

Abstract
Vital bleaching is one of the most requested cosmetic dental procedures asked by patients who seek a more pleasing smile. This procedure consists of carbamide or hydrogen peroxide gel applications that can be applied in-office or by the patient (at-home/overnight bleaching system). Some in-office treatments utilise whitening light with the objective of speeding up the whitening process. The objective of this article is to review and summarise the current literature with regard to the effect of light-activation sources on in-office tooth bleaching. A literature search was conducted using Medline, accessed via the National Library of Medicine Pub Med from 2003 to 2013 searching for articles relating to effectiveness of light activation sources on in-office tooth bleaching. This study found conflicting evidence on whether light truly improve tooth whitening. Other factors such as, type of stain, initial tooth colour and subject age which can influence tooth bleaching outcome were discussed. Conclusions: The use of light activator sources with in-office bleaching treatment of vital teeth did not increase the efficacy of bleaching or accelerate the bleaching.
Keywords: Bleaching, carbamide, hydrogen peroxide, in-office bleaching, whitening
INTRODUCTION
The causes of tooth discolouration are usually various and multifaceted. They have been classified as extrinsic, intrinsic and internalised discolouration.1 The extrinsic discolouration is associated with the use of tea, coffee, tobacco, some foods such as blueberries, and red wine.2 Intrinsic stains (dentin staining) may be due to systemic conditions, use of medications after the permanent teeth have erupted (e.g., minocycline) or during their development (tetracycline), childhood diseases, infection or trauma to a primary tooth while the underlying tooth is developing, trauma to a permanent tooth or natural aging changes and the accumulation of stain that has entered the teeth.1
There is an increase in patient awareness of the ability to improve the appearance of their discoloured teeth. Not only these patients are seeking to improve the esthetic appearance of their smiles, they are also seeking an effective method. There are several ways to manage tooth discolouration, which include crowns, veneers, or tooth bleaching. For crowns and veneers, these treatment options entail a moderate loss of dental hard tissue. Vital tooth bleaching is not only a less costly alternative to bonded restorative dentistry; it is a conservative and non-invasive technique which has been well accepted to be safe and effective.3
Tooth bleaching using oxalic acid was first introduced in 18484, followed by hydrogen peroxide (HP) in 1884.5 Contemporary, tooth bleaching systems are primarily based on oxidation by HP or one of its precursors such as, carbamide peroxide (CP).6 Hydrogen peroxide releases oxygen that breaks down conjugated bonds in protein chains associated with stain into a single bond. This will result in more absorption of colour wavelengths and resulting in the reflection of little colour (i.e., a whitening effect).2 In the meantime, various treatment modalities are available which include over-the-counter bleaching (self-administered), in-office bleaching (professionally administered) and dentist supervised take-home bleaching (professionally dispensed).7
Home bleaching
Home bleaching is considered a safe and effective treatment.8,9,10 This technique is performed with low concentration hydrogen peroxide (4%-8%) or carbamide peroxide (10%-22%) formulations, which are inserted into trays. These trays are placed in the mouth for 2-8 hours per day, over the course of 2-6 weeks.11
Over-the-counter bleaching
An OTC, 5.3% hydrogen peroxide-coated polyethylene strip (Crest Whitestrips, Procter & Gamble) was recently introduced to the market. According to the manufacturer's instruction, the patient applies two strips per day for 30 minutes each. A similar 6.5% hydrogen peroxide-coated strip is available by prescription. Clinical studies comparing the whitening efficacy of 10% carbamide peroxide (which breaks down in 3.5% hydrogen peroxide) with the efficacy of the hydrogen peroxide-coated strips have demonstrated that the polyethylene strips may be an acceptable alternative to the night guard method of at-home whitening.12
In-office bleaching
Although in-office bleaching is performed using high concentration hydrogen peroxide (15%-40%),12 it becomes a widely used procedure because of these advantages: Minimally invasive, immediate visible results and no need of patient cooperation.13 Also, in-office whitening is the best for patients who need close monitoring for clinical conditions such as pronounced gingival recession or deep, unrestored abfraction lesions, and necessary for tooth discolouration associated with endodontic therapy.2
Since the introduction of in-office bleaching treatments, the use of curing lights (including halogen curing lights, plasma arches, LED, LED plus lasers, lasers) has been recommended to accelerate the action of the bleaching gel.14 It is believed that most light sources decompose peroxide faster (by increasing the temperature) to form free radicals which whiten teeth.15,16,17
However, some studies reported that the use of light sources did not improve the in-office bleaching treatment of vital teeth.17,18 The clinical results obtained with the use of these lights were poor, showing an increase in tooth sensitivity and reduced long-term colour stability, especially when the treatment was done in one appointment.14 Recent developments in in-office bleaching systems that use a chemical catalyst combined with light-cured block-out materials and compounds have resulted in decreased tooth sensitivity and enhanced treatment and have demonstrated improved results.18 Therefore, the aim of this paper is to review the current literature to evaluate the effect of light-activation sources on in-office tooth bleaching.
With the help of currently available literature, the electronic database “the National Library of Medicine” PubMed was searched for scientific articles relating to effectiveness of light activation sources on in-office tooth bleaching. The search was carried out between 2003 and 2013.
Colour evaluation
Before and after bleaching, the shade is usually assessed using two different methods: Vita Shade Guide, and a spectrophotometer.5
Standard Vita Shade Guide
This is a visual and subjective assessment method. The investigator conduct all the shade comparisons using a standard Vita Shade Guide (Vita Zahnfabrik, Germany) before and after bleaching. Shade guide tabs are arranged from B1to C4, each corresponding to a numerical value from 1 to16, the smaller the numeric value the lighter the tooth.5 This method is the most common, as it is a quick, simple procedure and has been used successfully in many studies.10,19,20,21,22,23
Spectrophotometer
This is an instrumental method for shade matching and has been preferred over the visual evaluation, because it makes the process more practical and statistically more reliable.14 Spectrophotometric colour measurement of specimens was based on the CIE L*a*b* system. The L*a*b* system organises all existing colours within a three-dimensional colour space. L* represents the degree of lightness and ranges from 0 (black) to 100 (white); a* represents the green-red axis while b* represents the blue-yellow axis.5
This system was defined by the International Commission on Illumination in 196724 and is referred to as CIE Lab. The colour comparison before and after treatment is given by the differences between the two colours (ΔE), which is calculated using the formula:
ΔE = [(ΔL*)2 + (Δa*)2 + (Δb*)2]1/2
The effect of light-activation sources on in-office tooth bleaching
Strong controversy surrounds the success of light sources has been detected. Some researchers believe that it is effective in the bleaching process, while others believe only certain lights are effective and others reported no effect [Tables 1 and 2].17,18,25,26,27,28,29,30,31,34
Table 1.
Studies demonstrated that the use of light-activation sources did not affect the outcome of in-office bleaching
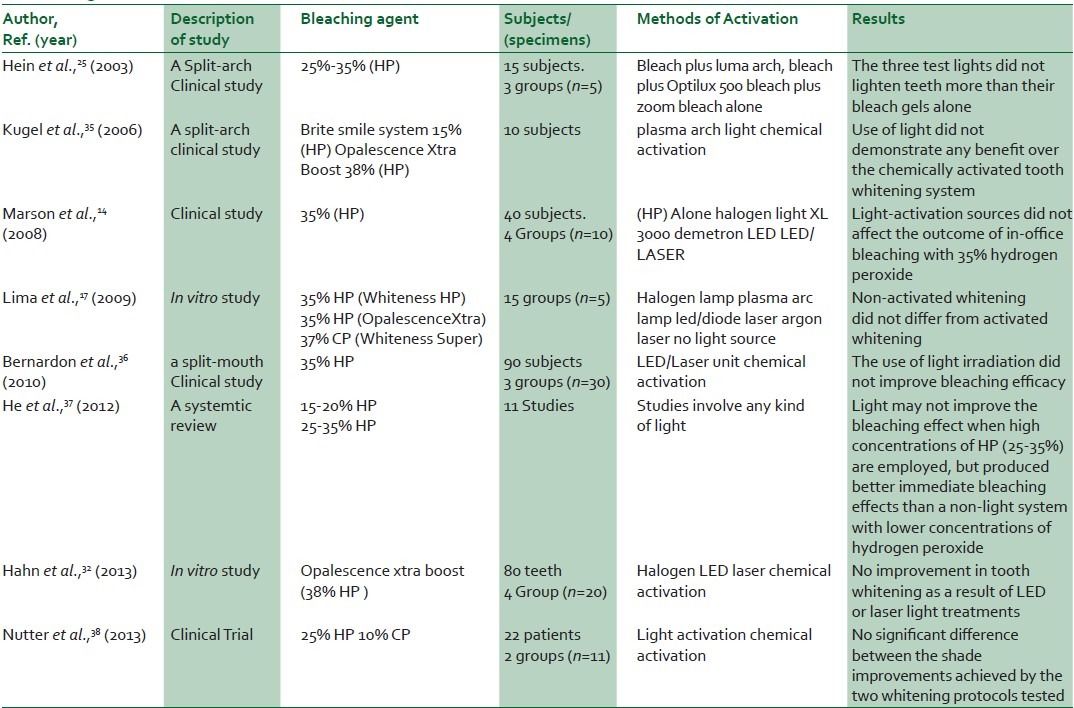
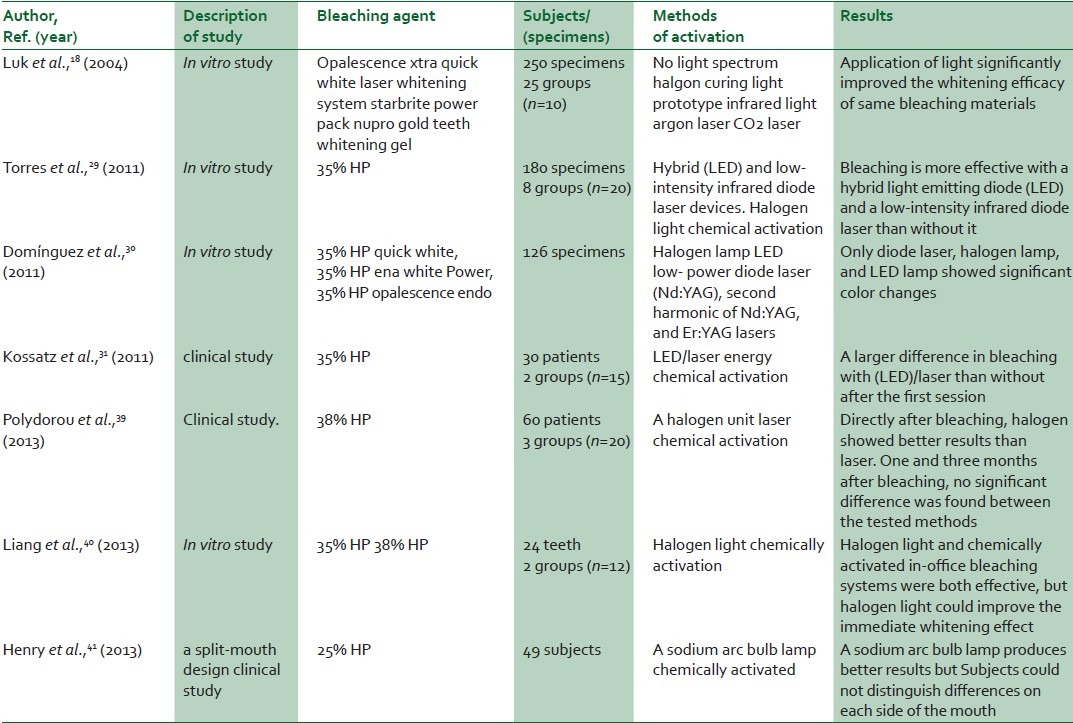
Table 2.
Studies demonstrated that application of light significantly improved the whitening efficacy of some bleaching materials
Hein et al., 200325 reported no difference in the whitening effect of bleaching gels [25%-35% (HP)] with or without three different lights (LumaArch, Optilux 500, and Zoom!). They concluded that the proprietary chemicals added to the bleaching gels acted as catalysts in the whitening process and were solely responsible for activation, where as the lights had no influence.
Luk et al., 200418 reported that colour change were significantly affected by inter action of the bleaching and light variables, and the application of light significantly improved the whitening efficacy of same bleaching materials. Kugel et al., 200635 reported that the use of light did not demonstrate any benefit over the chemically activated tooth whitening system after a 2-week recall. Marson et al., 200814 reported that the in-office bleaching treatment of vital teeth with 35% hydrogen peroxide did not show improvement with the use of any auxiliary sources tested (halogen light, LED, LED/Laser).
Lima et al., 200917 summarised that non-activated whitening did not differ from activated whitening. Where, approximately 35% HP was used with different light sources (LED/diode laser, a halogen lamp, plasma arc lamp, argon laser). Bruzell et al., 200942 reported no difference in efficacy between teeth bleached with or without irradiation for any of the products. The inspection of teeth was performed one week after bleaching using seven bleaching products with or without simultaneous use of seven different bleaching lamps.
Bernardon et al., 201036 reported that similar results were observed when teeth bleached using the in-office technique and light irradiation were compared to teeth bleached without light irradiation to evaluating the clinical performance of 35% HP bleaching gel with and without use of LED/Laser unit. In a study of Browning and Swift 201143 of power bleaching it was stated that light sources used in tooth whitening do not generate sufficient heat to damage teeth. They concluded that high concentrations of chemicals are responsible for faster whitening and that light sources are therefore superfluous in the whitening process.
Torres et al., 201129 reported that bleaching is more effective with a hybrid light-emitting diode (LED) and a low-intensity infrared diode laser than the control group. This research evaluated the effectiveness of the colour change of hybrid LED and low-intensity infrared diode laser devices for activating dental bleaching, bleaching without light, and bleaching with halogen light. Domνnguez et al., 201130 reported that only the diode laser, halogen lamp and LED lamp showed significant colour changes when using six different photo activation systems on three different 35% hydrogen peroxide whiteners. It was concluded that the light source is more important than the bleaching agent in the whitening process.
Kossatz et al., 201131 reported a larger difference in bleaching with a LED/laser than without it on 35% HP gel after the first session of bleaching, but after two sessions, the use of LED/laser light activation did not improve bleaching speed. He et al., 201237 reported that a light-activated system produced better immediate bleaching effects than a non-light system with lower concentrations of hydrogen peroxide. When high concentrations of HP (25-35%) were employed, there was no difference in the immediate bleaching effect or short-term bleaching effect between the light-activated system and the non-light system.
Hahn et al., 201332 could not find an improvement in tooth whitening as a result of LED or laser light treatments, when evaluating the colour stability of bleaching with Opalescence Xtra Boost (38% hydrogen peroxide) using four different methods: activation with halogen, LED, laser or chemical activation. Polydorou et al., 201339 reported that directly after bleaching, the use of halogen showed better results than laser (P ≤ 0.05), on evaluating the colour stability of vital bleaching using a halogen unit, laser, or only chemical activation up to 3 months after treatment.
Liang et al., 201340 concluded that halogen light and chemically activated in-office bleaching systems were both effective for tooth whitening; however, halogen light activation could improve the immediate tooth whitening.
Nuttera et al., 201338 reported that there was no significant difference in shade change between in-office bleaching with light activated 25% hydrogen peroxide gel followed by 2 weeks at home, night-time bleaching with 10% carbamide peroxide gel in a customised bleaching tray and in-office bleaching with 25% hydrogen peroxide without light activation followed by 2 weeks at home, night time bleaching with 10% carbamide peroxide gel in a customised bleaching tray.
Henry et al., 201341 reported that on a split-mouth design study, the use of a sodium arc bulb lamp with 25% hydrogen peroxide for in-office whitening produces better results on maxillary teeth up to 1 week after whitening is completed. Using only gel for whitening could not distinguish differences on each side of the mouth.
DISCUSSION
This review summarises the present literature about the effect of light-activation sources on in-office tooth bleaching. Bleaching has been accepted as the least aggressive method for treating discoloured teeth. However, the effectiveness of in-office systems has been controversial. Manufacturers have introduced “bleaching” lights that are reported to accelerate the bleaching process.44 This finding is in agreement with the studies of Torres et al. 2011,29 Domνnguez et al. 2011,30 and Luk et al. 200418 who reported that the application of light significantly improved the whitening efficacy of bleaching materials. This may be attributed to tooth dehydration45,46 that presumably is greater with increased tooth heating on using light activation source.
However, some researchers have stated that no acceleration or increase in efficacy occurs when using light sources.35,36,42 Light-activated whitening systems add cost, occupy operatory space, can cause burning of the soft tissue, and can increase operatory temperature.2 The use of a light for in-office whitening may not be justified due to the risks involved.
The controversial results which are reported with different tooth bleaching systems can be attributed to various factors such as: Base-line colour of the teeth of the chosen subjects, the type and concentration of the bleaching product, the time period for the in-chair treatment as well as the treatment period.7
The more yellow the teeth at baseline, the better the outcome of tooth bleaching.47 In the study of Gerlach and Zhou 2001 on 600 subjects, they demonstrated a significant relationship between the subject's age and the magnitude of bleaching response with younger subjects experiencing better tooth-bleaching results.47
The efficacy of hydrogen peroxide containing products are approximately the same when compared with carbamide peroxide-containing products with equivalent or similar hydrogen peroxide content and delivered using similar format and formulations, either tested in vitro48 or in vivo.49,50
Heymann 200551 has suggested that the concentration and contact time of the bleaching agent to the tooth are very important for the bleaching outcome. The study by Matis et al. 200744 agreed that the contact time of the bleaching agent appears to be an important factor; however, the concentration is not as important as a factor for the bleaching outcome. This may be attributed to the longer bleaching time which allow bleaching agent to react more thoroughly with coloured compound.5
Moreover, Sulieman et al. 200415 compared the in vitro tooth bleaching efficacy of gels containing 5-35% hydrogen peroxide. He found that the higher the concentration, the lower the number of gel applications required to produce uniform bleaching. Similar results were found by Leonard et al. 1998 who compared the in vitro tooth bleaching efficacy of 5%, 10% and 16% carbamide peroxide gels and found the whitening was initially faster for the 16% and 10% than the 5% concentration. However, the efficacy of the 5% carbamide peroxide gel approached the highest concentrations when the treatment time was extended52
In a clinical study using custom-made bleaching trays, Kihn et al. 200050 concluded that a 15% carbamide peroxide gel showed significantly more tooth whitening than a 10% carbamide gel after use for 2 weeks. This result was in agreement with another clinical study reported by Matis et al. 200053 who extended the treatment time for 6 weeks and the differences in tooth lightness were no longer of statistical significance. The initial faster rate of bleaching for higher concentrations of carbamide peroxide has also been observed when bleaching tetracycline stained teeth in vivo over a 6-month period.54
CONCLUSIONS
The in-office bleaching treatment of vital teeth did not show improvement with the use of light activator sources for the purpose of accelerating the process of the bleaching gel and achieving better results.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Watts A, Addy M. Tooth discolouration and staining: A review of the literature. Br Dent J. 2001;190:309–16. doi: 10.1038/sj.bdj.4800959. [DOI] [PubMed] [Google Scholar]
- 2.Boksman L. Current status of tooth whitening: Literature review. Dent Today. 2006;25:74, 76–9. [PubMed] [Google Scholar]
- 3.Sun L, Liang S, Sa Y, Wang Z, Ma X, Jiang T, et al. Surface alteration of human tooth enamel subjected to acidic and neutral 30% hydrogen peroxide. J Dent. 2011;39:686–92. doi: 10.1016/j.jdent.2011.07.011. [DOI] [PubMed] [Google Scholar]
- 4.Sulieman M, Addy M, Macdonald E, Rees JS. The bleaching depth of a 35% hydrogen peroxide based in-office product: A study in vitro. J Dent. 2005;33:33–40. doi: 10.1016/j.jdent.2004.07.008. [DOI] [PubMed] [Google Scholar]
- 5.Wang W, Zhu Y, Li J, Liao S, Ai H. Efficacy of cold light bleaching using different bleaching times and their effects on human enamel. Dent Mater J. 2013;32:761–6. doi: 10.4012/dmj.2013-109. [DOI] [PubMed] [Google Scholar]
- 6.Lee BS, Huang SH, Chiang YC, Chien YS, Mou CY, Lin CP. Development of in vitro tooth staining model and usage of catalysts to elevate the effectiveness of tooth bleaching. Dent Mater. 2008;24:57–66. doi: 10.1016/j.dental.2007.01.012. [DOI] [PubMed] [Google Scholar]
- 7.Hayward R, Osman Y, Grobler SR. A clinical study of the effectiveness of a light emitting diode system on tooth bleaching. Open Dent J. 2012;6:143–7. doi: 10.2174/1874210601206010143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Jorgensen MG, Carroll WB. Incidence of tooth sensitivity after home whitening treatment. J Am Dent Assoc. 2002;133:1076–82. doi: 10.14219/jada.archive.2002.0332. [DOI] [PubMed] [Google Scholar]
- 9.Zeknois R, Matis BA, Cochran MA, Al Shetri SE, Eckert GJ, Carlson TJ. Clinical evaluation of in-office and at-home bleaching treatments. Oper Dent. 2003;28:114–21. [PubMed] [Google Scholar]
- 10.Auschill TM, Hellwig E, Schmidale S, Sculean A, Arweiler NB. Efficacy, side effects and patients’ acceptance of different bleaching techniques (OTC, in-office, at-home) Oper Dent. 2005;30:156–63. [PubMed] [Google Scholar]
- 11.de Almeida LC, Costa CA, Riehl H, dos Santos PH, Sundfeld RH, Briso AL. Occurrence of sensitivity during at-home and in-office tooth bleaching therapies with or without use of light sources. Acta Odontol Latinoam. 2012;25:3–8. [PubMed] [Google Scholar]
- 12.Perdigão J, Baratieri LN, Arcari GM. Contemporary trends and techniques in tooth whitening: A review. Pract Proced Aesthet Dent. 2004;16:185–92. [PubMed] [Google Scholar]
- 13.Ferreira Sda S, Araújo JL, Morhy ON, Tapety CM, Youssef MN, Sobral MA. The effect of fluoride therapies on the morphology of bleached human dental enamel. Microsc Res Tech. 2011;74:512–6. doi: 10.1002/jemt.20939. [DOI] [PubMed] [Google Scholar]
- 14.Marson FC, Sensi LG, Vieira LC, Araujo E. Clinical evaluation of in-office dental bleaching treatments with and without the use of light-activation sources. Oper Dent. 2008;33:15–22. doi: 10.2341/07-57. [DOI] [PubMed] [Google Scholar]
- 15.Sulieman M, Addy M, MacDonald E, Rees JS. The effect of hydrogen peroxide concentration on the outcome of tooth whitening: An in vitro study. J Dent. 2004;32:295–9. doi: 10.1016/j.jdent.2004.01.003. [DOI] [PubMed] [Google Scholar]
- 16.Joiner A. Tooth colour: A review of the literature. J Dent. 2004;32:3–12. doi: 10.1016/j.jdent.2003.10.013. [DOI] [PubMed] [Google Scholar]
- 17.Lima DA, Aguiar FH, Liporoni PC, Munin E, Ambrosano GM, Lovadino JR. In vitro evaluation of the effectiveness of bleaching agents activated by different light sources. J Prosthodont. 2009;18:249–54. doi: 10.1111/j.1532-849X.2008.00420.x. [DOI] [PubMed] [Google Scholar]
- 18.Luk K, Tam L, Hubert M. Effect of light energy on peroxide tooth bleaching. J Am Dent Assoc. 2004;135:194–201. doi: 10.14219/jada.archive.2004.0151. [DOI] [PubMed] [Google Scholar]
- 19.Sulieman M, MacDonald E, Rees JS, Addy M. Comparison of three in-office bleaching systems based on 35% hydrogen peroxide with different light activators. Am J Dent. 2005;18:194–7. [PubMed] [Google Scholar]
- 20.de Silva Gottardi M, Brackett MG, Haywood VB. Number of in-office light-activated bleaching treatments needed to achieve patient satisfaction. Quintessence Int. 2006;37:115–20. [PubMed] [Google Scholar]
- 21.Leonard RH, Jr, Haywood VB, Eagle JC, Garland GE, Caplan DJ, Matthews KP, et al. Night guard vital bleaching of tetracycline-stained teeth: 54 months post treatment. J Esthet Dent. 1999;11:265–77. doi: 10.1111/j.1708-8240.1999.tb00408.x. [DOI] [PubMed] [Google Scholar]
- 22.Guan YH, Lath DL, Lilley TH, Willmot DR, Marlow I, Brook AH. The measurement of tooth whiteness by image analysis and spectrophotometry: A comparison. J Oral Rehabil. 2005;32:7–15. doi: 10.1111/j.1365-2842.2004.01340.x. [DOI] [PubMed] [Google Scholar]
- 23.Goodson JM, Tavares M, Sweeney M, Stultz J, Newman M, Smith V, et al. Tooth whitening: Tooth color changes following treatment by peroxide and light. J Clin Dent. 2005;16:78–82. [PubMed] [Google Scholar]
- 24.Palmer DA. The definition of a standard observer for mesopic photometry. Vision Res. 1967;7:619–28. doi: 10.1016/0042-6989(67)90070-3. [DOI] [PubMed] [Google Scholar]
- 25.Hein DK, Ploeger BJ, Hartup JK, Wagstaff RS, Palmer TM, Hansen LD. In-office vital tooth bleaching - what do lights add? Compend Contin Educ Dent. 2003;24:340–52. [PubMed] [Google Scholar]
- 26.Zhang C, Wang X, Kinoshita J, Zhao B, Toko T, Kimura Y, et al. Effects of KTP laser irradiation, diode laser and LED on tooth bleaching: A comparative study. Photomed Laser Surg. 2007;25:91–5. doi: 10.1089/pho.2006.2025. [DOI] [PubMed] [Google Scholar]
- 27.Tavares M, Stultz J, Newman M, Smith V, Kent R, Carpino E, et al. Light augments tooth whitening with peroxide. J Am Dent Assoc. 2003;134:167–75. doi: 10.14219/jada.archive.2003.0130. [DOI] [PubMed] [Google Scholar]
- 28.Gurgan S, Cakir FY, Yazici E. Different light-activated in-office bleaching systems: A clinical evaluation. Lasers Med Sci. 2010;25:817–22. doi: 10.1007/s10103-009-0688-x. [DOI] [PubMed] [Google Scholar]
- 29.Torres CR, Barcellos DC, Batista GR, Borges AB, Cassiano KV, Pucci CR. Assessment of the effectiveness of light-emitting diode and diode laser hybrid light sources to intensify dental bleaching treatment. Acta Odontol Scand. 2011;69:176–81. doi: 10.3109/00016357.2010.549503. [DOI] [PubMed] [Google Scholar]
- 30.Domínguez A, García JA, Costela A, Gómez C. Influence of the light source and bleaching gel on the efficacy of the tooth whitening process. Photomed Laser Surg. 2011;29:53–9. doi: 10.1089/pho.2009.2751. [DOI] [PubMed] [Google Scholar]
- 31.Kossatz S, Dalanhol AP, Cunha T, Loguercio A, Reis A. Effect of light activation on tooth sensitivity after in-office bleaching. Oper Dent. 2011;36:251–7. doi: 10.2341/10-289-C. [DOI] [PubMed] [Google Scholar]
- 32.Hahn P, Schondelmaier N, Wolkewitz M, Altenburger MJ, Polydorou O. Efficacy of tooth bleaching with and without light activation and its effect on the pulp temperature: An in vitro study. Odontology. 2013;101:67–74. doi: 10.1007/s10266-012-0063-4. [DOI] [PubMed] [Google Scholar]
- 33.D’Arce MB, Lima DA, Aguiar FH, Ambrosano GM, Munin E, Lovadino JR. Evaluation of ultrasound and light sources as bleaching catalysts: An in vitro study. Eur J Esthet Dent. 2012;7:176–84. [PubMed] [Google Scholar]
- 34.Al Quran FA, Mansour Y, Al-Hyari S, Al Wahadni A, Mair L. Efficacy and persistence of tooth bleaching using a diode laser with three different treatment regimens. Eur J Esthet Dent. 2011;6:436–45. [PubMed] [Google Scholar]
- 35.Kugel G, Papathanasiou A, Williams AJ, 3rd, Anderson C, Ferreira S. Clinical evaluation of chemical and light-activated tooth whitening systems. Compend Contin Educ Dent. 2006;27:54–62. [PubMed] [Google Scholar]
- 36.Bernardon JK, Sartori N, Perdigão J, Ballarin A, Lopes GC, Baratieri LN. Clinical performance of vital bleaching techniques. Oper Dent. 2010;35:3–10. doi: 10.2341/09-008CR. [DOI] [PubMed] [Google Scholar]
- 37.He LB, Shao MY, Tan K, Xu X, Li JY. The effects of light on bleaching and tooth sensitivity during in-office vital bleaching: A systematic review and meta-analysis. J Dent. 2012;40:644–53. doi: 10.1016/j.jdent.2012.04.010. [DOI] [PubMed] [Google Scholar]
- 38.Nutter BJ, Sharif MO, Smith AB, Brunton PA. A clinical study comparing the efficacy of light activated in-surgery whitening versus in-surgery whitening without light activation. J Dent. 2013;41:e3–7. doi: 10.1016/j.jdent.2013.03.004. [DOI] [PubMed] [Google Scholar]
- 39.Polydorou O, Wirsching M, Wokewitz M, Hahn P. Three-month evaluation of vital tooth bleaching using light units: A randomized clinical study. Oper Dent. 2013;38:21–32. doi: 10.2341/12-041-C. [DOI] [PubMed] [Google Scholar]
- 40.Liang S, Sa Y, Jiang T, Ma X, Xing W, Wang Z, et al. In vitro evaluation of halogen light-activated vs chemically activated in-office bleaching systems. Acta Odontol Scand. 2013;71:1149–55. doi: 10.3109/00016357.2012.757355. [DOI] [PubMed] [Google Scholar]
- 41.Henry RK, Bauchmoyer SM, Moore W, Rashid RG. The effect of light on tooth whitening: A split-mouth design. Int J Dent Hyg. 2013;11:151–4. doi: 10.1111/j.1601-5037.2012.00568.x. [DOI] [PubMed] [Google Scholar]
- 42.Bruzell EM, Johnsen B, Aalerud TN, Dahl JE, Christensen T. In vitro efficacy and risk for adverse effects of light-assisted tooth bleaching. Photochem Photobiol Sci. 2009;8:377–85. doi: 10.1039/b813132e. [DOI] [PubMed] [Google Scholar]
- 43.Browning WD, Swift EJ., Jr Critical appraisal. Power bleaching. J Esthet Restor Dent. 2011;23:61–7. doi: 10.1111/j.1708-8240.2010.00390.x. [DOI] [PubMed] [Google Scholar]
- 44.Matis BA, Cochran MA, Franco M, Al-Ammar W, Eckert GJ, Stropes M. Eight in-office tooth whitening systems evaluated in vitro: A pilot study. Oper Dent. 2007;32:322–7. doi: 10.2341/06-135. [DOI] [PubMed] [Google Scholar]
- 45.Jones AH, Diaz-Arnold AM, Vargas MA, Cobb DS. Colorimetric assessment of laser and home bleaching techniques. J Esthet Dent. 1999;11:87–94. doi: 10.1111/j.1708-8240.1999.tb00382.x. [DOI] [PubMed] [Google Scholar]
- 46.Amengual Lorenzo J, Cabanes Gumbau G, Cervera Sanchez C, Forner Navarro L, Llena Puy MC. Clinical study of a halgon light activated bleaching agent in non-vital teeth: Case reports. Quintessence Int. 1996;27:383–8. [PubMed] [Google Scholar]
- 47.Gerlach RW, Zhou X. Vital bleaching with whitening strips: Summary of clinical research on effectiveness and tolerability. J Contemp Dent Pract. 2001;2:1–16. [PubMed] [Google Scholar]
- 48.Joiner A, Thakker G. In vitro evaluation of a novel 6% hydrogen peroxide tooth whitening product. J Dent. 2004;32:19–25. doi: 10.1016/j.jdent.2003.10.007. [DOI] [PubMed] [Google Scholar]
- 49.Nathoo S, Stewart B, Petrone ME, Chaknis P, Zhang YP, DeVizio W, et al. Comparative clinical investigation of the tooth whitening efficacy of two tooth whitening gels. J Clin Dent. 2003;14:64–9. [PubMed] [Google Scholar]
- 50.Kihn PW, Barnes DM, Romberg E, Peterson K. A clinical evaluation of 10 percent vs.15 percent carbamide peroxide tooth-whitening agents. J Am Dent Assoc. 2000;131:1478–84. doi: 10.14219/jada.archive.2000.0061. [DOI] [PubMed] [Google Scholar]
- 51.Heymann HO. Tooth whitening: Facts and fallacies. Br Dent J. 2005;198:514. doi: 10.1038/sj.bdj.4812298. [DOI] [PubMed] [Google Scholar]
- 52.Leonard RH, Sharma A, Haywood VB. Use of different concentration of carbamide peroxide for bleaching teeth: An in vitro study. Quintessence Int. 1998;29:503–7. [PubMed] [Google Scholar]
- 53.Matis BA, Mousa HN, Cochran MA, Eckert GJ. Clinical evaluation of bleaching agents of different concentrations. Quintessence Int. 2000;31:303–10. [PubMed] [Google Scholar]
- 54.Matis BA, Wang Y, Jiang T, Eckert GJ. Extended at-home bleaching of tetracycline-stained teeth with different concentrations of carbamide peroxide. Quintessence Int. 2002;33:645–55. [PubMed] [Google Scholar]