performance of differential colposcopy | number of patients with an excision in whom a preoperative differential colposcopy was undertaken | all patients in whom an excision was performed | ≥ 95 % |
| 4 | unit remarkable findings on excision | number of patients with excisions and histology leading to ≥ CIN 2 | all patients in whom an excision was performed | ≥ 85 % |
| 5 | unit details of findings reports | number of patients with excision and comprehensive written histological evaluation of the excision (= type and size of all lesions (not metric), vertical and horizontal extension of invasive lesions, resection margins, distance of lesion to endocervical margin in mm) | all patients in whom an excision was performed | ≥ 95 % |
| 6 | unit proportion of R0 resections in CIN III | number of patients with R0 resection in histological finding in CIN III | all patients with excision and histological finding in CIN III | ≥ 80 % |
| 7 | unit follow-up after excision | number of patients with recommendation for single follow-up 6–12 months after excision | all patients in whom an excision was performed | ≥ 90 % |
| 8 | unit proportion of knife conisations in excisions | number of patients with knife conisation | all patients in whom an excision was performed | < 10 % |
| 9 | consultancy/unit documentation (at least as sketches) of visualisation of squamous cell-columnar epithelium border | number of patients with colposcopy in whom the squamous cell-columnar epithelium border was documented (at least as sketches) | all patients with colposcopy | ≥ 85 % |
The quality indicators (characteristics) are oriented on the internationally used quality indicators of EFC. As a founding member of the EFC the AG-CPC has worked continuously on the European minimum requirements for colposcopy facilities 2. These are based on a representative survey among the EFC member states and are regularly evaluated. This was last done in February 2014.
Accordingly the requirements and characteristics in the questionnaire are taken into consideration in the quality indicators of the EFC.
Currently the EFC is initiating a certification procedure for course systems – firstly for the basic courses. Approvements for the training programmes will follow. The AG-CPC has already submitted its course system for certification.
The Concrete Route to Certification
In contrast to the dysplasia consultancies, for which the conformity evaluation is based on the documentation control, the certification of dysplasia units calls for an on-site auditing.
The auditing of dysplasia units follows a defined scheme that is similar to that for organ cancer centres (Fig. 4).
Fig. 4.
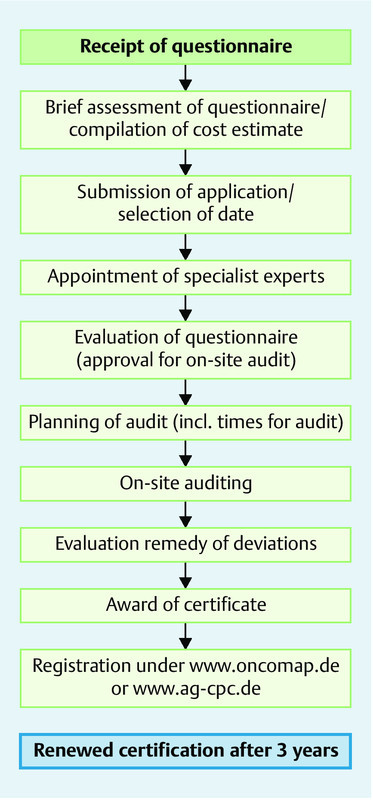
Procedure for auditing dysplasia units.
For the application as a dysplasia unit it is necessary to submit at least the first two pages of the questionnaire with details of the cooperation with a DKG certified gynaecological cancer centre, the medical expertise of the last calendar year as well as target audit date by OnkoZert 8.
After receipt of the completely filled out questionnaire, OnkoZert undertakes a short evaluation (i.e., check for completeness, fundamental certifiability). When the questionnaire is adequately prepared the dysplasia unit receives from OnkoZert a cost estimation in which the costs for the certification are presented. In parallel OnkoZert selects the specialist experts by means of a tendering procedure. The completely filled out questionnaire (with details to B – requirements or, respectively, C – quality indicators/characteristics) must be submitted to OnkoZert at least 4 weeks before the planned audit date. Prior to the audit the designated experts conduct an evaluation of the contents of the questionnaire. Approval for the audit depends on a positive result of this evaluation. Conclusions and advice from the experts are to be analysed with regard to any need for action by the dysplasia unit before the audit date.
The on-site audit takes up about 4 to 5 hours. Any deviations detected during controls of the documents will be considered and assessed during the on-site auditing. Beside the general structure of the gynaecological dysplasia unit and inspection of the premises with consideration of the procedures and interfaces with the respective descriptions of methods, a focus is placed on the interdisciplinary tumour boards, trial management, patient information, further and continuing training and follow-up.
The audit can also be carried out as a joint procedure in the case of an in parallel existing gynaecological cancer centre.
In the course of the final meeting there will be direct feedback to the dysplasia unit – beside a summary of the current situation, possibilities for potential improvements will be presented in the form of advice. Unlike the other certifications by the DKG in which the expert auditor recommends that the certificate be awarded and a certificate granting committee evaluates the situation on the basis of the documentation before making its decision, the expert auditor can award the certificate to the dysplasia unit directly during the final meeting when no deviations have arisen during the course of the audit. After the on-site auditing the expert summarises the audit findings in the last part of the questionnaire that is specifically provided for this final report.
If deviations were expressed in the audit, they must be remedied within 3 months after the audit so that the certificate can then be awarded. In the case of general fulfilment of the requirements but still with a potential for improvement, the certificate is awarded for a limited period (18 months) and after 1 year it will be decided if further documentation or an on-site auditing is required.
The certified dysplasia units with valid certificates will be publically announced on the homepage of the AG-CPC and under www.oncomap.de 8, 9.
For retention of the certificate, the dysplasia units are required to annually submit their characteristics to OnkoZert. A renewed on-site auditing will take place after 3 years.
Status and Perspectives
After the DKG, AGO, AG-CPC and DGGG had prepared the questionnaire for the certification system for dysplasia units, initial pilot certifications were undertaken to check the requirements in real-life situations. For this, the gynaecological dysplasia unit in the womenʼs hospital of Erlangen University, the dysplasia centre in the womenʼs hospital of Jena University and the dysplasia unit of the womenʼs hospital of the Heinrich-Heine University Düsseldorf were approached. The weak points in the questionnaire discovered during audits were discussed in telephone conferences among the participating professional societies and a revised version of the questionnaire was prepared.
Subsequently, on May 9, 2014 the audit experts for the certification of dysplasia units took part in a training course in which the background and the concrete procedures were presented to the future auditors. Besides the training course and proven possession of the AC-CPCʼs colposcopy diploma, the auditors had to attend an on-site audit. As a result, a pool of trained expert auditors with a high state of expertise is now available for future certification procedures.
In addition to the certification of further dysplasia units, the certification of dysplasia consultancies is also currently underway so that in the near future a nationwide supply of certified health-care structures will be realised.
Footnotes
Conflict of Interest J. Quaas: none M. W. Beckmann: none S. Wesselmann: works for the DKG e. V. M. P. Lux: is auditor for the DKG e. V. A. Bischofberger: works for Onkozert A. Kämmerle: works for Onkozert
Supporting Information
German supporting information for this article
References
- 1.Deutsche Krebsgesellschaft e.V. Jahresbericht der Gynäkologischen Krebszentren (in press). 2014Online:http://www.krebsgesellschaft.delast access: 10.07.2014
- 2.European Federation for Colposcopy (EFC) Quality indicators, core competencies, criteria for approvals for basic coursesOnline:http://www.efc.cxlast access: February 2014
- 3.Mainz J. Defining and classifying clinical indicators for quality improvement. Int J Qual Health Care. 2003;15:523–530. doi: 10.1093/intqhc/mzg081. [DOI] [PubMed] [Google Scholar]
- 4.Qualitätssicherung Zytologie Bayern 2011, veröffentlicht 2013
- 5.Starker A, Saß A C. Inanspruchnahme von Krebsfrüherkennungsuntersuchungen. Ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1) Bundesgesundheitsblatt. 2013;56:858–867. doi: 10.1007/s00103-012-1655-4. [DOI] [PubMed] [Google Scholar]
- 6.Suchportal der zertifizierten ZentrenOnline:http://www.oncomap.de/index.phplast access: 09.07.2014
- 7.Wesselmann S, Beckmann M W, Winter A. The concept of the certification system of the German Cancer Society and its impact on gynecological cancer care. Arch Gynecol Obstet. 2014;289:7–12. doi: 10.1007/s00404-013-3084-5. [DOI] [PubMed] [Google Scholar]
- 8.Online:http://www.onkozert.delast access: 23.07.2014
- 9.Online:http://www.ag-cpc.delast access: 29.07.2014
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
German supporting information for this article