

Abstract
The identification of mastoidal emissary veins is of importance in the neurosurgical practice to diagnose abnormal and normal structures. In the present study, the objectives were to estimate the prevalence rate of mastoidal emissary foramina in the temporal bones of the adult skull and to study their number and morphology. The present study included 48 adult human skulls which were obtained from the gross anatomy laboratory of our institution. The mastoid parts of 96 temporal bones were macroscopically observed for the prevalence, number and morphology of the emissary foramina. It is observed that, the mastoidal emissary foramen was present in 88 temporal bones (91.7%) of our specimens. The foramen was observed single in 60 temporal bones (62.5%), double in 22 bones (22.9%), and triple in 6 temporal bones (6.2%). The mastoidal emissary foramen was absent in 8 (8.3%) temporal bones. The foramen was bilaterally absent in 3 (3.1%) skulls. It was unilaterally absent in 2 (2.1%) skulls and both were on the left side. The mastoidal emissary vein is prevalent in a large number (91.7%) of cases. It was observed that the accessory mastoidal emissary foramina were present in 29.1% of cases. Recognition of the mastoid emissary veins and accessory mastoid emissary veins during the otologic surgery is critical to avoid the significant bleeding. In the neurosurgical practice, the knowledge is important due to variability in the number of mastoidal emissary veins and their connection to the venous sinuses.
Keywords: Emissary vein, Foramen, Mastoid, Temporal
Introduction
Emissary veins travel through the emissary foramina of the skull and connect the intracranial veins with the extracranial. They are valveless veins and blood can flow in either direction, however the flow is usually away from the brain [1]. The mastoid emissary vein connects the posterior auricular vein with the sigmoid sinus. The emissary mastoid foramen transmits the mastoidal emissary vein and is present at the mastoid process of the temporal bone. It is not uncommon to see this foramen over the occipitomastoid suture [2]. The mastoid emissary foramen also transmits a branch of the occipital artery, which is going to supply the duramater of the posterior cranial fossa [3]. It has been reported that the number of mastoid emissary foramina may vary between zero to four [2, 4].
The mastoid emissary vein passes through the mastoid foramen, making the connection between the sigmoid sinus into the posterior auricular and occipital veins [5]. The blood which runs through the mastoid emissary vein is usually sluggish; however during the raised intracranial tension; this vein can become the source of drainage and decrease the intracranial pressure [6]. Notification of intracranial variations is important during the anesthetic blocks and the evaluation of regional anatomy is important to avoid the misinterpretations [7]. Modern operation procedures, nerve block and acupuncture need a clear understanding of the surrounding anatomy [8]. The mastoid emissary vein may get involved in the spread of craniofacial tumours and infections into the cranial cavity [2]. The identification of mastoidal emissary vein is important in the neurosurgical practice to diagnose the pathological from the normal structures. Their importance has been very well recognized in the plastic surgical field [9]. However, the detailed studies on the mastoid emissary veins are lacking in the literature, especially in the Indian subcontinent. The objective of the present study was to estimate the prevalence of mastoid emissary foramina in the temporal bones of the adult human skulls of South Indian origin and to study their number and morphology.
Materials and Methods
The present study included 48 adult human skull bases of South Indian origin which were obtained from the gross anatomy laboratory of our institution. The exact age and gender of the specimens were not determined. The skulls which showed pathological changes at the cranial base were excluded from the present study. The anterior, middle and posterior skull base region was carefully examined for the exclusion criteria like bony erosions, invasions, spurs and growths. The skull bases which exhibited these types of changes which are suggestive of tumor invasion were considered as pathologically abnormal and were excluded. The cranial cavity was also examined for the pathological signs suggestive of a tumor invasion and if found were excluded. The mastoid parts of the 96 temporal bones were macroscopically observed for the prevalence and number of the emissary foramina. A magnifying lens has been used to observe the mastoid emissary foramina. The patency of the each foramen was confirmed by passing a probe. The observations were made on the mastoid part of the temporal bone, temporo occipital suture and part of the occipital bone which is just medial to the temporo occipital suture. Each specimen was examined by three authors of the present study and discussed, before writing the observations.
Results
In the present study, the mastoidal emissary foramen was observed in 88 temporal bones (91.7%). The morphological distribution of the mastoid emissary foramina of the present study are represented in Fig. 1. The foramen was observed single (Fig. 2A) in 60 temporal bones (62.5%), double (Fig. 2B) in 22 bones (22.9%), and triple (Fig. 2C) in 6 temporal bones (6.2%). The mastoidal emissary foramen was absent in 8 temporal bones (8.3%). The foramen was bilaterally absent in 3 skulls (3.1%) and unilaterally absent in 2 skulls (2.1%). Among the unilateral absence, both were observed on the right side. The side wise distribution of the mastoid emissary foramina of the present study are represented in Table 1.
Fig. 1.

Morphological distribution of the mastoid emissary foramina observed in the present study (n=96).
Fig. 2.
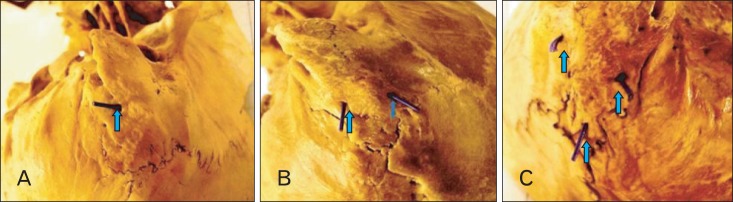
Pictures of the skull bases of the present study showing. (A) Single mastoidal emissary foramen (62.5%). (B) Double mastoidal emissary foramen (22.9%). (C) Triple mastoidal emissary foramen (6.2%).
Table 1.
Showing the side wise distribution of the mastoid emissary foramina (n=96)
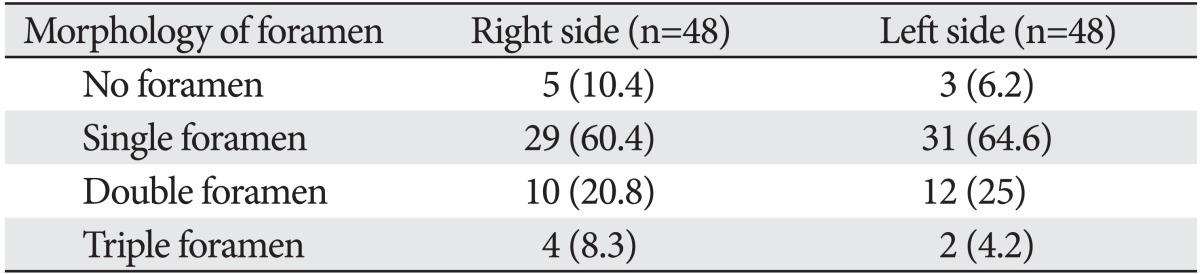
Values are presented as number (%).
Discussion
The anatomical and physiological researches have described the anthropological significance of the emissary mastoid vein in the human evolution and preferential intracranial venous flow into the vertebral veins in the bipedal man [9, 10]. As an upright human posture necessitated the delivery of blood away from the brain into the vertebral veins, the venous channels like the enlarged occipital, transverse sinuses, accessory hypoglossal canals and emissary venous foramina developed [11]. These are considered to be the epigenetic adaptations of humans for delivering the blood preferentially into the vertebral venous plexus [12]. In Australopithecus, the occipital vein is the major pathway for the venous drainage. This is unlike in Homo sapiens, where the size of occipital vein was very small leading to the evolution of some new veins. Mastoid emissary vein is one among those and this is the reason for the development of the mastoid foramen in the human modern skull [11]. It has been described that the sigmoid sinus opens into the vertebral venous plexus in the standing position and drains into the internal jugular vein during the recumbent position [13]. The mastoidal emissary foramen is often absent in the skulls of nonhuman primates like gorillas and chimpanzees. It has been opined that, during the process of human evolution, the size of the mastoid emissary vein was increased [11]. Goucha et al. [13] reported that, remodeling of the mastoid process of temporal bone during the human evolution is correlating with the origin of the emissary mastoid vein. Everything in the art of medicine, right from examining a plain X-ray until operating the human body, requires a sound knowledge of anatomy [14]. Variations in the foramina of the skull have aroused the curiosity among the anatomists for many decades. These non-metric skull variants would help in finding the genetic relationships of the species among the populations [15]. The mastoid emissary foramen is considered as anatomical landmark for differentiation of the species and is important in forensic science anthropology [6].
Craniofacial bone variations have been studied since the beginning of the century. These variations are studied by using the cadavers and skulls in the anatomy laboratory [7]. The variations of skull foramina are of interest due to the clinical implications these structures cause in the fields of neurology, neurosurgery and maxillofacial surgery. Few morphological anatomical variations were often neglected by the surgeons and are described in the gross anatomy text books as rare anomalous structures [16]. Recognition of variant foramina of skull is important to understand the regional neurovascular anatomy and to segregate the normal from abnormal structures [17]. The misinterpretation of these types of anomalies can cause complications during the surgical procedures and lead to procedure failures due to iatrogenic neurovascular injury [18]. With the increased application of magnetic nuclear resonance and computed axial tomogram, the skull foramina are increasingly studied in the clinical set up. The observation of foramina of skull has become a must do criteria in the clinical diagnosis [19], but the literature about them is missing in the gross anatomy texts.
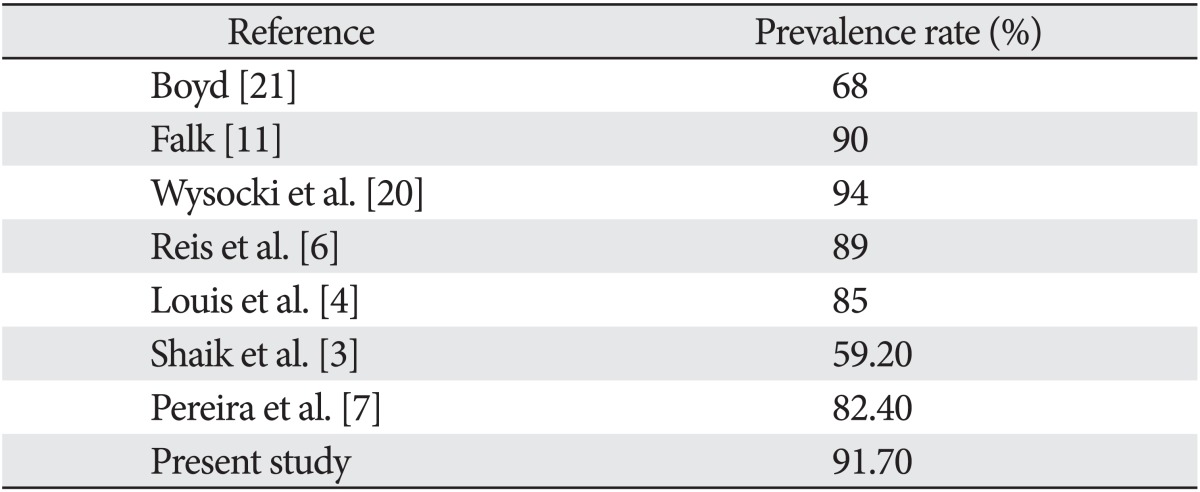
In a study from Louis et al. [4], the incidence of mastoid emissary vein was reported 98% for the right side and 72% for left side. They reported that, in 85% of cases, the occipital and mastoid emissary veins formed a confluence of veins. Kim et al. [9] observed that, 83.7% of their samples were found to have at least one mastoidal emissary foramen. Wysocki et al. [20] observed the mastoid foramen in 94% of their cases. In a study from Brazilian skulls, by Pereira et al. [7], it was reported that the mastoid foramen was recorded on the right side in 90% and 85% cases on the left side of male skulls. In female skulls, the mastoid foramen was also observed in 72.7% and 81.8% of cases on right and left sides respectively. The limitation of the present study is the gender related comparison, which is not taken into consideration in the present study. Boyd [21] observed a prevalence of emissary mastoid foramen in 68% cases from 1478 modern human skulls, in contrast Falk [11], reported an incident rate of 90% from 51 samples. Reis et al. [6] reported an incidence of 89% from 40 cadavers. The prevalence rate of mastoid emissary foramina in the present study has been compared with the previous reports and the comparison is represented in Table 2. The present study has observed that the prevalence rate is almost similar to the previous reports. The present study reports that there was no significant difference among the races with respect to the incidence of mastoid emissary veins. The study states that the mastoid emissary foramina are a feature of the human.
Table 2.
Prevalence of mastoid emissary foramen with the data from literature
Friedmann et al. [22] reported that, it is common to find the temporal bone venous variations in patients of CHARGE syndrome. They observed that, the most common variation was a mastoid emissary vein, connecting the occipital vein with the sigmoid sinus. In their surgical practice, they had to change their surgical approach due the variant course of the vein. Friedmann et al. [22] proposed that, variant emissary veins have to be included as the preoperative assessment in the inner ear implant surgeries. Computed tomogram scan of the temporal skull bone may exhibit some anomalous veins which require preoperative visualization and a different surgical approach in the mastoidectomy procedure.
The venous variation pattern shows that there is a defective development of the superior bulb of the internal jugular vein and the sigmoid venous sinus to develop, which results in the formation of emissary veins. Identification of these variant veins is important in an otologic surgery to avoid the dangerous catastrophic hemorrhage. The mastoid emissary vein is involved as a source of blood loss during the ear surgeries and skull base operation procedures, especially in the lateral and retrosigmoid approaches. The complete morphological idea of the mastoid emissary vein will avoid the complication [4]. The usage of the emissary mastoid vein is a better technique for understanding an isolated sigmoid or transverse dural venous sinus [4]. Inadvertent injuries to the mastoid emissary veins may cause a significant bleeding. It has also been reported that, it can lead to thrombus and embolus formation due to their bidirectional flow and close proximity to the sigmoid sinus. In this context, recognition of mastoid emissary veins and managing the bleeding from this vessel is important to the surgeon operating in this area. This is important in the craniofacial surgery, while operating the cases of craniosynostosis, where mastoid emissary vein may be the only drainage route of the brain [9].
Cheatle [23] reported a case of a male patient with history of carbuncle in the neck, eventually developed cavernous venous thrombosis and meningitis. During his autopsy procedure, it was observed that the infection was spreading from the occipital vein, through the mastoid emissary vein to the transverse sinus, and then from the superior petrosal sinus to the cavernous venous sinus. It is reported that the knowledge of mastoid canals and grooves is very important to the otorhinolaryngologists and neurosurgeons [3]. In the present study, we believe that this investigation has provided additional information on the morphology of the mastoid emissary foramina. In the present study, the mastoidal emissary vein was prevalent in a large number of cases. It was observed that the accessory mastoidal emissary foramina were present in 29.1% of cases. Recognition of the mastoidal emissary veins and accessory mastoid emissary veins during the ear surgery is essential to avoid the dangerous blood loss. In the human neurosurgical practice, the knowledge about this vein is important due to the variability in their number and their relation to the sigmoid sinus.
With the observations of the present study, the clinicians and researchers examining the mastoid emissary foramina may have an anatomical reference. Implications for the future study about this subject would involve the radiological examination of these foramina with the usage of computed tomography (CT) scans and magnetic resonance imaging (MRI) studies. More details of the emissary veins and correlation with the other emissary veins in the skull can be performed by using the radiological methods [24]. It seems worthy that the perception of existence of mastoid foramen through any medical imaging techniques could be used to estimate the pattern of mastoid emissary vein for the further clinical implications. The bony foramina are more clearly visible in the computed tomogram scans. So the foramina seen in the CT scan film can indicate the topography of the emissary vein. This will definitely guide the radiologists in understanding the course of an emissary vein. However in an MRI film, the emissary vein itself is obvious. The future implication of the present study would include studying the mastoid emissary foramina radiologically by using CT scan and MRI films. The limitation of the present study would include the morphometry of the mastoid emissary foramina, which is not done in the present study. It is believed that the dimensional differences among the foramina seem to exist. The dimension of the foramina would be relavant to the evolutionary feature by the erect posture of the human. It could be helpful to improve the clinical radiologic examination of the mastoid emissary formina. The better ideas about this subject include studying the dimensions of mastoidal emissary foramina by using the scion image analyzer software. This further research may serve more distinct evidence about the clinical and anatomical implications mentioned in this subject.
References
- 1.Singhal S, Ravindranath R. Occipital emissary foramina in South Indian modern human skulls. ISRN Anat. 2013;2013:727489. doi: 10.5402/2013/727489. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sicher H, DuBrul EL. Oral anatomy. 6th ed. Rio de Janeiro: Guanabara Koogan; 1977. [Google Scholar]
- 3.Shaik HS, Shepur MP, Desai SD, Thomas ST, Maavishettar GF, Haseena S. Study of mastoid canals and grooves in South Indian skulls. Indian J Med Healthc. 2012;1:32–33. [Google Scholar]
- 4.Louis RG, Jr, Loukas M, Wartmann CT, Tubbs RS, Apaydin N, Gupta AA, Spentzouris G, Ysique JR. Clinical anatomy of the mastoid and occipital emissary veins in a large series. Surg Radiol Anat. 2009;31:139–144. doi: 10.1007/s00276-008-0423-5. [DOI] [PubMed] [Google Scholar]
- 5.El Kettani C, Badaoui R, Fikri M, Jeanjean P, Montpellier D, Tchaoussoff J. Pulmonary oedema after venous air embolism during craniotomy. Eur J Anaesthesiol. 2002;19:846–848. doi: 10.1017/s0265021502291358. [DOI] [PubMed] [Google Scholar]
- 6.Reis CV, Deshmukh V, Zabramski JM, Crusius M, Desmukh P, Spetzler RF, Preul MC. Anatomy of the mastoid emissary vein and venous system of the posterior neck region: neurosurgical implications. Neurosurgery. 2007;61(5 Suppl 2):193–200. doi: 10.1227/01.neu.0000303217.53607.d9. [DOI] [PubMed] [Google Scholar]
- 7.Pereira GA, Lopes PT, Santos AM, Pozzobon A. Study of landmarks in dried skulls in a Brazil population. J Morphol Sci. 2013;30:94–97. [Google Scholar]
- 8.Singh R. Morphometric analysis of infraorbital foramen in Indian dry skulls. Anat Cell Biol. 2011;44:79–83. doi: 10.5115/acb.2011.44.1.79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kim LK, Ahn CS, Fernandes AE. Mastoid emissary vein: anatomy and clinical relevance in plastic & reconstructive surgery. J Plast Reconstr Aesthet Surg. 2014;67:775–780. doi: 10.1016/j.bjps.2014.03.002. [DOI] [PubMed] [Google Scholar]
- 10.Falk D, Conroy GC. The cranial venous sinus system in Australopithecus afarensis. Nature. 1983;306:779–781. [Google Scholar]
- 11.Falk D. Evolution of cranial blood drainage in hominids: enlarged occipital/marginal sinuses and emissary foramina. Am J Phys Anthropol. 1986;70:311–324. doi: 10.1002/ajpa.1330700306. [DOI] [PubMed] [Google Scholar]
- 12.Kimbel WH. Variation in the pattern of cranial venous sinuses and hominid phylogeny. Am J Phys Anthropol. 1984;63:243–263. doi: 10.1002/ajpa.1330630302. [DOI] [PubMed] [Google Scholar]
- 13.Goucha S, Mnif N, Bouhala T, Tenzakhti F, El Andaloussi H, Fazaa B, Hamza R, Kamoun MR. Value of imaging in GAPO syndrome. J Radiol. 2002;83(2 Pt 1):153–156. [PubMed] [Google Scholar]
- 14.Mavrodi A, Paraskevas G. Evolution of the paranasal sinuses' anatomy through the ages. Anat Cell Biol. 2013;46:235–238. doi: 10.5115/acb.2013.46.4.235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kaur J, Srivastava D, Singh D, Raheja S. The study of hyperostosic variants: significance of hyperostotic variants of human skulls in anthropology. Anat Cell Biol. 2012;45:268–273. doi: 10.5115/acb.2012.45.4.268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Keskil S, Gözil R, Calgüner E. Common surgical pitfalls in the skull. Surg Neurol. 2003;59:228–231. doi: 10.1016/s0090-3019(02)01038-8. [DOI] [PubMed] [Google Scholar]
- 17.Freire AR, Rossi AC, de Oliveira VC, Prado FB, Caria PH, Botacin PR. Emissary foramens of the human skull: anatomical characteristics and its relations with clinical neurosurgery. Int J Morphol. 2013;31:287–292. [Google Scholar]
- 18.Gözil R, Kadioglu D, Calgüner E. Occipital emissary foramen in skulls from central Anatolia. Acta Anat (Basel) 1995;153:325–326. [PubMed] [Google Scholar]
- 19.Berge JK, Bergman RA. Variations in size and in symmetry of foramina of the human skull. Clin Anat. 2001;14:406–413. doi: 10.1002/ca.1075. [DOI] [PubMed] [Google Scholar]
- 20.Wysocki J, Reymond J, Skarzyński H, Wróbel B. The size of selected human skull foramina in relation to skull capacity. Folia Morphol (Warsz) 2006;65:301–308. [PubMed] [Google Scholar]
- 21.Boyd GI. The emissary foramina of the cranium in man and the anthropoids. J Anat. 1930;65(Pt 1):108–121. [PMC free article] [PubMed] [Google Scholar]
- 22.Friedmann DR, Amoils M, Germiller JA, Lustig LR, Glastonbury CM, Pramanik BK, Lalwani AK. Venous malformations of the temporal bone are a common feature in CHARGE syndrome. Laryngoscope. 2012;122:895–900. doi: 10.1002/lary.23205. [DOI] [PubMed] [Google Scholar]
- 23.Cheatle A. The mastoid emissary vein and its surgical importance. Proc R Soc Med. 1925;18:29–34. doi: 10.1177/003591572501801223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Murlimanju BV, Prabhu LV, Pai MM, Jaffar M, Saralaya VV, Tonse M, M D P. Occipital emissary foramina in human skulls: an anatomical investigation with reference to surgical anatomy of emissary veins. Turk Neurosurg. 2011;21:36–38. [PubMed] [Google Scholar]