

To the editor,
We read with interest the article published in your journal by Zeng et al. (1), reporting a case of infection by the multi-flagellated protozoon Lophomonas blattarum (LB) in an acute exacerbation of chronic obstructive pulmonary disease (COPD) (Figure 1).
Figure 1.
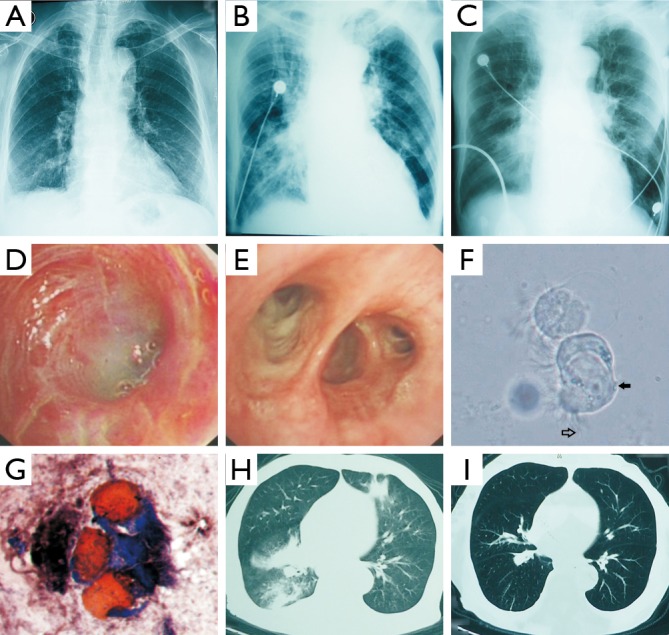
Image, bronchoscopy and smear finding in this case. (A) Chest X-ray showed no signs of any infiltration, masses and lymphadenopathy, at the fifth day from onset; (B) chest X-ray showed bilateral effusion, infiltrated and linear opacities, at the nineth day from onset; (C) chest X-ray showed improvement after tinidazole injection, at the fifteenth day from onset; (D) bronchoscopy showed a lot of purulent sputum, and diffusely swelling and friable mucus on the left lingual bronchus; (E) bronchoscopy showed a lot of purulent sputum, and diffusely swelling and congestion mucus on the right middle bronchus; (F) (×400); (G) (Leifson, ×400): Lophomonas blattarum clustered in direct suction specimen.,  body of Lophomonas blattarum;,
body of Lophomonas blattarum;,  wave flagellates; (H) pulmonary CT scan presented bilateral effusion, infiltrated, at the twenty fifth day from onset; (I) pulmonary CT scan presented improvement and resolved of lesion, 3 months later after discharge.
wave flagellates; (H) pulmonary CT scan presented bilateral effusion, infiltrated, at the twenty fifth day from onset; (I) pulmonary CT scan presented improvement and resolved of lesion, 3 months later after discharge.
On carefully examination of the two of the images provided in the article (Figure 1F,G), we think that on balance this article may have misidentified respiratory ciliated cells for multiflagellated protozoon. Our concerns are based on a set of morphological features that we have developed to differentiate ciliated epithelial cells from flagellated protozoa under the light microscopy (2,3).
We believe that Figure 1F shows a small group of ciliated bronchial cells (similar to a Creola body) with two large nuclei occupying almost the half of the cytoplasm and numerous short, regular and well oriented cilia (rather than true flagella). Similarly, we would argue that Figure 1G probably represents three ciliated bronchial cells, as the cells are columnar in shape, with large reed nuclei located at the basal end and tufts of cilia located at the apical ends of the cells.
Leaving the morphologic considerations aside, it is true that a positive response to the therapy with albendazole is an important point to consider. However, albendazole and other similar drugs such as nitroimidazoles are highly active against gram-negative anaerobic bacteria (4), which can be the causative agent in acute exacerbations of COPD.
The majority of articles reporting clinical cases of LB have been written by Chinese authors but in a lot of them, as it has been pointed out by Mu et al. (5), ciliated bronchial cells may have been erroneously misidentified as multiflagellated protozoa. We are similarly conscious that the misidentification of epithelial ciliated cells as multiflagellated protozoa needs to be considered when respiratory samples are examined under light microscopy (6,7).
In the absence of culture or molecular techniques, strict morphologic criteria need applied during light microscopy.
Acknowledgements
Disclosure: The authors declare no conflict of interest.
References
- 1.Zeng H, Kong X, Chen X, et al. Lophomonas blattarum infection presented as acute exacerbation of chronic obstructive pulmonary disease. J Thorac Dis 2014;6:E73-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Martínez-Girón R, Doganci L.Lophomonas blattarum: a bronchopulmonary pathogen. Acta Cytol 2010;54:1050-1 [PubMed] [Google Scholar]
- 3.Martínez-Girón R. Protozoal infections. In: Barrios R, Haque AK. eds. Parasitic diseases of the lungs. New York: Springer-Verlag, 2013:47-68. [Google Scholar]
- 4.Löfmark S, Edlund C, Nord CE. Metronidazole is still the drug of choice for treatment of anaerobic infections. Clin Infect Dis 2010;50Suppl 1:S16-23 [DOI] [PubMed] [Google Scholar]
- 5.Mu XL, Shang Y, Zheng SY, et al. A study on the differential diagnosis of ciliated epithelial cells from Lophomonas blattarum in bronchoalveolar lavage fluid. Zhonghua Jie He He Hu Xi Za Zhi 2013;36:646-50 [PubMed] [Google Scholar]
- 6.Martínez-Girón R, van Woerden HC, Doganci L. Lophomonas misidentification in bronchoalveolar lavages. Intern Med 2011;50:2721; author reply 2723 [DOI] [PubMed] [Google Scholar]
- 7.Martínez-Girón R, van Woerden HC. Bronchopulmonary lophomoniasis: emerging disease or unsubstantiated legend? Parasit Vectors 2014;7:284. [DOI] [PMC free article] [PubMed] [Google Scholar]