

Abstract
Preliminary evidence supports the role of emotion-related deficits in generalized anxiety disorder (GAD), including heightened emotional intensity, poor understanding of emotion, negative cognitive reactivity to emotions, and maladaptive emotion management. However, questions remain concerning the specificity of these emotion-related deficits compared to highly comorbid conditions such as social anxiety disorder (SAD). In the current study, 113 undergraduate students were administered measures of GAD, SAD, and emotion-related factors in order to clarify relationships among these variables. In univariate analyses, presence of SAD did not significantly impact the association between GAD and the emotion-related measures. Further, a discriminant function analysis revealed that emotional intensity and impaired regulation strategies provided the greatest discrimination between groups and best predicted a diagnosis of GAD (regardless of SAD comorbidity). Although their discriminatory ability was weaker, poor emotional understanding best predicted a diagnosis of SAD (regardless of GAD comorbidity), and non-acceptance of emotions best predicted comorbid GAD and SAD.
Keywords: Generalized anxiety disorder, Social phobia, Comorbidity, Emotion, Emotion dysregulation, Emotion regulation
Unlike other anxiety disorders, GAD lacks overt markers, such as behavioral avoidance of recurrent objects or situations as in specific or social phobias. Rather, symptoms occur primarily internally, thus making them difficult to observe. However, establishing worry as its central feature has improved both understanding and reliability of GAD (Mennin, Turk, & Heimberg, 2004). Delineation of the function of worry has shown the most promise in furthering our understanding of the disorder. Borkovec's avoidance theory (e.g., Borkovec, Alcaine, & Behar, 2004) posits that worry in GAD serves to decrease aversive imagery and physiological hyperarousal associated with negative emotion. Evidence for this conceptualization of worry in GAD has been found in a number of studies which demonstrate that worry is verbal–linguistic, as opposed to imagery-based, and during worry physiological arousal appears to be invariable on indices of heart rate and skin conductance. Borkovec and colleagues extrapolate from these findings that the worry process may become negatively reinforced by the reduction of autonomic arousal (Borkovec et al., 2004).
The avoidance function of worry may best be explained by the perceived aversive nature of emotional experience in GAD patients. When asked about reasons for worrying, individuals with GAD were distinguished from non-anxious controls by the greater likelihood to endorse that they engaged in worry to avoid thinking about more emotional topics (Borkovec & Roemer, 1995). An important question then is why individuals with GAD want to avoid emotional experience. One possibility may result from the nature of how emotions are generated and regulated (Gross, 1998). The relationship of emotional deficits to psychopathology has received increasing attention (e.g., Kring & Bachorowski, 1999). Much of this work has focused upon the functional role of emotions and has drawn considerably from findings in the basic affect sciences (Ekman & Davidson, 1994).
Mennin, Heimberg, Turk, and Fresco (2005) have proposed that GAD is characterized by significant deficits in emotional experience and regulation. In particular, they argue that individuals with GAD have difficulties in four components of emotion functioning. Specifically, individuals with GAD experience emotions with heightened intensity compared to persons without GAD. Second, individuals with GAD experience marked difficulties identifying, describing, and clarifying their emotional experiences (i.e., poor understanding). Third, they are prone to greater negative cognitive reactivity to emotions by holding catastrophic beliefs about the consequences of both negative and positive emotions and endorsing more difficulty attending to and allowing emotional experience to unfold. Fourth, individuals with GAD struggle to manage or soothe themselves when they experience negative emotions (i.e., maladaptive management). Within this model, maladaptive emotion management strategies in GAD can be classified either as difficulties modulating emotional experiences or as maladaptive attempts to control or suppress emotional experience.
Empirical evidence supports this theoretical perspective on GAD. An initial series of studies provided a test of this model (Mennin et al., 2005). In the first study, college students with and without GAD (assessed by self-report) were compared on their responses to a battery of measures assessing aspects of emotion. GAD participants reported increased intensity, poorer clarity, greater negative reactivity, and poorer management of emotions compared to control individuals (Study 1). In a follow-up study, these findings were replicated with a clinical sample of individuals who had received a primary diagnosis of GAD (Mennin et al., 2005; Study 2). In a third study, GAD students underwent a mood induction. Following a negative mood induction, control participants were able to report more acceptance of these emotions, greater clarity of feeling, and greater belief that they were able to change their mood state than participants with GAD (Mennin et al., 2005; Study 3). Evidence also suggests that specific regulation deficits, including diminished access to effective regulation strategies and poor ability to engage in goal-pursuit behavior when distressed, are associated with GAD and chronic worrying (Salters-Pedneault, Roemer, Tull, Rucker, & Mennin, 2006). In addition, Mennin et al. (2005; Studies 1 and 2) found that emotion-related deficits predicted a diagnosis of GAD above the effects of worry, anxiety and depression.
Despite this preliminary support for the emotion regulation perspective on GAD, Turk, Heimberg, Luterek, Mennin, and Fresco (2005) found that a number of these deficits were not specific to GAD. Individuals with GAD reported greater emotion intensity and negative reactivity to sad emotions than individuals with SAD and non-anxious controls; however, individuals with SAD indicated being less expressive of positive emotions, paying less attention to their emotions, and having more difficulty describing their emotions than individuals with GAD or non-anxious controls. Thus, emotion deficits may not be entirely specific to this disorder, and may characterize other forms of psychopathology such as social anxiety disorder (SAD). Similar to these findings, other investigators (Salovey, Stroud, Woolery, & Epel, 2002) have also shown a link between SAD and deficiencies in emotion regulatory ability.
The present study sought to extend the findings reported in previous work examining emotion-related deficits in GAD and SAD (Turk et al., 2005). A number of limitations regarding the Turk et al. (2005) paper suggest further investigation is warranted. First, participants did not undergo diagnostic interviews to confirm the diagnosis; rather, a self-report measure was used to identify an analogue sample. In this study, we used a structured clinical interview to ascertain diagnoses. Second, GAD and SAD commonly co-occur (12-month prevalence tetrachoric correlation = .47; Kessler, Chiu, Demler, & Walters, 2005). Thus, it is important to delineate emotion-related deficits in a comorbid group compared to non-comorbid GAD and SAD groups (as well as non-anxious individuals). Third, given that the measures of emotion intensity and management used in the Turk et al. study were not designed to denote dysfunction, the inclusion of instruments that have previously been utilized in clinical populations may provide more generalizable results.
The primary goals of this study were to examine reported differences in emotion intensity, understanding, attendance and acceptance, and regulation strategies among individuals with generalized anxiety disorder (GAD), social anxiety disorder (SAD), their co-occurrence, or neither condition. We hypothesized that GAD participants (regardless of co-occurring SAD), when compared to individuals with SAD (without GAD) or control participants, would report experiencing: (1) greater emotion intensity; (2) poorer understanding of their emotions; (3) greater negative cognitive reactivity as indexed by more difficulty attending to (i.e., awareness) and accepting emotions, and (4) maladaptive management of emotions as indexed by a difficulty in accessing effective regulatory strategies. We also hypothesized that emotion-related deficits, particularly emotional intensity, would better predict a diagnosis of GAD (with or without SAD) than SAD, in a discriminant function analysis.
1. Method
1.1. Participants
Undergraduate students at a northeastern university responded to recruitment efforts in an introductory psychology course or through campus-posted flyers and participated for payment. All participants were administered the GAD and SAD sections of the Anxiety Disorders Interview Schedule-IV (ADIS-IV; Di Nardo & Barlow, 1994) to confirm eligibility. ADIS-IV interviewers were upper-level graduate students who had been trained specifically in a year-long psychopathological diagnostic assessment seminar taught by the first author. Participants meeting criteria for GAD or SAD were invited to participate in the study. Participants who did not meet criteria for GAD or SAD and who scored below a 3 on a Clinician's Severity Rating of distress and impairment (CSR; range of 0–8 with a 4 denoting clinically significant symptom severity; Di Nardo & Barlow, 1994) due to worry or social anxiety were invited to participate in the study as control participants.
Thirty-one participants met criteria for GAD without SAD (9 male, 22 female), 18 participants met criteria for GAD and SAD (6 male, 12 female), 20 participants met criteria for SAD alone (6 male, 14 female) and 44 participants were classified as controls (18 male, 26 female). All diagnoses used to form groups were primary (CSR ≥ 4). Further, secondary diagnoses of GAD and SAD were not allowed in the SAD and GAD only groups, respectively. However, other disorders were allowed as secondary diagnoses as long as they were deemed to be of lesser severity (at least 1 CSR point below primary disorder). The mean age of the sample was 21.28 years (SD = 4.01) and was evenly distributed across the four groups without significant differences. Participants' self-reported race/ethnicity was as follows: 54.86% Caucasian (N=62), 16.81% African-American (N= 19), 7.96% Hispanic/Latino (N= 9), 13.27% Asian/Pacific Islander (N= 13), and 2.65% Middle Eastern descent (N = 2) and 4.42% (N = 5) declined to report this information. Ethnic background was equally distributed in study groups.
1.2. Procedure and measures
Participants who met criteria consented to participate in the study received the ADIS interview and then completed the Affect Intensity Measure (AIM; Larson & Deiner, 1987) and the Difficulties with Emotion Regulation Scale (DERS; Gratz & Roemer, 2004). Participants were then debriefed and paid $15 for participation in the study.
The AIM (Larson & Deiner, 1987) is a 40-item measure that assesses the intensity and reactivity in which respondents typically experience positive and negative emotions. The 10-item subscale, AIM-N, designed to assess the intensity of negative emotional experiences was used in this study. Participants indicate how often they experience specific emotional reactions to situations using a 6-point scale, where 1 is never, 2 is almost never, 3 is occasionally, 4 is usually, 5 is almost always, and 6 is always. Larson and Deiner (1987) report a test–retest reliability of .81 for the AIM after a 3-month interval. Internal consistency is high for the AIM (.90 ≤ α ≤.94) and construct validity has been demonstrated in a number of samples (Goldsmith & Walters, 1989; Larson & Deiner, 1987).
The DERS (Gratz & Roemer, 2004) is a 39-item measure that assesses dispositional tendencies for emotion dysregulation along a number of dimensions, including awareness, clarity of emotional experience, acceptance of emotions, ability to engage in goal-directed behavior, refrain from impulsive behavior when experiencing negative emotions, and accessibility of effective emotion regulation strategies. Four of the six subscales were administered (a total of 25 items): lack of awareness of emotion, poor clarity of emotion (emotional understanding), non-acceptance of emotion, and poor ability to access effective emotion regulation strategies. Participants indicate how much each item applies to them on a 5-point scale ranging from 1, not at all, to 5, completely (higher scores denote greater dysregulation). Subscales of the DERS have been shown to have high internal consistency (α's higher than .80 for each subscale) and the total score has demonstrated good test–retest reliability (ρ = .88). The DERS has also demonstrated good construct and predictive validity as a whole as well as within the individual subscales (Gratz & Roemer, 2004).
1.3. Analytic plan
To examine group differences on the dependent measures, we conducted a series of univariate ANOVAs with group as a between-subjects factor and each of the emotion deficit outcomes as the dependent variables. If group differences were found, we conducted non-orthogonal contrasts to determine which groups were significantly different from one another. First, we conducted a contrast to determine whether there was a difference between GAD participants with and without a SAD diagnosis. Both GAD with SAD and GAD without SAD were then compared to participants with only SAD and to control participants. We also compared the SAD only group to the control group. A discriminant function analysis was then conducted to determine whether emotion variables would differentially predict groups. Discriminant function analysis successively identifies the linear combinations of variables (canonical discriminant functions) that maximize separation among groups (Duarte Silva & Stam, 1995).
2. Results
Correlations for the emotion-related outcome measures are displayed in Table 1. The AIM-NI, DERS non-acceptance, and DERS strategies subscales demonstrated strong relationships with each other (r's > .50). With the exception of the AIM-NI and DERS awareness subscale which were highly inversely correlated, the DERS clarity and DERS awareness demonstrated weaker relationships with the other study variables but correlated highly with each other.
Table 1.
Pearson correlations among emotion measures.
| 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|
| 1. AIM-NI | – | ||||
| 2. DERS clarity | .16 | – | |||
| 3. DERS awareness | −.79 | .59** | – | ||
| 4. DERS non-acceptance | .40** | .34** | .28* | – | |
| 5. DERS strategies | .57** | .27* | .13 | .52** | – |
Note: AIM-NI denotes the Affect Intensity Measure, Negative Intensity Subscale; DERS denotes the Difficulties in Emotion Regulation Scale.
p < .01.
p < .001.
Emotion measure subscale scores for each group are displayed in Table 2.
Table 2.
Means and standard deviations on emotion measures for GAD (with and without SAD), SAD only, and control participants.
| Measure | GAD + SAD | GAD–SAD | SAD | CONTROL |
|---|---|---|---|---|
| AIM-NI | 3.99 (.15) | 3.92 (.11) | 3.48 (.14) | 3.01 (.10) |
| DERS | ||||
| Clarity | 2.59 (.17) | 2.28 (.13) | 2.31 (.16) | 1.94 (.11) |
| Awareness | 2.48 (.18) | 2.32 (.14) | 2.30 (.17) | 2.20 (.12) |
| Acceptance | 2.83 (.21) | 2.35 (.16) | 1.94 (.20) | 1.83 (.13) |
| Strategies | 2.53 (.10) | 2.29 (.13) | 2.00 (.16) | 1.62 (.11) |
Note: GAD + SAD denotes participants with both generalized anxiety disorder and social anxiety disorder, GAD−SAD denotes participants with generalized anxiety disorder but not social anxiety disorder, SAD denotes participants with only SAD, control denotes control participants. Higher scores on the DERS reflect greater emotion dysregulation.
2.1. Emotion intensity
Group differences were found on the AIM-NI subscale (F [3, 109] = 17.07, p< 0.001, η2 = 0.32). Using non-orthogonal contrasts, we first compared GAD with SAD and GAD without SAD and did not find a significant difference (CI: [−0.438, 0.304], p = .72, L = −.067). We then compared both GAD groups to the SAD and control groups. GAD with SAD participants reported higher scores on the AIM-NI subscale than SAD only (CI: [−0.914, −1.00], p < .05, L = −.507), or control participants (CI: [0.630, 1.331], p<.001, L = .980). GAD participants without SAD reported more intense negative emotions when compared with participants with SAD alone (CI: [0.081, 0.799], p < .05, L = .440), or the control group (CI [0.619, 1.207], p<.001, L = .913). Finally, individuals with only SAD also reported significantly greater intensity of negative emotions than control individuals (CI: [0.136, 0.811], p<.01, L = .473).
2.2. Emotion understanding
Differences were found between groups for the DERS clarity of emotions subscale, an index of poor emotional understanding (F [3, 109] = 4.02, p < 0.01, η2 = .01; Table 2). Non-orthogonal contrasts demonstrated that GAD with SAD and GAD without SAD groups did not differ on the DERS clarity of emotions subscale (CI: [−0.723, 0.113], p = .151, L = −0.305). GAD + SAD participants did not differ in DERS clarity scores compared to SAD only participants (CI: [−0.737, 0.179], p = .23, L = −.279) but demonstrated higher scores in comparison to controls [CI: (0.252, 1.042), p<.01, L = .647]. Similarly, GAD participants without SAD did not display poorer understanding of emotions than SAD only participants [CI: (−0.431, 0.378), p = .90, L = −.026] but did have significantly greater deficits in this index compared to controls (CI: [0.011, 0.673], p < .05, L= .342). Finally, the comparison between SAD only and control participants on DERS clarity scores did not reach significance (CI: [−.012, .748], p = .058, L = .368).
2.3. Emotion awareness and acceptance
No differences among the groups were found for scores on the DERS awareness of emotion subscale (F [3, 109] = 0.58, p = 0.631, η2 = .016). However, group differences emerged for DERS non-acceptance scores (F [3, 109] = 6.504, p < .001, η2 = 0.152; Table 2). Using non-orthogonal contrasts, the comparison between GAD with SAD and GAD without SAD participants on the DERS non-acceptance subscale did not reach significance (CI: [−0.992, 0.004], p = 0.067, L = −0.478). GAD with SAD participants reported greater DERS non-acceptance scores than SAD only participants, CI: (−1.451, −0.325), p<.01, L =−0.888) and control individuals (CI: [0.514, 1.483], p<.001, L = 0.998). In contrast, the GAD participants without SAD did not differ from SAD only participants on this measure (CI: [−0.087, 0.906], p<.01, L = 0.409) but did differ from controls (CI: [0.114, 0.926], p < .05, L = 0.520). The SAD only group, however, did not differ from controls on DERS non-acceptance subscales scores, CI: (−0.357, 0.578), p = .640, L = 0.110.
2.4. Emotion management
Differences among the groups were found for the DERS subscale, access to effective emotion regulation strategies (F (3, 109) = 9.611, p < .001, η2 = 0.209; Table 2). Using non-orthogonal contrasts, GAD with SAD and GAD without SAD participants did not differ on the ability to access to effective emotion regulation strategies (CI: [−0.643, 0.176], p = .262, L = −0.233). The GAD with SAD group displayed higher DERS strategies scores than SAD only (CI: [−0.977, −0.078], p < .05, L = −.528) or control (CI: [0.521, 1.295], p < .001, L = .908) participants. GAD without SAD participants did not significantly differ from SAD only participants (CI: [−0.102, 0.691], p = .14, L=.294) but did display higher DERS strategies subscales scores than control individuals (CI: [0.351, 0.999], p<.001, L = .675). Participants with only SAD also displayed higher DERS strategy scores than controls (CI: [0.008, 0.754], p < .05, L = .381).
2.5. Discriminant function analysis
Using, discriminant function analysis, three canonical discriminant functions containing the AIM-NI and the DERS subscales significantly discriminated the four diagnostic groups, Wilk's Λ = .589, χ2 (15, N= 113) = 56.94, p < .001. The first canonical function demonstrated the strongest discrimination among groups accounting for 91% of the variance (eigenvalue = .606, canonical r = .61) and had the highest absolute correlations (as determined by r's > .50) with the AIM negative intensity subscale (r = .83) and the DERS strategies subscale (r=.63). Only the DERS non-acceptance scale (r = .60) scale was highly correlated with the second canonical function, which accounted for 6% of the variance in discriminating among groups (eigenvalue = .037; canonical r=.19). Finally, only the DERS clarity scale displayed a strong correlation (r=−.61) with the third canonical function, which accounted for 3% of the variance in discriminating among groups (eigenvalue = .020; canonical r = .14).
Fig. 1 demonstrates the relationship of the four diagnostic groups with these functions by plotting the unstandardized canonical discriminant functions for each group in a discriminant space. The first function is plotted against the second function in Fig. 1a and the third function in Fig. 1b. As shown in Fig. 1a, the first function (vertical axis) best discriminates between those with and without GAD (regardless of SAD). Additionally, the second discriminant function (horizontal axis) is shown in Fig. 1a to be the primary contributor to the separation of the comorbid GAD with SAD group from the single anxiety disorder groups (i.e., GAD without SAD, SAD only). Finally, the third function (horizontal axis) displayed in Fig. 1b distinguishes those with SAD from those without SAD (regardless of GAD).
Fig. 1.
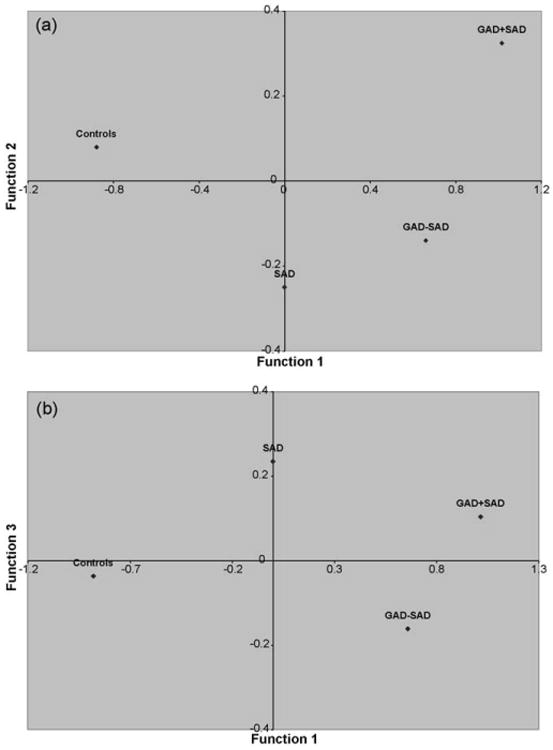
The mean scores of the two unstandardized canonical discriminant functions for the GAD groups with and without SAD, the SAD only group, and normal control group plotted in discriminant spaces of (a) Function 1 (vertical axis) × Function 2 (horizontal axis) and (b) Function 1 (vertical axis) × Function 3 (horizontal axis).
3. Discussion
The purpose of this study was to examine patterns of specificity in levels of emotion intensity, understanding, negative reactivity (i.e., lack of awareness, poor acceptance) and maladaptive management (i.e., difficulty accessing regulation strategies) in individuals with GAD, SAD, their co-occurrence, or neither condition. SAD did not significantly impact the link between these emotion variables and GAD but did itself show a relationship with a subset of these measures. When accounting simultaneously for all emotion variables and diagnostic groups, a discriminant function analysis revealed that emotion intensity and impaired regulation strategies accounted for the greatest differentiation between groups and best predicted a diagnosis of GAD (regardless of SAD comorbidity). Although their discriminatory ability was weaker, poor emotional understanding best predicted a diagnosis of SAD (regardless of GAD comorbidity), and non-acceptance of emotions best predicted GAD and SAD comorbidity.
Heightened intensity of emotions related most strongly to GAD in univariate group comparisons and in a discriminant function analysis. Turk and colleagues (2005) found a similarly specific relationship for heightened intensity of emotions using similar analyses. In a recent study, emotion intensity and maladaptive management uniquely predicted GAD beyond shared variance with MDD and SAD (Mennin, Holaway, Fresco, Moore, & Heimberg, 2007). Although linking heightened emotion intensity and GAD appears warranted, the specific nature of this intensity remains unclear. For instance, intensity of emotions may be a proxy for increased levels of neuroticism (i.e., underlying tendencies towards greater emotional reactivity) in GAD. GAD has been shown to have a strong genetic relationship with neuroticism (Hettema, Prescott, & Kendler, 2004). In contrast, SAD has not shown such a strong relationship with higher order neuroticism or negative affectivity factors (Watson, 2005). However, MDD is also strongly associated with these factors (Watson, 2005) but does not show a relationship with emotion intensity when GAD is taken into account (Mennin et al., 2007) and was not found to impact intensity levels of sadness reactivity in individuals with GAD who were induced to worry (McLaughlin, Mennin, & Farach, 2007).
Emotion intensity may not be pathological in itself. Indeed, one may cry at movies or become joyful at a dinner with friends without association to dysfunction (Kring & Bachorowski, 1999). Consistent with this non-pathological viewpoint, Mennin and colleagues (2007) found that heightened intensity did not load on a higher order emotion dysregulation factor, which included poor understanding, negative reactivity, and maladaptive management of emotions. One possibility is that heightened intensity increases the need for proper emotion management and that the subsequent deficiency in the latter skill may make individuals with GAD particularly susceptible to the effects of poor emotional responsiveness. In present analyses, as in the Mennin et al. (2007) study, both emotion intensity and maladaptive emotion management demonstrated strong and unique relationships with GAD when accounting for the presence of SAD. Although these results do not demonstrate a causal relationship, preliminary experimental research has supported the notion that individuals with GAD display greater dysregulation as a result of experiencing intense emotions (McLaughlin et al., 2007). Further, others have found that poor emotion regulatory ability mediates the effect of intensity on negative clinical outcomes (Lynch, Robins, Morse, & MorKrause, 2001).
Delineation of a strong link between GAD and poor ability to manage emotions does not preclude such a relationship with SAD. Indeed, univariate analyses in the present study demonstrate a significant relationship between SAD and difficulty accessing regulation strategies. Further, other investigations have shown a link between social anxiety and poor ability to manage emotions (Salovey et al., 2002; Turk et al., 2005). One possibility is that individuals with GAD may simply have more instances in which they experience heightened intensity and a need to enact emotion regulation strategies given the internally generated distress that is characteristic of the disorder. This can be contrasted with SAD where one may only need to enact these strategies when her or his emotional reactions are heightened in circumscribed social situations. Thus, the differential relationship between maladaptive emotion management and both GAD and SAD may be one of degree. Alternatively, the type of emotion management strategies that are dysfunctional in each of these disorders may differ. Difficulty accessing regulation strategies was one particular emotion management deficit explored in this study. Further research that delineates specific regulation strategies (e.g., expressive suppression; Gross, 1998) concurrently in both GAD and SAD are clearly necessary.
In contrast to emotion intensity and maladaptive management, poor understanding of emotions was found to be present in both GAD and SAD in the univariate analyses but slightly more characteristic of SAD in the discriminant function analysis. This result is consistent with previous work that found a unique relationship to SAD despite taking GAD co-occurrence into account through statistical control (Mennin et al., 2007) or group comparison (Turk et al., 2005). One way in which individuals increase their ability to understand their emotions is by reflecting their emotional states through interaction with others. If individuals with SAD are less likely to share their negative emotional reactions with others, they may subsequently have more difficulty understanding the significance of these emotional reactions. However, given that the strength of group discrimination by poor understanding was low, further research is clearly necessary to determine how important this variable is for explaining SAD phenomenology.
In this study, awareness and acceptance were used to signify negative cognitive reactions to emotions. Similar to previous studies (Mennin et al., 2005; Salters-Pedneault et al., 2006), no differences were found between GAD and control participants in reported attendance to emotional experience. SAD was also not related to this variable. This contrasts with Turk et al. (2005), who found that individuals with SAD paid less attention to emotions than those with GAD. One difficulty with this variable is that it is unclear whether greater or lesser attention to emotions is adaptive. Likely, both have merit given varying contexts. Thus, flexible awareness of emotions may be most adaptive by engendering acceptance and understanding of emotions but also permitting individuals to turn their attention away from emotional states as situations demand. Delineating situational determinants will help elucidate the role of emotion awareness in GAD and SAD. In contrast to awareness, difficulty in accepting emotions was found to be most characteristic of the comorbid GAD with SAD group in the univariate analyses and, to a lesser degree, in the discriminant function analysis. These results suggest that lack of emotional acceptance may be a non-specific feature of emotion dysregulation in the anxiety disorders. Indeed, emotion avoidance has been found to be an important factor in many anxiety disorders (Salters-Pedneault, Tull, & Roemer, 2004). Further, Hayes and colleagues (Hayes et al., 1996) have delineated the importance of “experiential avoidance” or an unwillingness to experience internal states such as emotion in many forms of psychopathology.
A number of limitations in the current study suggest these findings be interpreted with caution. First, student samples, even those meeting diagnostic criteria for a mental disorder, tend to be higher functioning than clinical samples. As such, these findings may not be generalizable to clinical samples of individuals with more severe GAD and SAD. However, despite the limitations inherent with student samples, all participants completed a well-validated structured interview to verify diagnosis. This represents a clear improvement on past studies examining emotion dysregulation in GAD in student populations (Turk et al., 2005). Nevertheless, future studies should examine the conditions under which individuals with GAD experience increased emotion dysregulation using clinical samples. Also, because the entire ADIS-IV was not administered, we were unable to determine the impact of disorders other than GAD and SAD and, thus, it is possible that differences between these groups could be attributed to additional comorbid conditions. A notable limitation of the present study was the exclusive reliance on self-report. It is possible that differences between groups may be a product of over-reporting emotional distress in GAD. One method for overcoming subjective report bias is to conduct a multimodal assessment of emotion including not only subjective elements but also expressive, psychophysiology, and neurobiological ones as well. Further investigations examining these components in GAD during emotion evocation are currently underway.
Overall, our findings are consistent with previous research that has documented greater emotional intensity and deficits in understanding, acceptance, and managing emotions in individuals with GAD (Mennin et al., 2005, 2007; Salters-Pedneault et al., 2006; Turk et al., 2005). Further, the present study demonstrates that levels of emotion intensity and dysregulation are not due solely to co-occurring social anxiety symptoms or increased levels of comorbidity. Specificity characteristics also emerged including a greater role for emotion intensity and maladaptive management in GAD and poor understanding in SAD. In contrast, lack of emotional acceptance may be a non-specific factor. Our results suggest directions for more fine-grained investigations. Experimental studies delineating the relationship of intensity and management in GAD and poor ability to utilize emotional knowledge in social settings among individuals with SAD would provide needed clarity in delineating mechanisms involved in these relationships. Although preliminary, the present findings provide initial evidence for the distinction of GAD and SAD in the role of various emotion-related deficits. Given further support, the delineation of emotion-related deficits in GAD and SAD may provide a fruitful direction for elucidating common and unique factors in the conceptualization and treatment of these disorders.
Contributor Information
Douglas S. Mennin, Email: doug.mennin@yale.edu.
Katie A. McLaughlin, Email: kmclaugh@hsph.harvard.edu.
References
- Borkovec TD, Alcaine O, Behar E. Avoidance theory of worry and generalized anxiety disorder. In: Heimberg RG, Turk CL, Mennin DS, editors. Generalized anxiety disorder: Advances in research and practice. New York: Guilford; 2004. pp. 77–108. [Google Scholar]
- Borkovec TD, Roemer L. Perceived functions of worry among generalized anxiety disorder subjects: Distraction from more emotionally distressing topics? Journal of Behavior Therapy and Experimental Psychiatry. 1995;26:25–30. doi: 10.1016/0005-7916(94)00064-s. [DOI] [PubMed] [Google Scholar]
- Di Nardo PA, Barlow DH. Anxiety disorders interview schedule for DSM-IV ADIS-IV. San Antonio, TX: Psychological Corporation; 1994. [Google Scholar]
- Duarte Silva AP, Stam A. Discriminant analysis. In: Grimm LG, Yarnold PR, editors. Reading and understanding multivariate statistics. Washington, DC: American Psychological Association; 1995. pp. 277–318. [Google Scholar]
- Ekman P, Davidson R. The nature of emotion: Fundamental questions. New York: Oxford University Press; 1994. [Google Scholar]
- Goldsmith RE, Walters H. A validity study of the Affect Intensity Measure. Journal of Social Behavior and Personality. 1989;4:133–140. [Google Scholar]
- Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and validation of the Difficulties with Emotion Regulation Scale. Journal of Psychopathology and Behavioral Assessment. 2004;26:41–54. [Google Scholar]
- Gross JJ. The emerging field of emotion regulation: An integrative review. Review of General Psychology. 1998;2:271–299. [Google Scholar]
- Hettema JM, Prescott CA, Kendler KS. Genetic and environmental sources of covariation between generalized anxiety disorder and neuroticism. American Journal of Psychiatry. 2004;161:1581–1587. doi: 10.1176/appi.ajp.161.9.1581. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Chiu WTM, Demler O, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey. Archives of General Psychiatry. 2005;62:617–627. doi: 10.1001/archpsyc.62.6.617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kring AM, Bachorowski J. Emotions and psychopathology. Cognition and Emotion. 1999;13:575–599. [Google Scholar]
- Larson RJ, Deiner E. Affect intensity as an individual difference characteristic: A review. Journal of Research in Personality. 1987;21:1–39. [Google Scholar]
- Lynch TR, Robins CJ, Morse JQ, MorKrause ED. A mediational model relating affect intensity, emotion inhibition, and psychological distress. Behavior Therapy. 2001;32:519–536. [Google Scholar]
- McLaughlin KA, Mennin DS, Farach FJ. The contributory role of worry in emotion generation and dysregulation in generalized anxiety disorder. Behaviour Research and Therapy. 2007;45:1735–1752. doi: 10.1016/j.brat.2006.12.004. [DOI] [PubMed] [Google Scholar]
- Mennin DS, Turk CL, Heimberg RG. Clinical presentation and descriptive psychopathology of generalized anxiety disorder. In: Heimberg RG, Turk CL, Mennin DS, editors. Generalized Anxiety Disorder: Advances in Research and Practice. New York: Guilford Press; 2004. pp. 3–28. [Google Scholar]
- Mennin DS, Heimberg RG, Turk CL, Fresco DM. Preliminary evidence for an emotion regulation deficit model of generalized anxiety disorder. Behaviour Research and Therapy. 2005;43:1281–1310. doi: 10.1016/j.brat.2004.08.008. [DOI] [PubMed] [Google Scholar]
- Mennin DS, Holaway R, Fresco DM, Moore MT, Heimberg RG. Delineating components of emotion and its dysregulation in anxiety and mood psychopathology. Behavior Therapy. 2007;38:284–302. doi: 10.1016/j.beth.2006.09.001. [DOI] [PubMed] [Google Scholar]
- Salovey P, Stroud LR, Woolery A, Epel ES. Perceived emotional intelligence, stress reactivity, and symptom reports: Further explorations using the Trait Meta-Mood Scale. Psychology and Health. 2002;17:611–627. [Google Scholar]
- Salters-Pedneault K, Tull MT, Roemer L. The role of avoidance of emotional material in the anxiety disorders. Applied and Preventive Psychology. 2004;11:95–114. [Google Scholar]
- Salters-Pedneault K, Roemer L, Tull MT, Rucker L, Mennin DS. Evidence of broad deficits in emotion regulation associated with chronic worry and generalized anxiety disorder. Cognitive Therapy and Research. 2006;30:469–480. [Google Scholar]
- Turk CL, Heimberg RG, Luterek JA, Mennin DS, Fresco DM. Delineating emotion regulation deficits in generalized anxiety disorder: A comparison with social anxiety disorder. Cognitive Therapy and Research. 2005;29:89–106. [Google Scholar]
- Watson D. Rethinking the mood and anxiety disorders: A quantitative hierarchical model for DSM-V. Journal of Abnormal Psychology. 2005;114:522–536. doi: 10.1037/0021-843X.114.4.522. [DOI] [PubMed] [Google Scholar]