

Abstract
The use of meditation to improve emotion and attention regulation has a long history in Asia and there are many practitioners in Western countries. Much of the evidence on the effectiveness of meditation is either anecdotal or a comparison of long-term meditators with controls matched in age and health. Recently, it has been possible to establish changes in self-regulation in undergraduate students after only 5 days of meditation practice, allowing randomized trials comparing effects of meditation with other self-control methods such as relaxation training. Early studies took place in Chinese universities; however, similar effects have been obtained with U.S. undergraduates, and with Chinese children aged 4.5 years and older Chinese participants aged 65 years. Studies using neuroimaging techniques have shown that meditation improves activation and connectivity in brain areas related to self-regulation, and these findings may provide an opportunity to examine remediation of mental disorders in a new light.
Keywords: meditation, IBMT, self-regulation, life span
Introduction
Mindfulness-based interventions (MBIs) are composed of several key components, including relaxation, breathing practice, mental imagery, and body–mind awareness.1–5 Although MBIs vary in their methods, quality, and dosage, some have been shown to improve attention, emotion regulation, and social relationships in children and adults.1,4–7 However, several key theoretical and methodological challenges arise in the field.8 As noted in a recent review,9 most research in this area has lacked scientific rigor and has not used the random assignment and active control necessary to attribute causality to the mindfulness intervention. One reason that most studies do not use these designs is the expectation that very long-term training is needed to obtain strong behavioral results. In this paper, we examine one form of mindfulness training for which extensive randomized trials have been conducted using a rigorous control of relaxation training. These studies have provided a possible anatomical basis for the effects of training involving both central and autonomic nervous system changes. These anatomical changes suggest the possibility of an approach to the remediation or prevention of some clinical conditions, including substance abuse, psychopathy, borderline personality disorder, and schizophrenia.
Randomized controlled trials
In 2007, we reported on a version of mindfulness meditation, integrative body–mind training (IBMT), adapted from traditional Chinese medicine.2 The general method for IBMT is briefly described in the next section.
Description of IBMT
IBMT originates from ancient eastern contemplative traditions including traditional Chinese medicine and Zen meditation. This type of meditation does not stress an effort to control thoughts, but instead promotes a state of restful alertness that allows a high degree of awareness and balance of the body, mind, and environment. The meditation state is facilitated through training and trainer–participant interaction.10
IBMT practice is typically conducted in a group setting and includes (1) a presession (approximately 5 min), (2) a practice session (approximately 20 min), and (3) a postsession (approximately 5 min). Each session is led by a qualified IBMT coach who has completed IBMT training and passed associated certification tests, participated actively in the IBMT intervention as part of training, and demonstrated the ability to effectively interact with the trainees. The role and skill of the coach in effectively engaging intervention participants is critical, especially when working with adolescents and children.11 In the presession, the coach reviews instructions for the practice session, interacts with participants, and helps guide them into quietness and a mindful state. In the practice session, participants follow IBMT instructions using a compact disk (CD) that includes background music to help them enter a meditative state. During the practice session, the coach observes facial and body cues to identify participants who are having problems with the method, and provides feedback either promptly or after the session. Practice sessions are intended to help each participant increase the length of time spent in the meditation experience, so that the quality of meditation will improve with each session. In the postsession, the coach facilitates a brief group discussion to help ensure that participants have had positive experiences.2,3,7,12
The rapid acquisition of the meditation state using IBMT allowed us to design a strong test of the effects of training. A sample of 80 Chinese undergraduates were assigned randomly to a meditation group that underwent five 20- to 30-min sessions of IBMT or to a control group that underwent five sessions of relaxation training,2 commonly used in the West as a part of cognitive behavioral therapy. We tested IBMT and control groups before and after training using the Attention Network Test (ANT), which uses a flanker task to introduce conflict and measure the efficiency of the executive network. Precues provide information on when and where the target will be presented to measure alerting and orienting.13
We found a greater improvement in executive attention in the IBMT group than in the control group (Fig. 1). IBMT also produced improvements in self-reported mood state and a reduction in the stress hormone cortisol following a cognitive challenge (mental arithmetic) as measured from saliva samples (Fig. 2A). It also improved immunoreactivity, measured by a salivary assay related to the efficiency of immunoreactivity (secretory immunoglobulin A, sIgA;2 Fig. 2B). The reduction in cortisol levels and improvement in immunoreactivity (sIgA) found with IBMT after 1 week were dependent on repeating the training just before assessment to ensure that subjects would be in the meditative state when tested. Other findings, such as self-reported improvements in mood and efficiency of executive attention as measured by the ANT, were found even without an additional training session.
Figure 1.

Differences in performance on the Attention Network Test (ANT). Shown are mean reaction times after training—mean reaction times before training and after 5 days (1 week of training with IBMT or relaxation). Differences are provided for the alerting (no cue–double cue), orienting (correct location cue–central cue) and executive attention (incongruent–congruent) networks for IBMT (experimental) and relaxation training (control) groups. The higher scores show less efficient resolution of conflict (see Ref. 2).
Figure 2.

Physiological changes before and after stress. (A) Comparison of cortisol concentration between the experimental group (red bars) and control group (gray bars) in three different stages after 5 days of training. *P < 0.05; **P < 0.01. Error bars indicate 1 SEM. More cortisol secretion indicates higher levels of stress. (B) Comparison of sIgA concentration between experimental group (red bars) and control group (purple bars) at three different stages after 5 days of training. **P<0.01. Error bars indicate 1 SEM. Higher immunoreactivity indicates a better response to stress (see Ref. 2).
Continued training
In additional studies in both the United States and China, groups of undergraduate students were randomly assigned to IBMT or relaxation for 1 month (4 weeks, 11 h in total). With this longer period of training, greater changes in aspects of attention were found. On the ANT, both the alerting and executive network were more improved with IBMT than with relaxation training.11 The increased dose of IBMT significantly reduced cortisol and significantly increased immunoreactivity even at baseline before any cognitive challenge (Fig. 3). This suggests that subjects with only 1 month of meditation training were able to resist the stress of everyday life to a greater degree than they were able to before training or following relaxation training.14,15 These studies also showed that our findings in China were consistent with those in U.S. undergraduates.
Figure 3.

Secretory immunoglobulin A (sIgA) and cortisol secretion at baseline (before any specific stress or training). Measurements were taken three times: before any training, following 2 weeks of training, and following 4 weeks of training. After 4 weeks of training, there is significantly reduced cortisol (stress) and increased immune response (sIgA) at baseline (see Ref. 14).
Cultural differences
Our initial studies were conducted with Chinese undergraduates at Dalian University of Technology, and we have now replicated many of these studies with American students at the University of Oregon. While the brain mechanisms, behavior, and physiological outcomes of training were very similar in the two cultures, there were differences in the subject populations. While anecdotal, these differences do have important consequences for conducting future research. For example, it was difficult to get American students to commit themselves to a regular schedule of sessions, particularly for those lasting 1 month. The U.S. students needed more makeup sessions and tended to keep a more irregular schedule than Chinese students who maintained regular schedules and rarely missed sessions. Generally, the training sessions involved five to seven students, and the group setting was preferred by Chinese students, but many U.S. students also wanted individual sessions. The U.S. students also appeared to prefer detailed verbal instructions to achieve the meditative state, whereas Chinese students better followed the intended method into the meditative state. The average age in Chinese and American groups was 20 years old, and the undergraduates shared similar interests such as the use of iPhones, computers, and the Internet. We thought the Chinese students may be more sensitive to meditation given cultural influences but did not find evidence of this.10
It is natural to ask how long the effects of training with IBMT last. To date we have had some difficulty in providing an answer to that question. One of the problems is retaining a full sample of the same U.S. undergraduates to participate again after 6 months or 1 year because they are often too busy, or have changed or left school. However, the issue of improvement with no further training is somewhat less relevant for meditation training than for other forms of intervention. Once having learned the method, it is relatively easy to continue, and the practice can be carried out with little or no expense other than setting aside a half hour per day. Nonetheless, we plan to test the lasting effects in future research.
Mechanisms
Physiological changes
Training in IBMT improved executive attention;2,11 however, unlike other studies used to train attention,16–18 there was no specific effort to have the trainees perform a behavioral task. We have argued that IBMT might work by changing the brain state.4 A change in state refers to a change in the central and autonomic nervous system that does not depend upon performance of any particular task. One part of our argument was based on evidence from heart rate variability showing increased activity in the parasympathetic portion of the autonomic nervous system specific to IBMT practice.3 More specifically, we thought that the calm but focused meditation state might increase the function of the anterior cingulate portion of the executive attention network, a hypothesis that was tested in the study described below. Also indicative of a change of brain state is that meditation may alter the resting state (default state) as measured by functional magnetic resonance imaging (fMRI).8,19,20
Brain changes
A further study3 collected brain imaging (single-photon emission computed tomography, SPECT) data before and after 5 days of training. Activation of the anterior cingulate cortex (ACC) was greater following IBMT than following relaxation training, confirming our hypothesis. Following 1 month of training, the IBMT group showed improved functional connectivity between the ACC and striatum in comparison with the relaxation group. Moreover, parasympathetic function, as measured by heart rate variability, had changed more in the IBMT group than in the controls. Further studies using diffusion tensor imaging revealed that several white matter tracts connecting the ACC to other areas had improved their efficiency as measured by fractional anisotropy derived from diffusion tensor imaging.21 The tracts altered by training are indicated in Figure 4, including the anterior corona radiata, which has previously been shown to be specifically related to the executive attention network.22 These findings show that connectivity related to self-regulation can be altered in adults by meditation training. The results have potential implications for all aspects of self-regulation–related problems or disorders, including clinical or educational applications.
Figure 4.
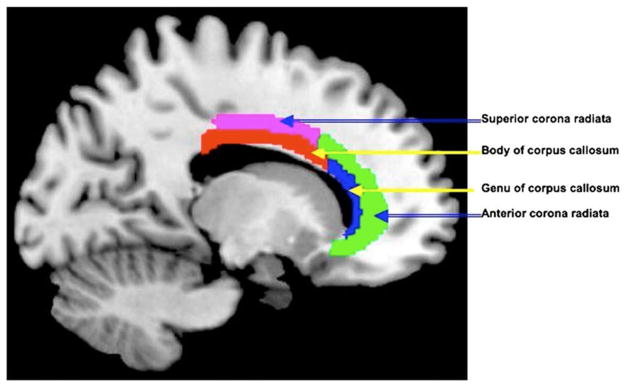
The white matter pathways in which there were greater changes in connectivity (as measured by fractional anisotropy (FA) from diffusion tensor imaging) after 4 weeks of IBMT than after the same period of relaxation training (see Ref. 21).
Older adults and preschool children
Comparing physical and mental training in aging
Previous studies have shown that physical exercise and meditation both lead to increases in physical and mental health.1,23 However, it is unknown whether the two practices share the same underlying mechanisms. In the same local communities, we randomly chose healthy and high-functioning Chinese elders (about 65 years old) from previously developed 10-year IBMT or physical exercise groups. Each group had practiced daily in the local community for an average of 1 hour. The IBMT or exercise instructor in the same community supervised the practice sessions.11 All participants were living independently and were matched in age, sex, education, and health status. At the end of the 10 years of training, we measured brain activity, physiology, and behavior. No sedentary control group was assigned because such a group would be unlikely to maintain good health over a 10-year period so that our data represent only differences between mental and physical training.
In comparison with exercise, we found significantly higher results for IBMT on (1) ratings of quality of life, (2) parasympathetic activity indexed by high-frequency heart rate variability, (3) basal sIgA levels, and (4) basal cortisol levels.11 The IBMT group also showed stronger brain connectivity between the dorsal ACC and the striatum using resting-state fMRI and greater grey matter in the striatum using structural MRI than the exercise group. The exercise group showed lower overall heart rate and greater chest respiratory amplitude than the IBMT group at baseline. Our results suggested that meditation and physical exercise may work in part by different mechanisms, with exercise producing greater physical fitness and meditation producing greater central nervous system changes. These findings suggest that combining physical and mental training may lead to better health and quality of life during aging.
Preschool children
During childhood the ability to resolve conflict is correlated with parental reports of their child’s ability to regulate his or her behavior. These findings have led us to associate the executive network with behavioral self-regulation or self-control.24–26
Previously we had given 4- and 6-year-old children executive attention training using computer programs developed from those used to train monkeys for space experiments. These exercises involved specific practice on attention tasks. Five days of training produced improved networks underlying executive attention17,18 and improved IQ scores. Since our study, a number of other methods have been used to train attention in preschool children. All of these methods have involved what we call attention training, that is the deliberate exercise of particular brain networks related to attention functions.16
It may be thought that preschool children would not be able to be trained in meditation that requires strict adherence to instructions. However, there is evidence for the effectiveness of meditation training in young children.12,27 For example, Chinese 4.5-year-olds were given 10 h of practice with a child version of IBMT in half-hour sessions over a month, in comparison with an active control condition that included classroom activity. This training produced a significant increase in self-regulation as measured by parents’ reports of effortful control in the Children’s Behavior Questionnaire.26 Performance in two Stroop-type tests adapted for children was also significantly improved for the IBMT group in comparison to controls.10 These findings suggest that IBMT can have effects in a range of age groups from preschool-age children to older adults. In the future we plan to apply this program to U.S. children.
Clinical applications
Overall attention and attention-state training are promising methods for clinical application. Attentional difficulties are a frequent symptom of different forms of psychopathology.25 However, without a real understanding of the neural substrates of attention, there has not been a sufficient basis for systematic efforts to remedy attentional problems. This situation has been changed with the application of our understanding of attention networks to pathology. Viewing attention as an organ system with its own functional anatomy carrying out specific attentional functions, and investigating the underlying neural networks, provides a means of classifying disorders that differs from the usual internalizing (e.g., depression) versus externalizing (e.g., conduct disorder) classification applied to such disorders.28
A number of mental disorders seem to involve primarily the executive attention network. These disorders involve a specific difficulty in resolving conflict in the flanker or other conflict-related tasks. Although many disorders also involve other executive functions, such as planning or problem solving, we concentrate on measures of conflict resolution that involve the executive attention network we have been discussing. These disorders include, but are not limited to, substance abuse, psychopathy, borderline personality disorder, and schizophrenia.25 Since we have discussed a method to improve the functioning of executive attention through specific training and meditation, it seems reasonable to test whether training would prove particularly useful for disorders that involve this network. Below, we briefly outline some of the areas where our training methods might be relevant to various disorders.
Substance abuse
Many studies of substance abuse have identified abnormalities in the frontal midline including the ACC and striatum among other areas.29,30 In one example, a recent study using conflict tasks (Stroop) and fMRI showed that, in comparison with a control group, adolescent long-term marijuana abusers showed a deficit in the ability to resolve conflict caused by an inefficient executive network.31 This result could either be the cause or the result of using the drug. In either case, methods that might strengthen the activation and connectivity of the ACC could be useful in the treatment of this disorder.
Psychopathy
Psychopathy involves a failure of empathy for the pain of others when taking actions that are rewarding to the self. Studies suggest that psychopathic behavior also rests upon the kind of attention paid to environmental cues including other people. When cues are deliberately attended to, psychopaths seem to behave similarly to nonpsychopaths, but they do not seem to monitor the environment for those cues if they are not already in the focus of attention.32 According to one imaging study, the ventral ACC was less active in psychopaths when viewing frightening faces than for nonpsychopaths.33 Since attention-state training increases activity in the ventral anterior cingulate, this might be a relevant therapy.
Borderline personality disorder
Borderline personality disorder is characterized by great variability of affect and difficulties in interpersonal relations. We compared borderline patients with controls who were equally high in negative emotionality and low in self-regulation as measured by adult temperament scales.26 It was found that borderline patients had even greater deficits in conflict resolution in the ANT than controls.34
Imaging results showed overgeneralization of responding to negative words in the amygdala, and reduced responding in the anterior cingulate and related midline frontal areas involved in self-regulation, in borderline patients.35 Patients with higher effortful control and better conflict scores on the ANT were also the most likely to show improvements with therapy. Since mindfulness training increases ACC activation, it might improve self-regulation in these patients.
Schizophrenia
In a study using the ANT,36 patients with chronic schizophrenia were compared to a control group matched for age and education. The schizophrenic patients had much longer reaction times in order to resolve conflict than did the controls. They also showed a small orienting deficit of the type that had been reported previously in first-break never-medicated patients.37 An imaging study run on these first-break patients revealed a deficit in activity in the left globus pallidus. The disorder seems to progress from a focal abnormality to one involving a reduction of executive control.38 The pathology involved in schizophrenia in the chronic state appears to be related to the executive network and self-regulation; thus it might also be a candidate for meditation or other executive attention training.
Summary
Mindfulness mediation has proven effective in improving brain functions related to executive attention in normal subjects across the life span. Our studies of IBMT suggest its utility in improving the activity and connectivity of the executive attention network involved in self-regulation. This network can also be improved by exercises that involve its repeated use. The evidence discussed here supports the use of attention training and meditation to improve the lives of children and as a possible treatment of a variety of conditions that may involve a deficit in self-regulation.
Acknowledgments
We thank Rongxiang Tang for assistance with manuscript preparation. The preparation of this paper and the research described here were supported by Grants from the Office of Naval Research, 973 Program 2012CB518200, R21 DA030066, and HD060563.
Footnotes
Conflicts of interest
The authors declare no conflicts of interest.
References
- 1.Lutz A, Slagter HA, Dunne JD, Davidson RJ. Attention regulation and monitoring in meditation. Trends Cogn Sci. 2008;12:163–169. doi: 10.1016/j.tics.2008.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tang YY, Ma Y, Wang J, et al. Short term meditation training improves attention and self-regulation. Proc Natl Acad Sci USA. 2007;104:17152–17156. doi: 10.1073/pnas.0707678104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tang YY, Ma Y, Fan Y, et al. Central and autonomic nervous system interaction is altered by short-term meditation. Proc Natl Acad Sci USA. 2009;106:8865–8870. doi: 10.1073/pnas.0904031106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tang YY, Posner MI. Attention training and attention state training. Trends Cogn Sci. 2009;13:222–227. doi: 10.1016/j.tics.2009.01.009. [DOI] [PubMed] [Google Scholar]
- 5.Tang YY, Rothbart MK, Posner MI. Neural correlates of establishing, maintaining and switching brain states. Trends Cogn Sci. 2012;16:330–337. doi: 10.1016/j.tics.2012.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hölzel BK, Lazar SW, Gard T, et al. How does mindfulness meditation work? Proposing mechanisms of action from a conceptual and neural perspective. Perspect Psychol Sci. 2011;6:537–559. doi: 10.1177/1745691611419671. [DOI] [PubMed] [Google Scholar]
- 7.Tang YY. Mechanism of integrative body-mind training. Neurosci Bull. 2011;27:383–388. doi: 10.1007/s12264-011-1141-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tang YY, Posner MI. Theory and method in mindfulness neuroscience. Soc Cogn Affect Neurosci. 2013;8:118–120. doi: 10.1093/scan/nss112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Greenberg MT, Harris AR. Nurturing mindfulness in children and youth: Current state of research. Child Dev Perspect. 2011;6:161–166. [Google Scholar]
- 10.Tang YY, Lu Q, Fan M, et al. Mechanisms of white matter changes induced by meditation. Proc Natl Acad Sci USA. 2012;109:10570–10574. doi: 10.1073/pnas.1207817109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tang YY. Exploring the Brain, Optimizing the Life. Beijing, China: Science Press; 2009. [Google Scholar]
- 12.Tang YY, Yang L, Leve LD, Harold GT. Improving executive function and its neurobiological mechanisms through a mindfulness-based intervention: advances within the field of developmental neuroscience. Child Dev Perspect. 2012;6:361–366. doi: 10.1111/j.1750-8606.2012.00250.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fan J, McCandliss BD, Sommer T, et al. Testing the efficiency and independence of attentional networks. J Cogn Neurosci. 2002;14:340–347. doi: 10.1162/089892902317361886. [DOI] [PubMed] [Google Scholar]
- 14.Fan Y, Tang YY, Ma Y, Posner MI. Mucosal immunity modulated by integrative meditation in a dose dependent fashion. J Altern Complement Med. 2010;16:151–155. doi: 10.1089/acm.2009.0234. [DOI] [PubMed] [Google Scholar]
- 15.Fan Y, Tang YY, Posner MI. Cortisol level modulated by integrative meditation in a dose-dependent fashion. Stress Health 2013. 2013 May 20; doi: 10.1002/smi.2497. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 16.Diamond A, Lee K. Interventions shown to aid executive function development in children 4 to 12 years old. Science. 2011;333:959–964. doi: 10.1126/science.1204529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rueda MR, Rothbart MK, McCandliss BD, et al. Training, maturation and genetic influences on the development of executive attention. Proc Natl Acad Sci USA. 2005;102:14931–14936. doi: 10.1073/pnas.0506897102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rueda MR, Checa P, Combita LM. Enhanced efficiency of the executive attention network after training in preschool children: immediate and after two month effects. Devel Cogn Neurosci. 2012;2:S192–S204. doi: 10.1016/j.dcn.2011.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Brewer JA, Worhunsky PD, Gray JR, et al. Meditation experience is associated with differences in default mode network activity and connectivity. Proc Natl Acad Sci USA. 2012;108:20254–20259. doi: 10.1073/pnas.1112029108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jang JH, Jung WH, Kang DH, et al. Increased default mode network connectivity associated with meditation. Neurosci Lett. 2011;487:358–362. doi: 10.1016/j.neulet.2010.10.056. [DOI] [PubMed] [Google Scholar]
- 21.Tang YY, Lu Q, Geng X, et al. Short-term mental training induces white-matter changes in the anterior cingulate. Proc Natl Acad Sci USA. 2010;107:16649–16652. doi: 10.1073/pnas.1011043107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Niogi S, McCandliss BD. Individual differences in distinct components of attention are linked to anatomical variations in distinct white matter tracts. Front Neuroanat. 2009;4:2. doi: 10.3389/neuro.05.002.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hillman CH, Erickson KI, Kramer AF. Be smart exercise your heart. Exercise effects on brain and cognition. Nat Rev Neurosci. 2008;9:58–64. doi: 10.1038/nrn2298. [DOI] [PubMed] [Google Scholar]
- 24.Posner MI, Rothbart MK, Sheese BE, Tang YY. The anterior cingulate gyrus and the mechanism of self-regulation. Cogn Affect Behav Neurosci. 2007;7:391–395. doi: 10.3758/cabn.7.4.391. [DOI] [PubMed] [Google Scholar]
- 25.Posner MI. Attention in a Social World. New York: Oxford University Press; 2012. [Google Scholar]
- 26.Rothbart MK. Becoming Who We Are. New York: Guilford; 2011. [Google Scholar]
- 27.Zelazo PD, Lyons KE. The potential benefits of mindfulness training in early childhood: a developmental social cognitive neuroscience perspective. Child Dev Perspect. 2012;6:154–160. [Google Scholar]
- 28.Posner MI, Fan J. Attention as an organ system. In: Pomerantz JR, Crair MC, editors. Topics in Integrative Neuroscience: from Cells to Cognition. Cambridge: Cambridge University Press; 2004. pp. 31–59. [Google Scholar]
- 29.Baler RD, Volkow ND. Drug addiction: the neurobiology of disrupted self-control. Trends Mol Med. 2006;12:559–566. doi: 10.1016/j.molmed.2006.10.005. [DOI] [PubMed] [Google Scholar]
- 30.Feil J, Sheppard D, Fitzgerald PB, et al. Addiction, compulsive drug seeking, and the role of frontostriatal mechanisms in regulating inhibitory control. Neurosci Biobehav Rev. 2010;35:248–275. doi: 10.1016/j.neubiorev.2010.03.001. [DOI] [PubMed] [Google Scholar]
- 31.Abdullaev Y, Posner MI, Nunnally R, Dishion T. Functional MRI evidence for inefficient attentional control in adolescent chronic cannabis abusers. Behav Brain Res. 2010;215:45–57. doi: 10.1016/j.bbr.2010.06.023. [DOI] [PubMed] [Google Scholar]
- 32.Zeier JD, Maxwell JS, Newman JP. Attention moderates the processing of inhibitory information in primary psychopathy. J Abnorm Psychol. 2009;118:554–563. doi: 10.1037/a0016480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Blair RJR, Morris JS, Frith CD, et al. Dissociable neural responses to facial expression of sadness and anger. Brain. 1999;1222:883–893. doi: 10.1093/brain/122.5.883. [DOI] [PubMed] [Google Scholar]
- 34.Posner MI, Rothbart MK, Vizueta N, et al. Attentional mechanisms of borderline personality disorder. Proc Natl Acad Sci USA. 2002;99:16366–16370. doi: 10.1073/pnas.252644699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Silbersweig D, Clarkin JF, Goldstein M, et al. Failure of frontolimbic inhibitory function in the context of negative emotion in borderline personality disorder. Am J Psychiatr. 2007;164:1832–1841. doi: 10.1176/appi.ajp.2007.06010126. [DOI] [PubMed] [Google Scholar]
- 36.Wang KJ, Fan J, Dong Y, et al. Selective impairment of attentional networks of orienting and executive control in schizophrenia. Schizophr Res. 2005;78:235–241. doi: 10.1016/j.schres.2005.01.019. [DOI] [PubMed] [Google Scholar]
- 37.Posner MI, Early TS, Reiman E, et al. Asymmetries in hemispheric control of attention in schizophrenia. Arch Gen Psychiatr. 1988;45:814–821. doi: 10.1001/archpsyc.1988.01800330038004. [DOI] [PubMed] [Google Scholar]
- 38.Early TS, Posner MI, Reiman EM, Raichle ME. Hyperactivity of the left stiato-pallidal projection, Part I: lower level theory. Psychiatr Dev. 1989;2:85–108. [PubMed] [Google Scholar]