

Abstract
The treatment of coronary chronic total occlusions (CTO) continues to solicit technical innovations. As success primarily depends on crossing the lesion with a wire, all aspects regarding tip shape retention, torque precision, and penetration ability of the guide-wire have greatly influenced new techniques and strategies. The world of interventional cardiology has to look carefully at these developments, and to use them accordingly to improve the success rate in ordinary percutaneous coronary interventions. We present a didactical case report of a CTO revascularization treated with a new ‘dual core’ technology guide-wire.
Keywords: Chronic total occlusion, PCI, Drug-eluting stent, Antegrade approach
Introduction
Coronary chronic total occlusion (CTO) represents a challenge for the interventional cardiologist [1–4]. Indeed, CTO is characterized by technical and procedural complexities and a relatively low rate of procedural success in comparison with percutaneous coronary interventions (PCI) in other non-CTO lesions.
In order to find technical solutions to improve results of PCI in CTO, intracoronary guide-wires probably represent the most important class of devices. The recent onset of so-called ‘composite core, dual coil’ guide-wires can be considered an absolute turning point. The following is a didactic case report to illustrate this concept.
Case report
A 66-year-old male, ex-smoker, with mild hypertension and dyslipidemia, was admitted to our department with stable angina (Canadian Cardiovascular Society classification 3). He underwent exercise stress test, which was positive. Segmental regional wall motion was normal at 2D-echocardiogram. A coronary angiography revealed a CTO of the proximal left anterior descending (LAD) coronary artery, with ipsilateral bridge collaterals and faint epicardial contralateral collateralization from the right coronary artery. Fig. 1A shows a blunt stump type CTO of the LAD, uncertainly placed around the vessel, sharing into a septal and a diagonal branch. The opacification of LAD was ‘type 2’, according to the Rentrop and Cohen classification (Fig. 1B) [5]. Although the occlusion appeared to be short, the retrograde filling was helpful enough to identify a reliable entry point. Considering the anatomy of the occlusion, we tried to use an intravascular ultrasound (IVUS) probe in order to correctly identify the entry point of LAD CTO. However, due to proximal calcification, we were not able to advance the IVUS probe in mid LAD. At this stage, before going through a retrograde approach, an antegrade probing was attempted using an additional Fielder XT-A wire (Asahi Intecc Co., Ltd.) (Fig. 2) [6].
Figure 1.
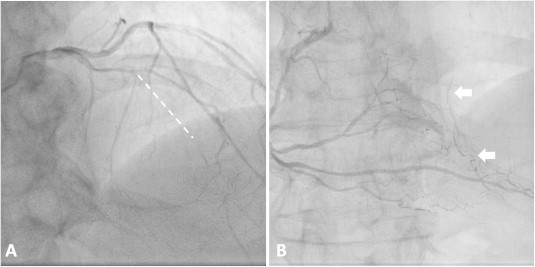
Baseline angiographic images: (A) cranial angiographic view of left coronary artery system showing the chronic total occlusion (CTO) of anterior descending (LAD). The proximal tortuosity of LAD and spot calcifications (white arrows), which present just upstream to the emergence of a septal and a diagonal branch, did not allow the advancement of intravascular ultrasound probe in order to identify the CTO’s entry-point. (B) Cranial left anterior oblique view of right coronary angiography showing the faint contralateral collateralization for distal LAD (arrows).
Figure 2.
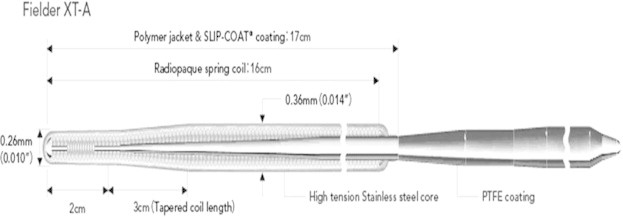
Fielder XT-A (Asahi Intecc Co., Ltd.) characteristics [6]. Polymer sleeve provides excellent trackability and lubricity even in absence of stump. The ‘composite core’ construction provides excellent tip durability and torque performance with smooth passage, enhancing crossability.
The rationale for such a choice was based on a unique combination of guide-wire characteristics which include a precise guide-tip shape retention and a fine transmission to the tip of any degree of external rotation. Moreover, a 0.010″ tip tapering enhances penetration into an eventual plaque micro-fracture. Finally, the hydrophilic characteristics facilitate the sliding motion along the lesion. Precisely oriented (Fig. 3), the guide-wire was able to reach the distal true lumen of LAD, thereby greatly simplifying the procedure. After progressive lesion dilation, the procedure was completed by the implantation of two everolimus-eluting stents (Abbott Vascular Xience Prime, Santa Clara, CA) (2.75 × 28 mm and 3.0 × 24 mm, respectively) crossing over the bifurcation with the diagonal branch. After the final stent expansion and modeling performed by kissing balloon inflation between LAD and the diagonal branch, the full vessel opacification revealed an unusual and confusing anatomy of the vessel with a septal branch originating from the diagonal (Fig. 4). Angiographic success was obtained, and the patient was discharged two days after the procedure. No events were observed at six months of clinical follow-up.
Figure 3.
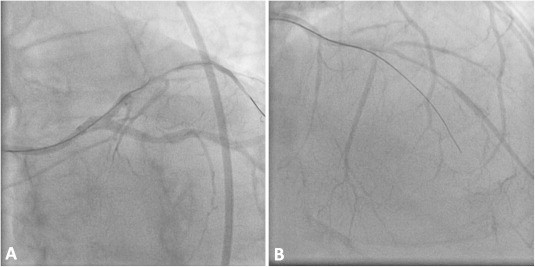
Left anterior descending chronic total occlusion revascularization procedure: (A) caudal left anterior oblique view showing the orientation of Fielder XT-A guide wire through the proximal cap of LAD CTO. (B) Cranial angiographic view of left coronary artery system showing the advancement of Fielder XT-A into LAD with the gain of distal true lumen.
Figure 4.

Final result after two everolimus-eluting stents.
Discussion
There are innovative solutions to overcome the difficulties encountered in percutaneous CTO treatment. In case of proximal cap blunt stump, recommendations are made to resort to IVUS images in order to precisely identify it and address the efforts for a subintimal-guided penetration [7]. In our case, this option was not available due to a calcification located upstream of the obstruction (Fig. 1A – arrow), hindering the IVUS probe crossing. Any pre-dilation at this stage could have induced plaque modifications, thus possibly further compromising chances for an antegrade wire penetration. Moreover, the retrograde approach was difficult due to poor retrograde collateralization.
In the field of intracoronary guide-wires, the so-called plastic wires, which are as lubricous as the hydrophilic wires, can reduce friction and greatly facilitate the crossing of coronary occlusions. However, their tips do not easily retain their shapes and, especially if tapered, they are not precisely addressable towards a specific direction. This is easier with the so-called hydrophobic guides, thanks to a spring coil layer at the tip. For both, the transmission of external rotations to the tip occurs in steps, with torque whips. An almost ideal innovation, first introduced with the Sion guide-wires (Asahi Intecc Co., Ltd.) [8]. is obtained by paralleling a classic linear core with another, formed by twisted wires, joined at the tip (‘composite core’), which allows a more gradual tip rotation. With the Fielder XT guide-wires family, such a characteristic is combined with diversifications of tip weight and tapering. Moreover, the insertion of a rope-coil at the tip, inside a classic spring-coil (‘dual coil’), permits a fine and durable shaping, which fully integrates with the classic easy sliding, typical of hydrophilic guides [9]. Using this guide-wire family, it is easily possible to cross CTO towards invisible micro-channels, as we showed in our case, or to perform the recently described mini-STAR technique in case of conventional approach failure [10]. New dual coil core guide-wires, such as the Gaia guide-wire series, were specifically developed for CTO crossings, allowing better torque control and maneuverability. The initial use of such guide-wires could have provided easier and faster angiographic success in the case reported here.
Conclusion
It is of utmost importance to follow developments in the construction of materials dedicated to CTO percutaneous revascularization. The new Fielder ‘composite core, dual coil’ guide-wire family allows better orientation insight into the coronary artery and a high penetration capacity, which improves the chance of success.
Conflict of interest
We have no conflict of interest to declare.
Footnotes
Peer review under responsibility of King Saud University.

References
- 1.Sianos G., Werner G.S., Galassi A.R., Papafaklis M.I., Escaned J., Hildick-Smith D. Recanalisation of chronic total coronary occlusions: 2012 consensus document from the EuroCTO club. EuroIntervention. 2012;8(1):139–145. doi: 10.4244/EIJV8I1A21. [DOI] [PubMed] [Google Scholar]
- 2.Galassi A.R., Tomasello S.D., Costanzo L., Campisano M.B., Barrano G., Tamburino C. Long-term clinical and angiographic results of sirolimus-eluting stent in complex coronary chronic total occlusion revascularization: the SECTOR registry. J Interv Cardiol. 2011;24(5):426–436. doi: 10.1111/j.1540-8183.2011.00648.x. [DOI] [PubMed] [Google Scholar]
- 3.Galassi A.R., Tomasello S.D., Crea F., Costanzo L., Campisano M.B., Marzá F. Transient impairment of vasomotion function after successful chronic total occlusion recanalization. J Am Coll Cardiol. 2012;59(8):711–718. doi: 10.1016/j.jacc.2011.10.894. [DOI] [PubMed] [Google Scholar]
- 4.Stojkovic S., Sianos G., Katoh O., Galassi A.R., Beleslin B., Vukcevic V. Efficiency, safety, and long-term follow-up of retrograde approach for CTO recanalization: initial (Belgrade) experience with international proctorship. J Interv Cardiol. 2012;25(6):540–548. doi: 10.1111/j.1540-8183.2012.00754.x. [DOI] [PubMed] [Google Scholar]
- 5.Galassi AR., Tomasello SD., Khamis H. Collateral circulation in CTO. In: Waksman R., Saito S., editors. Chronic total occlusions: a guide to recanalization. Wiley-Blackwell; 2013. pp. 9–17. [Google Scholar]
- 6.Website. http://www.asahi-intecc.com.
- 7.Galassi A.R., Tomasello S.D., Costanzo L., Tamburino C. Anterograde techniques for percutaneous revascularization of chronic total coronary occlusions. Interv Cardiol. 2010;2(3):377–390. [Google Scholar]
- 8.Galassi AR., Ganyukov V., Tomasello SD., Haes B., Leonid B. Successful antegrade revascularization by the innovation of composite core dual coil in a three-vessel total occlusive disease for cardiac arrest patient using extracorporeal membrane oxygenation (ECMO) Eur Heart J. 2014 doi: 10.1093/eurheartj/ehu070. Feb 26. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 9.Tomasello S.D., Marzà F., Giubilato S., Galassi A.R. Retrograde approach for revascularization of coronary chronic total occlusion. Minerva Cardioangiol. 2012;60(5):461–472. [PubMed] [Google Scholar]
- 10.Galassi A.R., Tomasello S.D., Costanzo L., Campisano M.B., Barrano G., Ueno M. Mini-STAR as bail-out strategy for percutaneous coronary intervention of chronic total occlusion. Catheter Cardiovasc Interv. 2012;79(1):30–40. doi: 10.1002/ccd.22998. [DOI] [PubMed] [Google Scholar]