

Abstract
Background:
It is important that every member of our community should be trained in effective BLS technique to save lives. At least doctors including dental practitioners, and medical and paramedical staff should be trained in high quality CPR, as it is a basic medical skill which can save many lives if implemented timely.
Aim:
Our aim was to study the awareness of Basic Life Support (BLS) among dental students and practitioners in New Delhi.
Materials and Methods:
This cross sectional study was conducted by assessing responses to 20 selected questions pertaining to BLS among dental students, resident doctors/tutors, faculty members and private practitioners in New Delhi. All participants were given a printed questionnaire where they had to mention their qualifications and clinical experience, apart from answering 20 questions.
Statistical Analysis:
Data was collected and evaluated using commercially available statistical package for social sciences (SPSS version 12).
Results:
One hundred and four responders were included. Sadly, none of our responders had complete knowledge about BLS. The maximum mean score (9.19 ± 1.23) was obtained by dentists with clinical experience between 1-5 years.
Conclusion:
To ensure better and safer healthcare, it is essential for all dental practitioners to be well versed with BLS.
Keywords: Basic life support, cardiopulmonary arrest, dental practitioners
INTRODUCTION
Cardiopulmonary arrest (CPA) is a sudden cessation of effective respiration or circulation, excluding patients of chronic diseases and terminal malignancies.[1] The American Heart Association advocates a “chain of survival” for all victims needing cardiopulmonary resuscitation (CPR) including-early recognition of a victim, early CPR, rapid defibrillation, effective advanced life support and integrated post-cardiac arrest care. Amongst these, the first three steps constitute what is known as basic life support (BLS), a key component, which improves the chances of survival following cardiac arrest. As the central nervous system can undergo irreversible damage within 3-4 min of hypoxia or anoxia, early and effective BLS, including defibrillation can greatly improve the chances of survival.[2]
It is important that every member of our community should be trained in effective BLS technique to save lives. At least doctors, including dental practitioners, and medical and paramedical staff, should be trained in high quality CPR, as it is a basic medical skill, which can save many lives if implemented timely. In the United States, BLS training has been recommended for all health-care professionals from as early as 1966.[3] In our country, though it is increasingly becoming a part of teaching curriculum of medical students, awareness about the correct technique amongst dental practitioners is still questionable.
AIM
Our aim was to study the awareness of BLS among dental students and practitioners in New Delhi.
MATERIALS AND METHODS
This cross-sectional study was conducted by assessing responses to 20 selected questions pertaining to BLS among dental students, resident doctors/tutors, faculty members, and private practitioners in New Delhi. All participants were given a printed questionnaire where they had to mention their qualifications and clinical experience, apart from answering 20 questions. The questions covered various aspects of BLS including abbreviations of BLS andAED (automated external defibrillator) assessment of patients, resuscitation techniques, use of defibrillators and recognizing and managing victims of stroke, electrocution, road traffic accidents, and myocardial infarction. Those who were not willing to participate or returned incomplete questionnaires were excluded from the study.
Statistical analysis
Data was collected and evaluated using commercially available statistical package for social sciences (SPSS version 12). Descriptive and frequency analysis was made for counts, percentage and mean as appropriate.
RESULTS
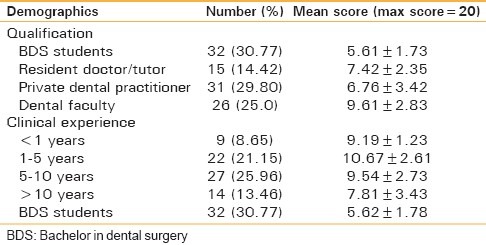
One hundred and four responders were included and out of these, 26 (25%) were faculty members, 15 (14.42%) were resident doctors/tutors, 31 (39.80%) were private dental practitioners and the rest 32 (30.77%) were dental (bachelor in dental surgery) students [Table 1].
Table 1.
Various characteristics of participants
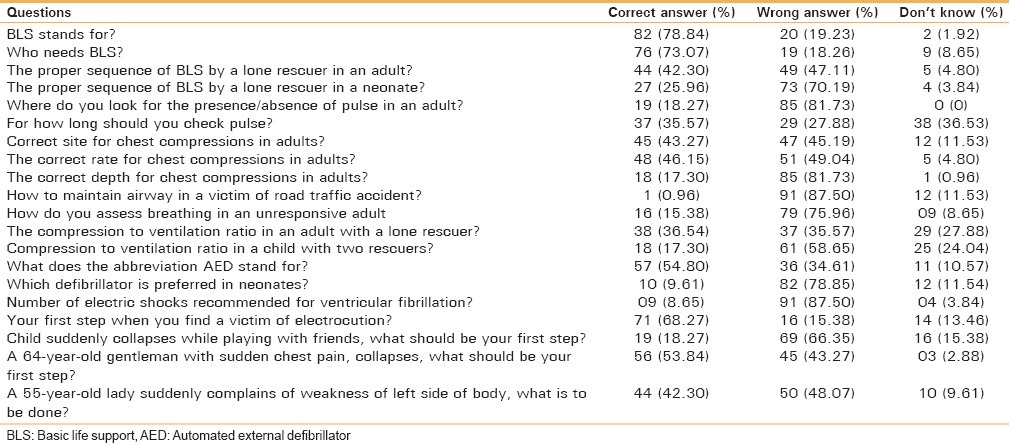
Sadly, none of our responders had complete knowledge about BLS. Seventy eight per cent of the responders knew that BLS stands for basic life support [Table 2]. Seventy three per cent could correctly assess who needed BLS among four case scenarios. The latest guidelines by AHA (American Heart Association) recommend the correct sequence for CPR in an adult as C-A-B (chest compressions, airway, breathing). Less than half of our responders (42.3%) knew this correct sequence. Only 25.96% of the responders knew the correct sequence in neonates (A-B-C). Surprisingly, only 18.27% of responders knew the correct location to check for pulse (either carotid), though 35.57% knew that the pulse should be palpated for more than 5 s but less than 10 s. Forty three per cent of the responders knew the correct site (lower one third of sternum), and 48% knew the correct rate of chest compressions (at least 100 per min). Only one responder knew that airway in a victim of trauma or road traffic accident should be maintained by jaw thrust only. Only 15.38% of responders knew how to assess breathing in an unconscious victim (look only for presence/absence of normal breathing). The correct ratio for chest compression and ventilation in an adult victim (30:2) was answered correctly by 36.54% of responders whereas, 58.65% of the responders did not know the correct ratio in a child with two rescuers (15:2). Fifty four per cent of the responders were aware of what the abbreviation AED stands for (automated external defibrillator) but 87.5% did not know that only one electric shock is now recommended as a treatment for ventricular fibrillation. Sixty eight per cent of the responders knew that when trying to rescue a victim of electrocution, the first step is to ensure scene safety. More than two thirds of the responders did not know that the first step to take when a child suddenly collapses is to administer rescue breaths rather than activating emergency medical services (EMS). More than half of our responders were aware that when an elderly gentleman collapses after complaining of chest pain, the first step is to activate EMS. Forty two percent of the responders did not suspect stroke in a middle aged lady suddenly complaining of weakness of one side of the body.
Table 2.
Basic life support knowledge of the participants
Looking closely at the individual groups, it was observed that the maximum mean score (9.19 ± 1.23) was obtained by dentists with clinical experience between 1 years and 5 years, being fresh with their knowledge. The minimum mean score was obtained by BDS students (5.62 ± 1.78), emphasising on the need to include BLS in their curriculum [Table 1].
DISCUSSION
Life threatening emergencies can occur anytime and anywhere. The most urgent of all is CPA. There have been reports of CPA and deaths in dental clinics.[4,5,6] Though many dentists claim that they have never witnessed CPA, the lack of training and incompetence to deal with these emergencies can have tragic and legal consequences.[4]
There are only few studies on the competence of dental practitioners to resuscitate patients from CPA.[7] However, the common factor in all is an inadequate awareness and knowledge among dentists regarding BLS and CPR.
In a survey conducted by Singh et al. among 241 dentists regarding CPR and observed that though 75.9% of dentists had received information about CPR, 56.0% had the correct concept of performing it, and only 12% had received practical training in BLS.[8] In our study, none of the responders could answer all questions correctly and none had received any formal training.
In a study to evaluate the knowledge of CPR among dentists in Iran, it was noted that only 37% had a correct concept of BLS and CPR. None of them had received any practical training, though 4% admitted that they had witnessed CPA in their clinics.[9]
Girdler et al. found the total prevalence of all emergency events (excluding syncope) was 0.7 cases per dentist per year. Only 20.8% of dentists felt competent to diagnose the cause of a collapse in the dental surgery. However, the majority believed that they would be able to undertake initial treatment of most common emergencies. Despite this, more than 50% felt they were unable to manage a patient of myocardial infarction or anaphylaxis, and 49.7% did not know how to insert an oral airway or undertake an intravenous injection.[10] Chapman and Hussain reported that none of the dental practitioners they evaluated had the practical skills to perform quality CPR.[11,12] Arsati et al. in 2010 found that though the occurrence of life-threatening medical emergencies like anaphylaxis, myocardial infarction, cardiac arrest, and cerebrovascular accident is rare in Brazilian dental clinics, dentists are not fully prepared to manage medical emergencies and have insufficient experience training in CPR.[13]
Theoretical knowledge with practical demonstrations and regular practice with up to date recommendations is essential in maintaining the competence of BLS providers. Future post-graduate training in emergency care for dentists needs to be more accurately targeted to the known prevalence of emergencies and deficiencies in dentists’ emergency skills.
Our study showed that BLS skills are highly lacking among dentists. It is now essential to include this in the teaching curriculum of all medical, dental, nursing, and paramedical curricula. When these people are trained, then only can they spread awareness among general public about the facts of BLS.
Limitations
We could only assess the theoretical knowledge of responders. Practical skills could not be evaluated.
CONCLUSION
Dentistry is a specialised branch and has made immense progress. To ensure better and safer health-care, it is essential for all dental practitioners to be well versed with BLS. Not only BLS, other basic procedures such as use of emergency resuscitation equipment and drugs (AMBU (artificial manual breathing unit) bag, laryngoscope, drugs such as adrenaline and atropine) are highly desirable.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Russo AC, Nogueira DP, Ribeiro IJ, Lane JC, Martins JE, Carvalho JG. Pertubações causadas por agentes físicos. In: Gonçalves EL, Oliveira HL, Kieffer L, Germek AO, Pereira VG, editors. Manual De Clínica Médica. 1st ed. Rio de Janeiro: Guanabara Koogan; 1980. pp. 1533–57. [Google Scholar]
- 2.Sasson C, Rogers MA, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest: A systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3:63–81. doi: 10.1161/CIRCOUTCOMES.109.889576. [DOI] [PubMed] [Google Scholar]
- 3.Cardiopulmonary resuscitation: A statement by the Ad Hoc Committee on Cardiopulmonary Resuscitation of the Division of Medical Sciences, National Academy of Sciences, National Research Council. Cardiopulmonary Resuscitation. AMA. 1966;198:372–9. [Google Scholar]
- 4.Brahams D. Death in the dentist's chair. Lancet. 1989;2:991–2. doi: 10.1016/s0140-6736(89)91007-6. [DOI] [PubMed] [Google Scholar]
- 5.Hunter PL. Cardiac arrest in the dental surgery. Br Dent J. 1991;170:284. doi: 10.1038/sj.bdj.4807511. [DOI] [PubMed] [Google Scholar]
- 6.McCarthy FM. Emergencias en Odontología. Buenos Aires: WB Saunders; 1972. pp. 281–92. [Google Scholar]
- 7.Chapman PJ. Medical emergencies in dental practice and choice of emergency drugs and equipment: A survey of Australian dentists. Aust Dent J. 1997;42:103–8. doi: 10.1111/j.1834-7819.1997.tb00104.x. [DOI] [PubMed] [Google Scholar]
- 8.Singh K, Bhat N, Nagaraappa R, Sharda A, Asawa K, Agarwal A, et al. Cardiopulmonary resuscitation: Knowledge and personal experience among dentists in Udaipur, India. J Dental Sci. 2011;6:72–5. [Google Scholar]
- 9.Kavari SH, Chohedri AH. Cardiopulmonary resuscitation: Knowledge and personal experience in Iranian dentists. Pak J Med Sci. 2007;23:296–7. [Google Scholar]
- 10.Girdler NM, Smith DG. Prevalence of emergency events in British dental practice and emergency management skills of British dentists. Resuscitation. 1999;41:159–67. doi: 10.1016/s0300-9572(99)00054-4. [DOI] [PubMed] [Google Scholar]
- 11.Chapman PJ. A questionnaire survey of dentists regarding knowledge and perceived competence in resuscitation and occurrence of resuscitation emergencies. Aust Dent J. 1995;40:98–103. doi: 10.1111/j.1834-7819.1995.tb03123.x. [DOI] [PubMed] [Google Scholar]
- 12.Hussain I, Matthews RW, Scully C. Cardiopulmonary resuscitation skills of dental personnel. Br Dent J. 1992;173:173–4. doi: 10.1038/sj.bdj.4807987. [DOI] [PubMed] [Google Scholar]
- 13.Arsati F, Montalli VA, Flório FM, Ramacciato JC, da Cunha FL, Cecanho R, et al. Brazilian dentists’ attitudes about medical emergencies during dental treatment. J Dent Educ. 2010;74:661–6. [PubMed] [Google Scholar]