

Abstract
Background:
Medial patellofemoral ligament (MPFL) is one of the major static medial stabilising structures of the patella. MPFL is most often damaged in patients with patellar instability. Reconstruction of MPFL is becoming a common surgical procedure in treating patellar instability. We hypothesised that MPFL reconstruction was adequate to treat patients with patellar instability if the tibial tubercle and the centre of the trochlear groove (TT-TG) value was less than 20 mm and without a dysplastic trochlea.
Materials and Methods:
30 patients matching our inclusion criteria and operated between April 2009 and May 2011 were included in the study. MPFL reconstruction was performed using gracilis tendon fixed with endobutton on the patellar side and bio absorbable interference screw or staple on the femoral side. Patients were followed up with subjective criteria, Kujala score and Lysholm score.
Results:
The mean duration of followup was 25 months (range 14-38 months). The mean preoperative Kujala score was 47.5 and Lysholm score was 44.7. The mean postoperative Kujala score was 87 and Lysholm score was 88.06. None of the patients had redislocation.
Conclusion:
MPFL reconstruction using gracilis tendon gives excellent results in patients with patellar instability with no redislocations. Some patients may have persistence of apprehension.
Keywords: Gracilis tendon, Kujala score, medial patellofemoral ligament, patellar instability
MeSH terms: Tendon transfer, ligaments, patellar dislocation, joint instability
INTRODUCTION
Patellofemoral problems form a large part of pathologies affecting the knee. Patellofemoral instability mostly affects the adolescent age group.1,2
Patella is held in position by static and dynamic restraints. The trochlear groove (TG) formed by the two condyles is the major static restraint. The medial soft tissue structures resisting the lateral forces on the patella have been divided into three layers by Warren and Marshall.3 The dynamic stabilizers are the muscles around the knee, the vastus medialis obliquus (VMO) being the most important muscle. The first layer is formed by the deep fascia investing the sartorious muscle. The second layer consists of the medial patellofemoral ligament (MPFL) and the superficial layer of the medial collateral ligament. The third layer is formed by the joint capsule and the deep layer of the medial collateral ligament. The second and third layers are separated by a thin layer of presynovial adipose tissue.
The medial static stabilizers are formed by MPFL, medial patellotibial ligament, medial patellomeniscal ligament.4 This triangular arrangement prevents lateral and superior translations of patella. The MPFL is attached to the medial femoral condyle 10 mm proximal and 2 mm posterior to the medial epicondyle, it is approximately 2 mm anterior and 4 mm distal to adductor tubercle, which is easily palpable.5 The patellar attachment is about 10 mm from the superior pole of patella almost at the upper and middle-third junctions. Biomechanical testing has shown that MPFL provides about 53% restraint against lateral forces on patella.6 The MPFL and medial patellomeniscal ligament together provide about 75% of medial resisting force.7
Surgical techniques to treat patellofemoral instability have been advocated as early as in 1959 and about 137 procedures have been described. Reconstruction of MPFL by various techniques is slowly gaining popularity in treating patients with patellar instability as it is the most commonly injured medial structure in a patellar dislocation.8 In this study we hypothesised that MPFL reconstruction was adequate to treat patients with patellar instability if the tibial tubercle and the centre of the trochlear groove (TT-TG) value was less than 20 mm and without a dysplastic trochlea.
MATERIALS AND METHODS
30 patients who had undergone MPFL reconstruction for patellar instability between April 2009 and May 2011 by the same technique and by the same surgeon were included in this prospective study. All patients included in the study had traumatic patellar dislocation followed by instability and was characterized by apprehension and reduced activity due to the fear of dislocation. They had a Beighton score of less than 6 and tibial tuberosity (TT) - TG distance of less than 20 and a minimum of two episodes of patellar dislocation for inclusion in the study. Patients with ligamentous laxity, TT - TG distance more than 20 mm and shallow trochlea were excluded from the study. Preoperative knee radiograph anteroposterior, lateral and skyline views were done. Preoperatively magnetic resonance imaging was done in all patients to confirm MPFL tear and rule out any associated osteochondral or other intraarticular pathologies. Patients were regularly followed up and were called for reassessment between May and August 2012.
Operative procedure
Diagnostic arthroscopy was performed and any intraarticular pathology (cartilage injury) was addressed. The gracilis tendon was used in all patients. Gracilis tendon was harvested through a 2-3 cm long incision placed 1 cm medial and below the TT. The sartorius fascia was identified and split. The gracilis tendon being tubular was easily palpable. We used a closed tendon stripper to strip the gracilis tendon once it was isolated along with its periosteal insertion. The tendon was then prepared. As the length between the femoral entry site and medial edge of patella was 6-7 cm for double stranded graft, a minimum of 16 cm length of tendon is required.9 A 3 cm incision was made over the medial femoral condyle centered over adductor tubercle and the tissues separated in layers. A 2 cm incision was made over the medial aspect of patella and the periosteum and bone are exposed. The plane between layers two and three containing presynovial fat was identified and separated. A path was created by blunt dissection between the medial aspect of patella and the femoral condylar incision. A guide wire was used to mark the entry point at the junction of upper 1/3 and lower 2/3 of patella, centered on the patella anteroposteriorly. An anterior cruciate ligament jig was used to pass the guide wire such that it exits laterally at the center of patella anteroposteriorly and the junction of upper 1/3rd and lower 2/3rd [Figure 1]. The position of the guide wire was checked under an image intensification. A 4.5 mm tunnel was made using a cannulated drill bit over the guide wire. A tunnel 20 mm in length was made of size corresponding to the graft diameter. A beath pin was passed into the lateral side of patella and graft along with the endobutton was passed and the button flipped. The graft was then passed into the femoral incision site through the plane previously created between layers 2 and 3. A guide wire was passed into femur under image guidance in the true lateral view, about 2-3 mm proximal to the intersection of the posterior end of the Blumensaat line and an imaginary line extending from the posterior margin of femur, this site marked the femoral insertion of MPFL [Figure 2].10 MPFL is not a true isometric structure. A 20-25 mm tunnel corresponding to the graft diameter was drilled over the guide wire and the graft was tightened by beath pin pull through sutures from the lateral aspect of femur and fixed with bio absorbable screw with the knee in 45° of flexion to avoid overtightening of the graft.11 In patients with cost constraint a staple was used. In patients with associated Grade III-IV chondral lesions, microfracture chondroplasty was done and in those with Grade I-II lesion debridement was done. The patellar tracking was reassessed by taking the knee through a full range of motion (ROM) and the wound closed in layers. No drain was used. Compression dressing was applied.
Figure 1.
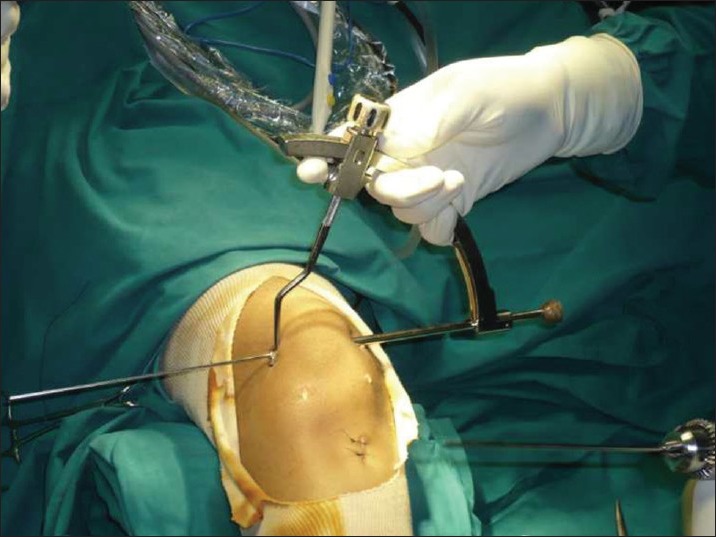
Peroperative clinical photograph showing anterior cruciate ligament jig used for patellar tunnel
Figure 2.
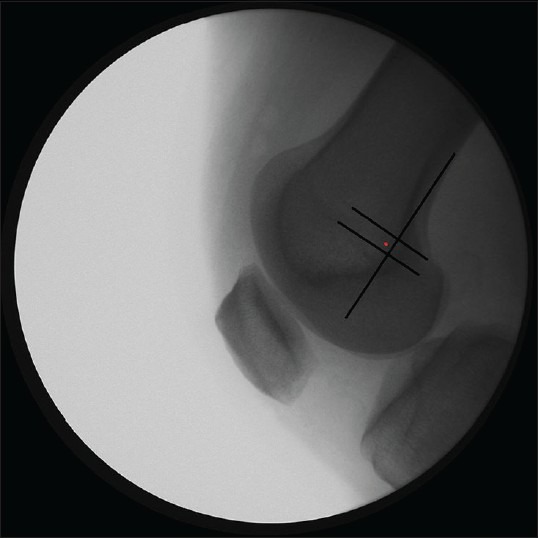
A fluoroscopic view showing C-arm landmark for femoral tunnel
Rehabilitation
The knee was supported with a long leg knee brace for 3 weeks. Partial weight bearing was started on day one and continued up to 3 weeks. Knee ROM between 0 and 45 was started on the 3rd postoperative day. The knee ROM from 0 to 90° was started from the 3rd postoperative week. At the end of 3 weeks brace was removed and full weight bearing was allowed. Patients were started on sports related activities and unopposed sports training was allowed after 3 months. Patients were slowly allowed to get back to active sports after 6 months.
RESULTS
Patients were reviewed between May and August 2012. The patients’ preoperative and postoperative Kujala and Lysholm scores were recorded. At the time of latest followup, their present Kujala and Lysholm scores were assessed. Patients were examined for tenderness and apprehension.
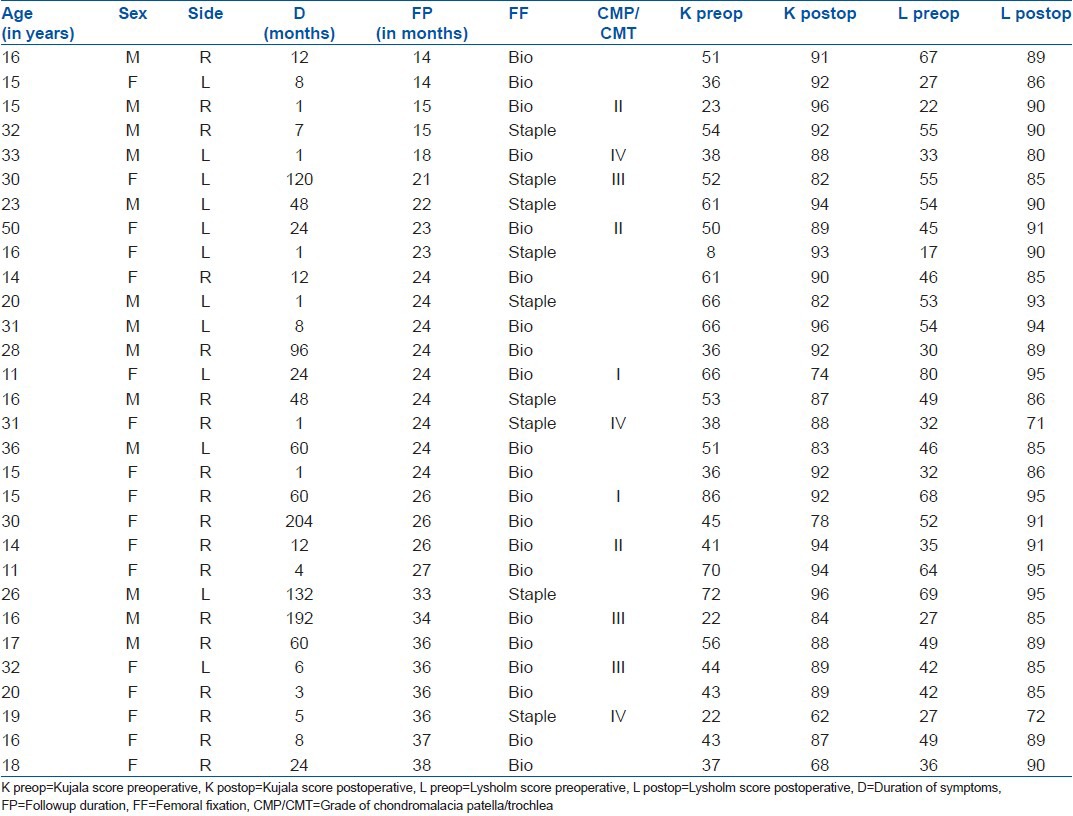
Of the 30 patients included in the study 13 were males and 17 females. The mean followup was 25 months (range 14-38 months). 22 (73%) patients had more than 24 months of followup. The median age of patients included in this study was 18 years (range 11-50 years). All patients had a minimum of two episodes of instability. The median period of instability prior to surgery was 1 year (range 1 month-17 years) [Table 1].
Table 1.
Clinical details of patients
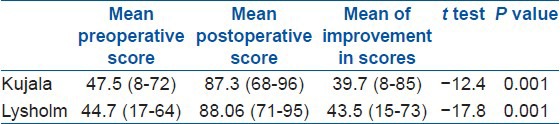
Subjective patient symptoms improved in 26 (86%) of patients. None of the patients had patellar subluxation or dislocation. 3 patients had apprehension regarding instability. The mean postoperative Kujala score was 87.3 (range 68-96) and the mean Lysholm score 88.06 (range 71-95). The mean improvement in Kujala score was 39.7 (range 8-85) and that of Lysholm score was a mean of 43.5 (range 15-73). 6 patients had pain on strenuous activity all of whom had International Cartilage Repair Society Grade III-IV cartilage lesion of the patella or trochlea at the time of the primary procedure. Full range of movement was attained in all patients expect one who had only 100° of flexion. All patients returned to preoperative level of activity. One patient who was a classical dancer returned to preoperative levels of dancing. Statistical analysis was done using paired Students’ t-test. The P value for both the Kujala and Lysholm scores were less 0.001, hence extremely significant [Table 2].
Table 2.
Functional outcome analysis
DISCUSSION
Various surgical procedures have been proposed to treat patellar instability. No surgical technique has been successful in all patient groups. A study by Fithian et al.12 have stated that more than 100 surgical techniques have been described to treat patellar dislocation. No single surgical procedure would be appropriate for all patients and hence a combination might be required.13 Proximal realignment procedures like medial plication and lateral release have been described with various recurrence rates.14,15 Medial transfer of TT as an isolated procedure in patellar instability has produced poor results.16,17,18
In the 1990's the importance of MPFL was identified as the primary medial stabilizing structure.7,19,20 According to Conlan et al. about 53% of medial restraint is provided by MPFL.6 Surgical explorations and radiological studies have shown that MPFL is injured in most cases of patellar dislocations.21,22 Studies have reported that reconstruction or repair of MPFL is important to maintain patellar stability.23,24,25,26,27
Our study contained 30 patients who underwent MPFL reconstruction and were followed up for a minimum of 14 months (with a mean of 25 months), 73% of patients had a followup of greater than 24 months. We did not have any recurrence of dislocation or subluxation, which is similar to other studies.9,28,29,30,31,32 The postoperative Kujala score was 87 (68-96) and the Lysholm score was 88 (78-95). This was similar to other studies.30,31,33,34 Schottle et al.10 reported significant improvement in the kujala scores following MPFL reconstruction comparable to our results. All patients with Grade III-IV cartilage lesion had pain associated with stair climbing and squatting and had lower scores compared with the rest.28 Seven patients had a positive apprehension test of which three had fear of instability during sports activity, but no one had any episode of subluxation or dislocation.
Patellar fracture has been described as a complication, but we did not encounter this in any patient.29 Pain at the femoral fixation (FF) site was present in six of the nine patients in whom staple was used for FF and this warranted removal of implant in all six patients, all of them had total relief from pain after implant removal.
MPFL reconstruction using gracilis graft with endobutton on the patellar side and bio absorbable interference screw on the femoral side has shown very satisfactory short term results. Some patients may have persistence of apprehension.
Footnotes
Source of Support: Nil
Conflict of Interest: None
REFERENCES
- 1.Cofield RH, Bryan RS. Acute dislocation of the patella: Results of conservative treatment. J Trauma. 1977;17:526–31. doi: 10.1097/00005373-197707000-00007. [DOI] [PubMed] [Google Scholar]
- 2.Larsen E, Lauridsen F. Conservative treatment of patellar dislocations. Influence of evident factors on the tendency to redislocation and the therapeutic result. Clin Orthop Relat Res. 1982;171:131–6. [PubMed] [Google Scholar]
- 3.Warren LF, Marshall JL. The supporting structures and layers on the medial side of the knee: An anatomical analysis. J Bone Joint Surg Am. 1979;61:56–62. [PubMed] [Google Scholar]
- 4.LaPrade RF, Engebretsen AH, Ly TV, Johansen S, Wentorf FA, Engebretsen L. The anatomy of the medial part of the knee. J Bone Joint Surg Am. 2007;89:2000–10. doi: 10.2106/JBJS.F.01176. [DOI] [PubMed] [Google Scholar]
- 5.Insall John N, Scott W Norman. 5th ed. Elsevier Churchill Livingstone; 2012. Surgery of the Knee; pp. 680–44. ISBN 978-1-4377-1503-3. [Google Scholar]
- 6.Conlan T, Garth WP, Jr, Lemons JE. Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am. 1993;75:682–93. doi: 10.2106/00004623-199305000-00007. [DOI] [PubMed] [Google Scholar]
- 7.Desio SM, Burks RT, Bachus KN. Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med. 1998;26:59–65. doi: 10.1177/03635465980260012701. [DOI] [PubMed] [Google Scholar]
- 8.Sallay PI, Poggi J, Speer KP, Garrett WE. Acute dislocation of the patella. A correlative pathoanatomic study. Am J Sports Med. 1996;24:52–60. doi: 10.1177/036354659602400110. [DOI] [PubMed] [Google Scholar]
- 9.Muneta T, Sekiya I, Tsuchiya M, Shinomiya K. A technique for reconstruction of the medial patellofemoral ligament. Clin Orthop Relat Res. 1999;359:51–5. doi: 10.1097/00003086-199902000-00016. [DOI] [PubMed] [Google Scholar]
- 10.Schöttle PB, Schmeling A, Rosenstiel N, Weiler A. Radiographic landmarks for femoral tunnel placement in medial patellofemoral ligament reconstruction. Am J Sports Med. 2007;35:801–4. doi: 10.1177/0363546506296415. [DOI] [PubMed] [Google Scholar]
- 11.LeGrand AB, Greis PE, Dobbs RE, Burks RT. MPFL reconstruction. Sports Med Arthrosc. 2007;15:72–7. doi: 10.1097/JSA.0b013e31803bb513. [DOI] [PubMed] [Google Scholar]
- 12.Fithian DC, Nomura E, Arendt E. Anatomy of patellar dislocation. Oper Tech Sports Med. 2001;9:102–111. [Google Scholar]
- 13.Aichroth PM, Al-Duri Z. Dislocation and subluxation of the patella: An overview. In: Aichroth PM, Al-Duri Z, editors. Knee Surgery. London: Martin Dunitz; 1992. pp. 354–79. [Google Scholar]
- 14.Scuderi G, Cuomo F, Scott WN. Lateral release and proximal realignment for patellar subluxation and dislocation. A long term followup. J Bone Joint Surg Am. 1988;70:856–61. [PubMed] [Google Scholar]
- 15.Zeichen J, Lobenhoffer P, Gerich T, Tscherne H, Bosch U. Medium-term results of the operative treatment of recurrent patellar dislocation by Insall proximal realignment. Knee Surg Sports Traumatol Arthrosc. 1999;7:173–6. doi: 10.1007/s001670050143. [DOI] [PubMed] [Google Scholar]
- 16.Brown DE, Alexander AH, Lichtman DM. The Elmslie-Trillat procedure: Evaluation in patellar dislocation and subluxation. Am J Sports Med. 1984;12:104–9. doi: 10.1177/036354658401200203. [DOI] [PubMed] [Google Scholar]
- 17.Conti C, Berruto M, Bianchi M. The Elmslie-Trillat procedure for recurrent subluxation of the patella. One to five year followup. Ital J Orthop Traumatol. 1992;18:341–9. [PubMed] [Google Scholar]
- 18.Ostermeier S, Stukenborg-Colsman C, Hurschler C, Wirth CJ. In vitro investigation of the effect of medial patellofemoral ligament reconstruction and medial tibial tuberosity transfer on lateral patellar stability. Arthroscopy. 2006;22:308–19. doi: 10.1016/j.arthro.2005.09.024. [DOI] [PubMed] [Google Scholar]
- 19.Burks RT, Desio SM, Bachus KN, Tyson L, Springer K. Biomechanical evaluation of lateral patellar dislocations. Am J Knee Surg. 1998;11:24–31. [PubMed] [Google Scholar]
- 20.Nomura E, Fujikawa K, Takeda T, Matsumoto H. Functional anatomy of the medial patellofemoral ligament (in Japanese) Clinical orthopedic surgery. 1993;28:5–10. [Google Scholar]
- 21.Nomura E. Classification of lesions of the medial patello-femoral ligament in patellar dislocation. Int Orthop. 1999;23:260–3. doi: 10.1007/s002640050366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ahmad CS, Stein BE, Matuz D, Henry JH. Immediate surgical repair of the medial patellar stabilizers for acute patellar dislocation. A review of eight cases. Am J Sports Med. 2000;28:804–10. doi: 10.1177/03635465000280060701. [DOI] [PubMed] [Google Scholar]
- 23.Hautamaa PV, Fithian DC, Kaufman KR, Daniel DM, Pohlmeyer AM. Medial soft tissue restraints in lateral patellar instability and repair. Clin Orthop Relat Res. 1998;349:174–82. doi: 10.1097/00003086-199804000-00021. [DOI] [PubMed] [Google Scholar]
- 24.Nomura E, Horiuchi Y, Kihara M. Medial patellofemoral ligament restraint in lateral patellar translation and reconstruction. Knee. 2000;7:121–17. doi: 10.1016/s0968-0160(00)00038-7. [DOI] [PubMed] [Google Scholar]
- 25.Smith TO, Walker J, Russell N. Outcomes of medial patellofemoral ligament reconstruction for patellar instability: A systematic review. Knee Surg Sports Traumatol Arthrosc. 2007;15:1301–14. doi: 10.1007/s00167-007-0390-0. [DOI] [PubMed] [Google Scholar]
- 26.Panagopoulos A, van Niekerk L, Triantafillopoulos IK. MPFL reconstruction for recurrent patella dislocation: A new surgical technique and review of the literature. Int J Sports Med. 2008;29:359–65. doi: 10.1055/s-2007-965360. [DOI] [PubMed] [Google Scholar]
- 27.Christiansen SE, Jacobsen BW, Lund B, Lind M. Reconstruction of the medial patellofemoral ligament with gracilis tendon autograft in transverse patellar drill holes. Arthroscopy. 2008;24:82–7. doi: 10.1016/j.arthro.2007.08.005. [DOI] [PubMed] [Google Scholar]
- 28.Ellera Gomes JL. Medial patellofemoral ligament reconstruction for recurrent dislocation of the patella: A preliminary report. Arthroscopy. 1992;8:335–40. doi: 10.1016/0749-8063(92)90064-i. [DOI] [PubMed] [Google Scholar]
- 29.Ellera Gomes JL, Stigler Marczyk LR, César de César P, Jungblut CF. Medial patellofemoral ligament reconstruction with semitendinosus autograft for chronic patellar instability: A followup study. Arthroscopy. 2004;20:147–51. doi: 10.1016/j.arthro.2003.11.006. [DOI] [PubMed] [Google Scholar]
- 30.Steiner TM, Torga-Spak R, Teitge RA. Medial patellofemoral ligament reconstruction in patients with lateral patellar instability and trochlear dysplasia. Am J Sports Med. 2006;34:1254–61. doi: 10.1177/0363546505285584. [DOI] [PubMed] [Google Scholar]
- 31.Deie M, Ochi M, Sumen Y, Adachi N, Kobayashi K, Yasumoto M. A long term followup study after medial patellofemoral ligament reconstruction using the transferred semitendinosus tendon for patellar dislocation. Knee Surg Sports Traumatol Arthrosc. 2005;13:522–8. doi: 10.1007/s00167-005-0641-x. [DOI] [PubMed] [Google Scholar]
- 32.Cossey AJ, Paterson R. A new technique for reconstructing the medial patellofemoral ligament. Knee. 2005;12:93–8. doi: 10.1016/j.knee.2004.05.003. [DOI] [PubMed] [Google Scholar]
- 33.Drez D, Jr, Edwards TB, Williams CS. Results of medial patellofemoral ligament reconstruction in the treatment of patellar dislocation. Arthroscopy. 2001;17:298–306. doi: 10.1053/jars.2001.21490. [DOI] [PubMed] [Google Scholar]
- 34.Schöttle PB, Fucentese SF, Romero J. Clinical and radiological outcome of medial patellofemoral ligament reconstruction with a semitendinosus autograft for patella instability. Knee Surg Sports Traumatol Arthrosc. 2005;13:516–21. doi: 10.1007/s00167-005-0659-0. [DOI] [PubMed] [Google Scholar]