

Abstract
Purpose
To describe early macular hole (MH) development in rhegmatogenous retinal detachment (RRD) after scleral buckling (SB) based on optical coherence tomography (OCT) findings.
Methods
The medical records and spectral domain OCT images of patients in whom MH developed after RRD repair were evaluated retrospectively.
Results
A postoperative MH was detected in five eyes that underwent SB during a 6-year period. All had fovea-off RRD without MH at the time of surgery. OCT showed partial loss of the inner retina with a preserved photoreceptor layer in early postoperative days. On average, 7 days (range,5 to 8 days) after surgery, outer retinal tissues disappeared, resulting in the full-thickness MH.
Conclusions
Serial OCT findings revealed that partial-thickness lamellar holes progressed to full-thickness MHs, which were formed by the degeneration of the outer retina in eyes with preceding loss of the glial cone in the fovea.
Keywords: Retinal perforations, Rhegmatogenous retinal detachment, Scleral buckling
The pathogenesis of idiopathic full-thickness macular holes (MHs) was proposed as tangential vitreofoveal traction by Gass [1]. Optical coherence tomography (OCT) depicted anteroposterior vitreous traction from perifoveal posterior vitreous detachment (PVD), which is considered the main mechanism for idiopathic MHs [2,3,4,5,6,7,8,9]. Meanwhile, several studies reported secondary or atypical MH development after scleral buckling (SB) for rhegmatogenous retinal detachment (RRD) [10,11,12,13,14]. They suggested several theories, including posterior vitreous separation, macular traction from the persistently attached posterior cortical vitreous, and microcytic degeneration of macula. However, the pathogenesis of secondary MH development after retinal detachment (RD) repair has remained unclear. In this study, we investigated and described the process of MH formation in RRD after SB based on serial OCT images.
Materials and Methods
This is a retrospective case series, including RRD patients who developed a new full-thickness MH after successful SB at Pusan National University Hospital in Korea. Patients were informed of all aspects of the procedure, and all patients provided written informed consent. The study was conducted in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. The institutional review board of Pusan National University Hospital waived approval, which is common practice for retrospective studies.
Patients who had concomitant MH with RD at presentation were excluded. Absence of MH was confirmed with ophthalmoscopy examination before and/or during surgery. The operations were performed by three vitreoretinal surgeons (ISB, SWP, and JEL). Cryoretinopexy was performed in all patients at the time of surgery. Subretinal fluid drainage and intravitreal injection of gas were performed at the surgeons' discretion.
The collected clinical data included age, gender, spherical equivalent, lens status, and axial length. The characteristics of RD were reviewed regarding foveal involvement, extension of detachment, location of breaks, and time to MH diagnosis. Development of MH was diagnosed with a biomicroscope and confirmed by spectral domain OCT (Cirrus HD-OCT, Carl Zeiss Meditec, Dublin, CA, USA; Spectralis, Heidelberg Engineering, Heidelberg, Germany). Serial OCT images were reviewed to analyze the process of MH formation.
Results
Among 927 eyes that underwent SB for primary RRD, MH developed in five eyes after surgery. The incidence was 0.54%. The mean age of the patients was 56.0 ± 6.8 years (range, 50 to 67 years). The fovea was detached in all five eyes (Figs. 1,2,3,4,5). Three of them were phakic, and two were highly myopic eyes with an axial length of 26 mm or more. No one, however, had chorioretinal atrophy masking the presence of a preoperative MH.
Fig. 1.

Fundus photograph and optical coherence tomography obtained from patient 1. (A) Fundus photograph showed superior bullous rhegmatogenous retinal detachment with fovea-off. (B) Optical coherence tomography scan on the second postoperative day. Outer retinal tissue (arrow) and residual fluid were seen on the fovea. Retinal cleavage (arrowhead) at the level of the external limiting membrane, perifoveal elevation, and intraretinal edema (yellow arrowhead) were detected. (C) Day 8. The outer retinal tissue of the fovea was gone and a full-thickness macular hole developed. Fine precipitates and sheddings (yellow arrows) were found on the base and wall of the hole. An intraretinal cyst (yellow arrowhead) remained.
Fig. 2.

Fundus photograph and optical coherence tomography obtained from patient 2. (A) Fundus photograph showed fovea-off rhegmatogenous retinal detachment and myopic crescent. Weiss ring (arrow) was visible. (B) Optical coherence tomography scan on the second postoperative day. Outer retinal tissue (arrow) of the fovea with low signal, and residual fluid (yellow arrowhead) at the temporal macula were seen. Retinal cleavage (arrowhead) also was detected at the level of the external limiting membrane. (C) Day 5. Subretinal fluid and retinal tissue disappeared, which resulted in a full-thickness macular hole with a flat edge.
Fig. 3.

Fundus photograph and optical coherence tomography obtained from patient 3. (A) Fundus photograph showed bullous rhegmatogenous retinal detachment with fovea-off. (B) Optical coherence tomography scan on the first postoperative day. The perifovea was edematous. Outer retinal tissue (arrow) of the fovea with a low signal, and cleavage (arrowheads) at the level of external limiting membrane were detected. (C) Day 7. The outer retinal tissue of the fovea (arrow) was more diminished, and perifoveal elevation decreased. The cleavage (arrowheads) was remained. (D) Day 10. The outer retinal tissue disappeared, and a full-thickness macular hole with fine precipitates and sheddings (yellow arrows) on the base and wall of the hole were detected.
Fig. 4.

Fundus photograph and optical coherence tomography obtained from patient 4. (A) Fundus photograph showed fovea-off rhegmatogenous retinal detachment. (B) Postoperative day 8. Retinal cleavage (arrowhead) and outer retina tissue or precipitate-like materials (arrow) were detected with residual fluids (yellow arrowhead). (C) Postoperative day 15. Retinal tissues diminished further at the fovea, forming a full-thickness macular hole with perifoveal edema. Precipitate was seen on the lateral wall of hole (arrow). Subretinal fluid (yellow arrowhead) was remained.
Fig. 5.

Fundus photograph and optical coherence tomography obtained from patient 5. (A) Fundus photograph shows superior bullous rhegmatogenous retinal detachment with fovea-off. (B) Postoperative day 6. Retinal cleavage (arrowhead) and foveal tissues (arrow), which looked like a macular hole with a flat edge, were seen faintly. (C) Twenty-five months after rhegmatogenous retinal detachment repair, a full-thickness macular hole and perifoveal edema were found. Precipitate-like material was seen on the lateral wall of the hole (arrow).
Three underwent segmental SB with silicone sponge, and two received encircling with a silicone rubber band. Subretinal fluid drainage was performed in all five eyes. Two (patient 2 and 5) received intravitreal gas injection at the end of the operation. MHs were diagnosed 7.0 ± 1.4 days (range, 5 to 8 days) on average after SB. The patients' characteristics were summarized in Table 1.
Table 1.
Patient characteristics
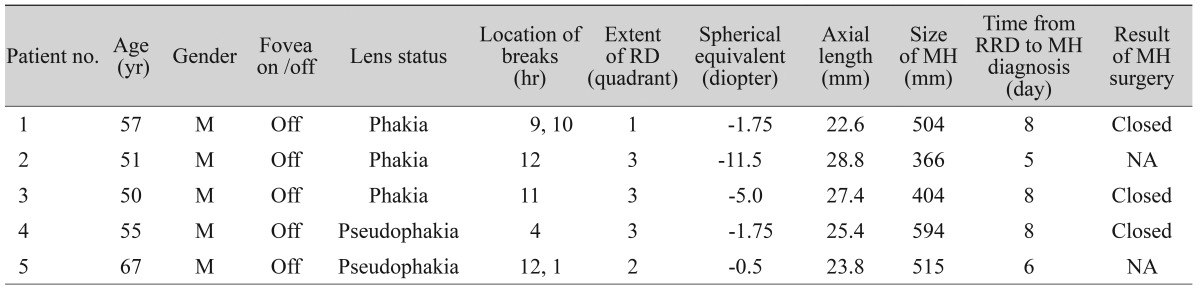
RD = retinal detachment; MH = macular hole; RRD = rhegmatogenous retinal detachment; NA = not applicable.
Spectral domain OCT images demonstrated that common features of a secondary MH after SB differed from those with idiopathic MH. In all of the eyes studied, the fovea appeared to have lamellar holes with loss of the inner retinal tissue before a full-thickness MH developed. The shape was that of a full-thickness MH except for the presence of a membranous tissue at the hole base, which was thought to be the degenerating photoreceptor layer. The outer retina seemed to be cleaved at the external limiting membrane (ELM) (Figs. 1B, 2B, and 3B). Within several days, the outer retinal tissue disappeared and all of the eyes rapidly advanced to a full-thickness MH. In two eyes, this development was accompanied with the resolution of submacular fluid. The mean diameter of holes was as large as 474.6 ± 90.6 mm. The operculum was not seen in all eyes on the OCT images.
In three patients, the MH was closed successfully after vitrectomy, internal limiting membrane removal, and gas tamponade. Two patients refused additional treatment for their MHs.
Selected case reports
1) Patient 1
A 57-year-old man had a superior bullous RRD with fovea-off in the right eye (Fig. 1A). His vision was counting fingers. SB, cryoretinopexy, and drainage of subretinal fluid were performed. Retinal reattachment was achieved successfully. The OCT image of the second postoperative day revealed a lamellar hole with perifoveal elevation and intraretinal cystic changes. The outer retinal tissue bulged due to residual f luid at the fovea. Moreover, the outer retinal layer was cleaved at the level of the ELM (Fig. 1B). On day 8, the outer retinal tissue of the fovea disappeared and a full-thickness MH developed as large as 504 mm with precipitates found on the base (Fig. 1C). The MH was closed after vitrectomy, internal limiting membrane peeling, and gas tamponade. Vision was 20 / 200 3 months after MH surgery.
2) Patient 2
A 51-year-old man presented with fovea-off RRD and myopic crescent in his left eye. Weiss ring was clearly visible (Fig. 2A). The retina was reattached by scleral encircling, cryoretinopexy, and drainage of subretinal f luid. Intraocular gas was injected to manage the fish-mouth phenomenon at the end of surgery. Two days after RRD repair, a lamellar hole with residual subretinal fluid was seen on the OCT scan. The outer retina of the lamellar hole showed a relatively low signal. Retinal cleavage was detected at the level of the ELM (Fig. 2B). On day 5, the resolution of the subretinal fluid was accompanied with an extinction of the outer retinal tissue, thereby resulting in a full-thickness MH with a flat edge (Fig. 2C). The size of the hole was 366 mm.
3) Patient 3
A 50-year-old man had superior bullous RD with fovea-off in the right eye (Fig. 3A). Vision was 20 / 400 at presentation. Successful retinal reattachment was achieved after encircling, cryoretinopexy, and drainage of subretinal fluid. OCT scan detected a lamellar hole with low-signaling outer retinal tissue and cleavage at the level of the ELM the day after surgery (Fig. 3B). As time passed, the outer retinal tissue of the fovea diminished (Fig. 3C), and a full-thickness MH developed on day 8. Its diameter was 404 mm, and precipitates were noted on the base of the hole (Fig. 3D). The hole was closed after MH surgery, but his vision remained 20 / 400 with no further improvement.
Discussion
This study presented five eyes with a lamellar hole in the early postoperative days and the development of a full-thickness MH by progressive disappearance of the outer retinal tissue approximately 1 week after RRD repair with SB. The lamellar hole had a cleft appearance at the level of the ELM. Several additional common characteristics were found. Despite the fast formation of MHs, the mean size was greater than 400 mm. No vitreomacular traction, retinal roof of fovea, or operculum were detected. All had fovea-off RRD at presentation. These findings suggest that MH in RRD developed not only from the vitreo-foveal detachment, but also from a combined mechanism affecting the inner and the outer retina.
The development of idiopathic MH was reportedly originally attributed to anteroposterior vitreous traction from perifoveal PVD occurring with the introduction of the OCT scan [2,3,4,5,6,7,8,9]. This can cause an intraretinal split evolving into cystic space, and then to the disruption of the outer retinal layer and the opening of the fovea, thus constituting a full-thickness MH. Previous studies for a secondary or atypical MH after SB for RRD also postulated that persistent vitreo-macula attachment involving the fovea present at the time of RRD repair could develop into a full-thickness MH with the separation of the vitreo-fovea attachment [10,11,12,13,14]. This mechanism, however, was not supported by OCT scans showing the formation of MH after RRD repair.
There were several proposed explanations for non-typical MH formation. Some studies suggested that other factors, such as microcystic degeneration and hydration of retinal tissue, influenced hole formation in secondary MHs and some idiopathic MHs [10,15,16,17]. Brown [10] suggested that foveal ischemia, resulting from separation between fovea and choroidal circulation, could induce secondary MH after RRD repair.
Delayed formation of a MH between 8 weeks to 2 years after PVD was reported [16,17]. Further, it was proposed that traction-induced inner foveal damage occurring before or coincident with spontaneous vitreofoveal separation destabilized the fovea and predisposed some eyes to delayed MH formation. Yamada [18] reported that an inverted cone-shaped zone of Müller cells (Müller cell cone), whose base corresponded with the internal limiting membrane and whose apex corresponded with the outer limiting membrane centrally, composed the floor of the fovea and served as a plug, binding together receptor cells in the foveola (Fig. 6A). Without this plug of glial cells, the retinal receptor cell layer would be highly susceptible to disruption at the umbo and to hole formation under a variety of circumstances, including sensory RD, minor trauma, cystoid macular edema, and macular degeneration [19]. Because of this foveal anatomy, loss of the Müller cell cone by PVD could contribute to inner retinal dehiscence and result in delayed full-thickness MH formation.
Fig. 6.
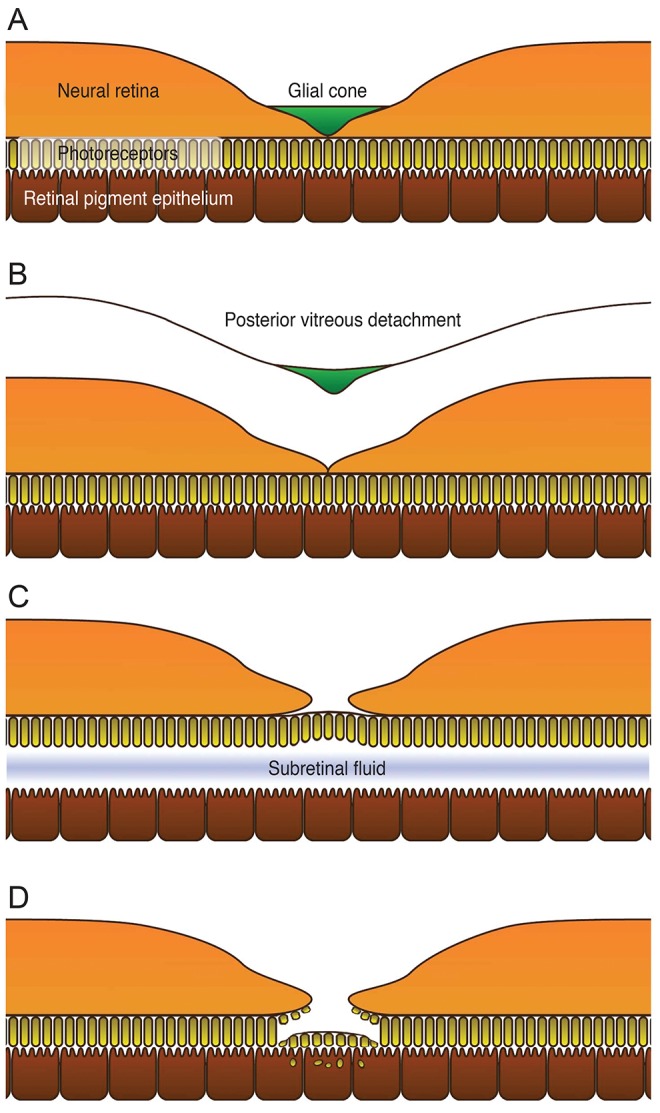
Schematic representation of macular hole formation in fovea-off rhegmatogenous retinal detachment after repair. (A) Before posterior vitreous detachment, the glial cone is intact and supports the structure of the fovea. (B) The glial cone is removed during posterior vitreous detachment, and the fovea is compromised. (C) Fovea-off rhegmatogenous retinal detachment induces outer retinal ischemia due to deprivation of diffusion from choroidal circulation. The external limit ing membrane provides temporary stability for the separated photoreceptors. (D) Finally, despite reattachment of the retina, degeneration of photoreceptors continues, resulting from the absorption of subretinal fluid and phagocytosis of the degenerated photoreceptors to accelerate development of a full-thickness macular hole.
Based on the above mechanism and our findings, we suggest that three factors may be related to the early development of MH in RRD after SB. The schematic representation is presented in Fig. 6. First, the inner retina is damaged due to pre-existing PVD. A glial cone is removed with PVD and the fovea is compromised, making it more susceptible to MH formation (Fig. 6B). Next is the degeneration of the outer retina due to neurosensory RD. The detached outer retina degrades due to deprivation of nutrition and oxygen perfusion from the choroid to the retina. The photoreceptor layer then separates at the ELM, which provides weak but temporary stability (Fig. 6C). The last step is the degeneration and phagocytosis of the damaged photoreceptors. After reattachment of the retina, the separated photoreceptors are apposed to the retinal pigment epithelium. The retinal pigment epithelium then absorbs the subretinal fluid and phagocytoses the degenerated photoreceptors to accelerate formation of a full-thickness MH (Fig. 6D).
Previous studies for MH complications in RRD were consistent with our results. The age of the patients was between 50 and 60 years, and the majority of them had a fovea-off RRD [10,12,13,19,20,21]. The holes were large [12,19,20]. Secondary MH formation after RRD repair is a rare condition [10,12,13], and the incidence has been unclear so far. A summary of previous studies and ours are presented in Table 2. However, intervals between SB and MH diagnosis varied. Some studies reported that the time to diagnose a MH was several weeks [10,13,20,21], and others reported over several months after SB [12,14,19]. The difference in the time to diagnosis for MH may result from the fovea status, such as severity of ischemic damage according to the duration of foveal detachment at the time of RRD repair. Differences in postoperative follow-up intervals also could influence the time to detect MH after surgery. Moreover, different mechanisms may exist for late MH formation.
Table 2.
Characteristics of previous studies for secondary MHs after SB
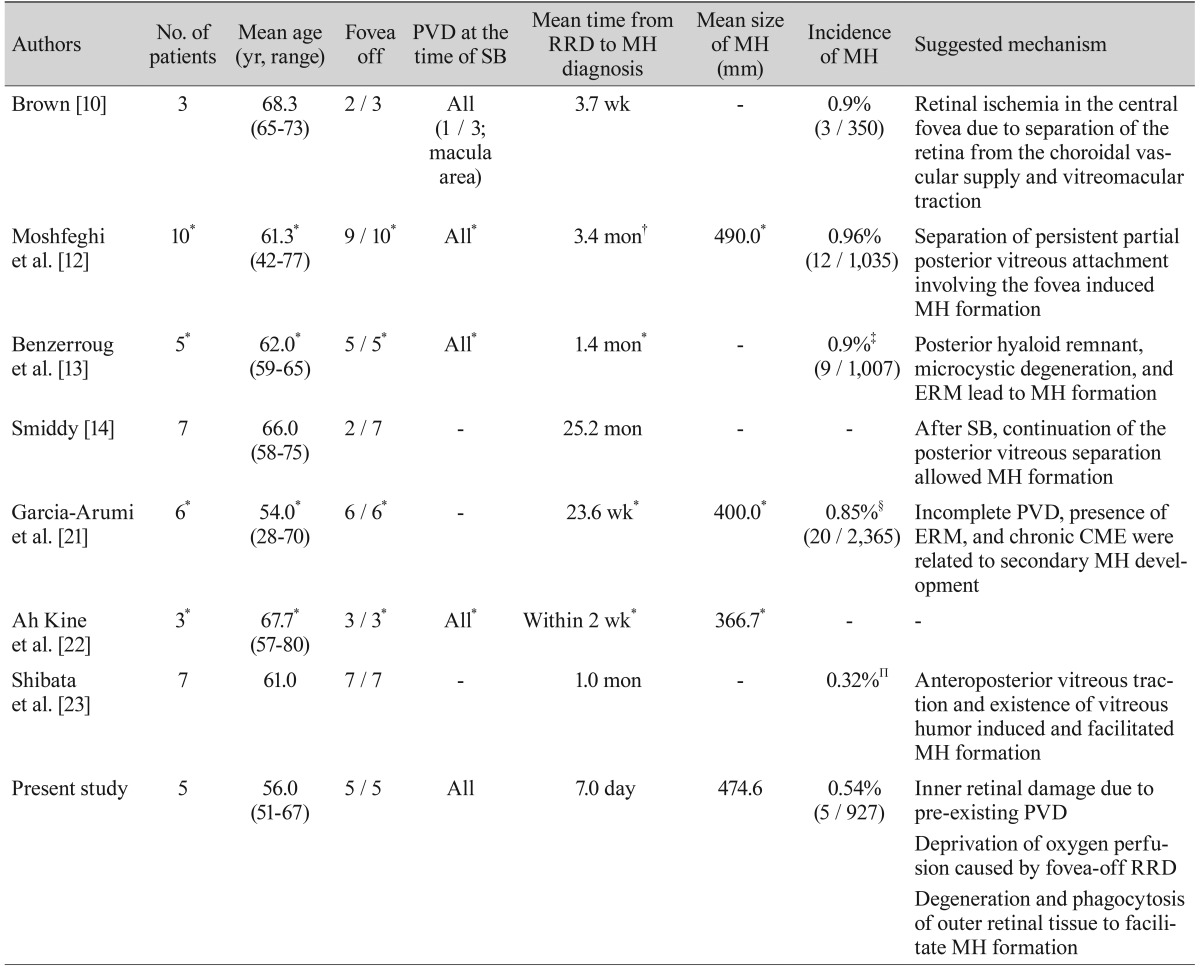
MH = macular hole; SB = scleral buckling; PVD = posterior vitreous detachment; RRD = rhegmatogenous retinal detachment; ERM = epiretinal membrane; CME = cystoid macular edema.
*Cases of SB only from original data; †Median value of time; ‡Included all types of SB, vitrectomy, and pneumatic retinopexy; §Included both SB and vitrectomy with encircling; ΠIncluded all types of SB, vitrectomy, and SB with vitrectomy.
Our study has limitations in that it was a retrospective study and the sample size was small. The MH incidence of 0.54% in the current study might be inaccurate, as preoperative and postoperative OCT scans were not obtained in all the eyes. Although it would be difficult to determine the presence of preoperative MH, especially in eyes with high myopia or macular folding. In these cases, there was little chance to miss any preoperative MHs due to careful fundus examination during and after surgery, as well as early postoperative OCT scans showing a preserved outer retina. Moreover, this study demonstrated the process of secondary MH formation in fovea-off RRD by means of serial spectral domain OCT images from lamellar hole to full-thickness MH development.
In summary, full-thickness MH can develop during the early postoperative period in fovea-off RRD after SB. Combined damage to the inner retina due to pre-existing PVD and to the outer retina by ischemia leads to the development of secondary MH. OCT examination is recommended for early detection and intervention.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Gass JD. Reappraisal of biomicroscopic classification of stages of development of a macular hole. Am J Ophthalmol. 1995;119:752–759. doi: 10.1016/s0002-9394(14)72781-3. [DOI] [PubMed] [Google Scholar]
- 2.Gaudric A, Haouchine B, Massin P, et al. Macular hole formation: new data provided by optical coherence tomography. Arch Ophthalmol. 1999;117:744–751. doi: 10.1001/archopht.117.6.744. [DOI] [PubMed] [Google Scholar]
- 3.Smiddy WE, Flynn HW., Jr Pathogenesis of macular holes and therapeutic implications. Am J Ophthalmol. 2004;137:525–537. doi: 10.1016/j.ajo.2003.12.011. [DOI] [PubMed] [Google Scholar]
- 4.Johnson MW. Posterior vitreous detachment: evolution and complications of its early stages. Am J Ophthalmol. 2010;149:371–382. doi: 10.1016/j.ajo.2009.11.022. [DOI] [PubMed] [Google Scholar]
- 5.Haouchine B, Massin P, Gaudric A. Foveal pseudocyst as the first step in macular hole formation: a prospective study by optical coherence tomography. Ophthalmology. 2001;108:15–22. doi: 10.1016/s0161-6420(00)00519-4. [DOI] [PubMed] [Google Scholar]
- 6.Ito Y, Terasaki H, Suzuki T, et al. Mapping posterior vitreous detachment by optical coherence tomography in eyes with idiopathic macular hole. Am J Ophthalmol. 2003;135:351–355. doi: 10.1016/s0002-9394(02)01944-x. [DOI] [PubMed] [Google Scholar]
- 7.Takahashi A, Nagaoka T, Ishiko S, et al. Foveal anatomic changes in a progressing stage 1 macular hole documented by spectral-domain optical coherence tomography. Ophthalmology. 2010;117:806–810. doi: 10.1016/j.ophtha.2009.09.022. [DOI] [PubMed] [Google Scholar]
- 8.Takahashi A, Yoshida A, Nagaoka T, et al. Idiopathic full-thickness macular holes and the vitreomacular interface: a high-resolution spectral-domain optical coherence tomography study. Am J Ophthalmol. 2012;154:881–892. doi: 10.1016/j.ajo.2012.05.024. [DOI] [PubMed] [Google Scholar]
- 9.Yeh PT, Chen TC, Yang CH, et al. Formation of idiopathic macular hole-reappraisal. Graefes Arch Clin Exp Ophthalmol. 2010;248:793–798. doi: 10.1007/s00417-009-1297-x. [DOI] [PubMed] [Google Scholar]
- 10.Brown GC. Macular hole following rhegmatogenous retinal detachment repair. Arch Ophthalmol. 1988;106:765–766. doi: 10.1001/archopht.1988.01060130835034. [DOI] [PubMed] [Google Scholar]
- 11.Boscia F, Recchimurzo N, Cardascia N, et al. Macular hole following conventional repair of bullous retinal detachment using air injection (D-ACE procedure) Eur J Ophthalmol. 2004;14:572–574. doi: 10.1177/112067210401400621. [DOI] [PubMed] [Google Scholar]
- 12.Moshfeghi AA, Salam GA, Deramo VA, et al. Management of macular holes that develop after retinal detachment repair. Am J Ophthalmol. 2003;136:895–899. doi: 10.1016/s0002-9394(03)00572-5. [DOI] [PubMed] [Google Scholar]
- 13.Benzerroug M, Genevois O, Siahmed K, et al. Results of surgery on macular holes that develop after rhegmatogenous retinal detachment. Br J Ophthalmol. 2008;92:217–219. doi: 10.1136/bjo.2007.122796. [DOI] [PubMed] [Google Scholar]
- 14.Smiddy WE. Atypical presentations of macular holes. Arch Ophthalmol. 1993;111:626–631. doi: 10.1001/archopht.1993.01090050060029. [DOI] [PubMed] [Google Scholar]
- 15.Tornambe PE. Macular hole genesis: the hydration theory. Retina. 2003;23:421–424. doi: 10.1097/00006982-200306000-00028. [DOI] [PubMed] [Google Scholar]
- 16.Smiddy WE. Macular hole formation without vitreofoveal traction. Arch Ophthalmol. 2008;126:737–738. doi: 10.1001/archopht.126.5.737. [DOI] [PubMed] [Google Scholar]
- 17.Besirli CG, Johnson MW. Traction-induced foveal damage predisposes eyes with pre-existing posterior vitreous detachment to idiopathic macular hole formation. Eye (Lond) 2012;26:792–795. doi: 10.1038/eye.2012.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yamada E. Some structural features of the fovea centralis in the human retina. Arch Ophthalmol. 1969;82:151–159. doi: 10.1001/archopht.1969.00990020153002. [DOI] [PubMed] [Google Scholar]
- 19.Gass JD. Muller cell cone, an overlooked part of the anatomy of the fovea centralis: hypotheses concerning its role in the pathogenesis of macular hole and foveomacualr retinoschisis. Arch Ophthalmol. 1999;117:821–823. doi: 10.1001/archopht.117.6.821. [DOI] [PubMed] [Google Scholar]
- 20.Tsuboi S, Taki-Noie J, Emi K, Manabe R. Fluid dynamics in eyes with rhegmatogenous retinal detachments. Am J Ophthalmol. 1985;99:673–676. doi: 10.1016/s0002-9394(14)76034-9. [DOI] [PubMed] [Google Scholar]
- 21.Garcia-Arumi J, Boixadera A, Martinez-Castillo V, et al. Macular holes after rhegmatogenous retinal detachment repair: surgical management and functional outcome. Retina. 2011;31:1777–1782. doi: 10.1097/IAE.0b013e31820a69c3. [DOI] [PubMed] [Google Scholar]
- 22.Ah Kine D, Benson SE, Inglesby DV, Steel DH. The results of surgery on macular holes associated with rhegmatogenous retinal detachment. Retina. 2002;22:429–434. doi: 10.1097/00006982-200208000-00006. [DOI] [PubMed] [Google Scholar]
- 23.Shibata M, Oshitari T, Kajita F, et al. Development of macular holes after rhegmatogenous retinal detachment repair in Japanese patients. J Ophthalmol. 2012;2012:740591. doi: 10.1155/2012/740591. [DOI] [PMC free article] [PubMed] [Google Scholar]