

Abstract
Background and Objectives
The prevalence of incomplete Kawasaki disease (iKD) is progressively increasing. We aimed to retrospectively investigate the predictors of intravenous immunoglobulin (IVIG) resistance in iKD patients and compare them with those of IVIG resistance in complete Kawasaki disease (cKD) patients. We also compared the prognosis of coronary artery lesions (CALs) between the IVIG non-responders and responders in both iKD and cKD groups.
Subjects and Methods
A total of 234 cKD and 77 iKD patients were treated with IVIG between February 2009 and April 2012. Among these 311 patients, we reviewed the data of 77 iKD patients and 75 age-matched cKD patients.
Results
Patients with iKD having an elevated neutrophil count {percentage of segmented neutrophils (SEG%) ≥79.0} were at risk of IVIG resistance, while patients with cKD having SEG% ≥79.25 and serum total bilirubin (TB) ≥0.56 mg/dL were at risk of IVIG resistance as shown by multivariable logistic regression analysis. Fractional changes of laboratory data before and after IVIG treatment showed that Creactive protein (CRP) and N-terminal B type natriuretic peptide (NT-proBNP) levels were significantly elevated in IVIG non-responders of the iKD group, whereas erythrocyte sedimentation rate was significantly elevated in IVIG non-responders of the cKD group. Among the patients who had CALs at 10 months after the start of illness, the z scores of coronary arteries were higher in IVIG non-responders of the iKD group, when compared with IVIG non-responders of the cKD group.
Conclusion
Elevated SEG%, changes in CRP and NT-proBNP levels may help in early detection of IVIG resistance in patients of the iKD group, which may aid in predicting the prognosis of CALs in these patients. Further studies with a larger number of patients are warranted.
Keywords: Kawasaki disease, Immunoglobulins, Coronary arteries
Introduction
Kawasaki disease (KD) is an acute systemic vasculitis that occurs in young children. According to the 2004 American Heart Association (AHA) guidelines for the diagnosis of KD, complete KD (cKD) is characterized by fever, changes in the extremities, polymorphous exanthem, bilateral bulbar conjunctival injection without exudate, changes in lips and oral cavity, and cervical lymphadenopathy (>1.5 cm in diameter).1) Patients with only two or three principal clinical features of KD in addition to fever are considered to have incomplete KD (iKD) when the other possible causes of fever have been excluded.1) The reported prevalence of iKD has increased from 15% to 47% since the publication of 2004 AHA guidelines.2),3),4),5),6)
A single dose (2 g/kg) of intravenous immunoglobulin (IVIG) infusion in combination with aspirin has been the standard treatment for KD.1) However, after initial treatment with IVIG, approximately 10-20% of KD patients have persistent or recrudescent fever, and they are said to show resistance to IVIG.1),7),8) Since prolonged fever can lead to increased prevalence of coronary artery lesions (CALs) in patients with KD,4),9) resistance to IVIG may be a risk factor for the development of CALs. Identification of patients who are at risk of IVIG resistance would ultimately aid in the prevention of CALs. Although several scoring systems have been developed for predicting IVIG resistance in patients with cKD,10),11),12) these scoring systems have limitations in predicting resistance to IVIG because of their low sensitivity. In addition, previous studies do not provide any information on the prevalence as well as on the prognosis of CALs in patients with iKD who show IVIG resistance.3),4),6) Therefore, the aim of this study was to determine the clinically useful predictors of IVIG resistance in patients with iKD as well as to compare and evaluate the prevalence and prognosis of CALs in patients with iKD and cKD.
Subjects and Methods
We retrospectively reviewed the medical records of patients diagnosed with KD at CHA Bundang Medical Center after receiving approval for the study from the Institutional Review Board of the same center. A total of 234 cKD and 77 iKD patients were treated with IVIG between February 2009 and April 2012. Among these 311 patients, we reviewed the laboratory measures and echocardiographic data of 77 iKD patients and 75 age-matched cKD patients.
Children with fever lasting 5 days or longer and at least 4 of the 5 principal clinical criteria of KD were defined as the cKD group, and children with 2 or 3 principal clinical criteria with fever lasting 5 or more days were defined as the iKD group with the exclusion of other alternative diagnosis.1) To exclude other febrile illnesses resembling KD, we performed serum titers for antistreptolysin-O, anti-Epstein-Barr virus antibodies, anti-Mumps virus antibodies, anti-mycoplasma antibodies, multiplex polymerase chain reaction for common respiratory viruses (respiratory syncytial virus, parainfluenza, influenza, metapneumovirus, rhinovirus) from nasopharyngeal aspirates, urinalysis, urine culture, and neck ultrasonogram results were reviewed to rule out suppurative lymphadenitis. All of the patients received 2 g/kg of IVIG in a single dose at the time of diagnosis, and were treated with high dose oral aspirin (80 mg/kg/day) until afebrile for 3-4 days and thereafter they were given low dose aspirin (5 mg/kg/day). Serial echocardiograms were done initially, after 3 months, and after 10 months to obtain the internal diameter of coronary arteries in both iKD and cKD groups. We measured the internal diameter of the proximal right coronary artery (RCA), proximal left anterior descending coronary artery (LAD), and left main coronary artery (LM). Patients were classified as having CALs when z scores of coronary arteries were found to be 2.5 or more in one or more of the RCA, LAD, and LM. The z scores of coronary arteries were obtained by using the measured dimensions of coronary arteries as well as the nonlinear regression equations based on the body surface area.13)
Patients were defined as IVIG non-responders when they had persistent or recrudescent fever ≥36 hours after completion of initial IVIG infusion.1) Patients in both the iKD and cKD groups were divided into IVIG non-responders and IVIG responders. Demographic variables studied were age, sex, duration of fever before and after initial treatment, and prevalence of IVIG resistance. Blood samples were obtained from patients before and at a median of 2 days after initial IVIG infusion. Laboratory variables studied were white blood cell count, percentage of segmented neutrophils (SEG%), hemoglobin, platelet count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), serum albumin, serum total bilirubin (TB), aspartate aminotransferase (AST), alanine aminotransferase (ALT), serum sodium, N-terminal B type natriuretic peptide (NT-proBNP), and gamma glutamyltransferase levels. In addition, to evaluate the treatment response after IVIG, we also compared the value of the fractional change (FC) of each variable as previously described by Mori et al.14) FC was defined as follows:
| FC=Y-X/X |
in which X represents laboratory data before IVIG and Y represents data at 2 to 3 days after IVIG treatment.14)
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) v. 20.0 for windows (SPSS, Chicago, IL, USA). Data are expressed as mean±standard deviation, percentage, or medians with the 25th and 75th percentiles in square brackets where appropriate. Comparison between variables was made with the Mann-Whitney U test for continuous variables and the chi-square test for categorical variables. To determine the predictive factors for IVIG resistance, we performed multivariable logistic regression analysis. To determine the cutoff value of each variable prior to multivariable logistic regression analysis, receiver operating characteristic curves (ROC) were used. Results were expressed as an odds ratio with a 95% confidence interval. A p of <0.05 was considered to be statistically significant.
Results
A total of 152 patients diagnosed with KD were enrolled in this study. Demographic variables are shown in Table 1. Of these, 77 patients (50.6%) were included in the iKD group, and 75 patients (49.3%) were included in the cKD group. Of these 152 KD patients, 84 patients were boys (55.3%) and 17 patients (11.2%) were IVIG non-responders. There was no significant difference in the prevalence of IVIG resistance between the iKD and cKD groups. Two patients had persistent fever after second infusion of IVIG and were treated with third IVIG infusion at ≥36 hours after completion of second IVIG treatment. Among the 5 principal symptoms of KD, conjunctival injection, changes in lips and oral cavity, and polymorphous exanthem were predominant in IVIG non-responders of the iKD group (Table 2). Comparison of laboratory data before initial IVIG treatment between the IVIG non-responders and the IVIG responders in the iKD and cKD groups is shown in Table 3. In the iKD group, the IVIG non-responders showed higher percentage of segmented neutrophils (SEG%) and TB before initial IVIG treatment compared to the IVIG responders; while in the cKD group, the IVIG non-responders showed higher AST and ALT levels and lower serum sodium levels in addition to higher SEG% and TB compared to the IVIG responders. Comparison of laboratory data after initial IVIG treatment showed no significant differences between IVIG non-responders and IVIG responders in both KD groups. To determine the cutoff value for predicting IVIG resistance, SEG% and TB before IVIG treatment in the iKD and cKD groups were assessed by ROC analysis. After multivariable logistic regression analysis, SEG% ≥79% was identified as a significant independent predictor of IVIG resistance in the iKD group with a sensitivity of 66.7% and specificity of 86.8%, SEG% ≥79.25% and TB ≥0.56 mg/dL were identified as significant predictors in the cKD group with a sensitivity of 75.0% and specificity of 95.5% (Table 4). FCs of laboratory data before and after IVIG treatment showed that CRP and NT-pro BNP levels were found to be significantly elevated after IVIG treatment in IVIG non-responders of the iKD group, whereas ESR was found to be significantly elevated in IVIG non-responders of the cKD group (Table 5).
Table 1.
Demographics of patients with incomplete KD and age-matched patients with complete KD
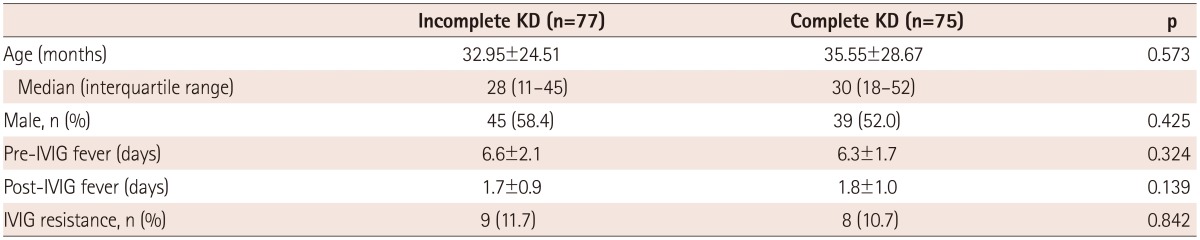
Data are expressed as mean±SD or median with the 25th and 75th percentiles in square brackets. *p<0.05. KD: Kawasaki disease, IVIG: intravenous immunoglobulin, Pre-IVIG fever: duration of fever until 1st IVIG, Post-IVIG fever: duration of fever until 2nd IVIG
Table 2.
Prevalence of 5 principal symptoms in patients with incomplete Kawasaki disease
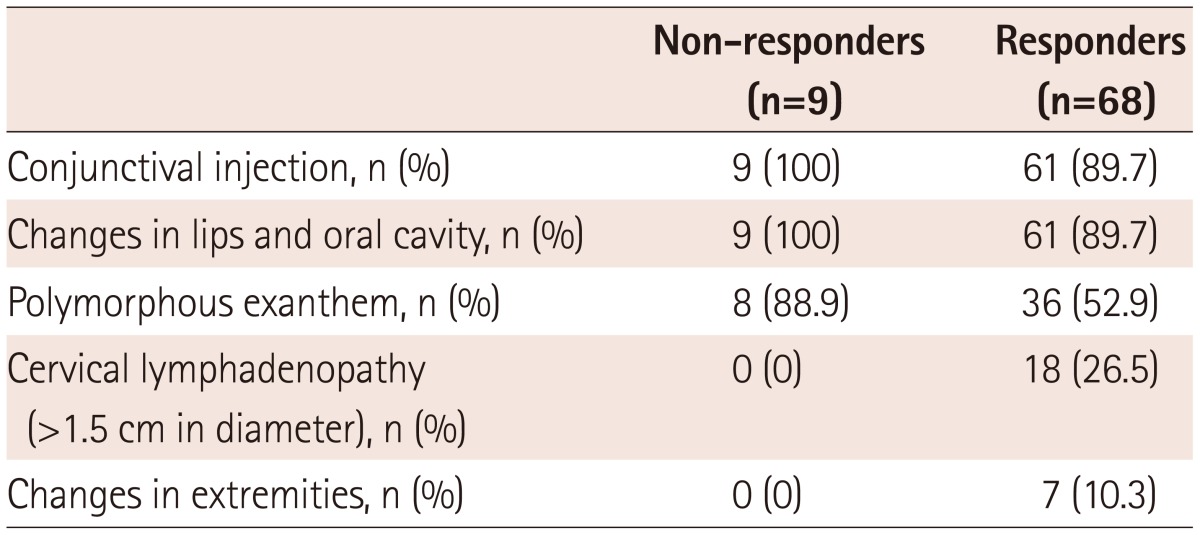
Non-responders: IVIG non-responders, Responders: IVIG responders. IVIG: intravenous immunoglobulin
Table 3.
Comparison of demographic, clinical, and laboratory features before initial treatment with IVIG in patients with incomplete and complete KD
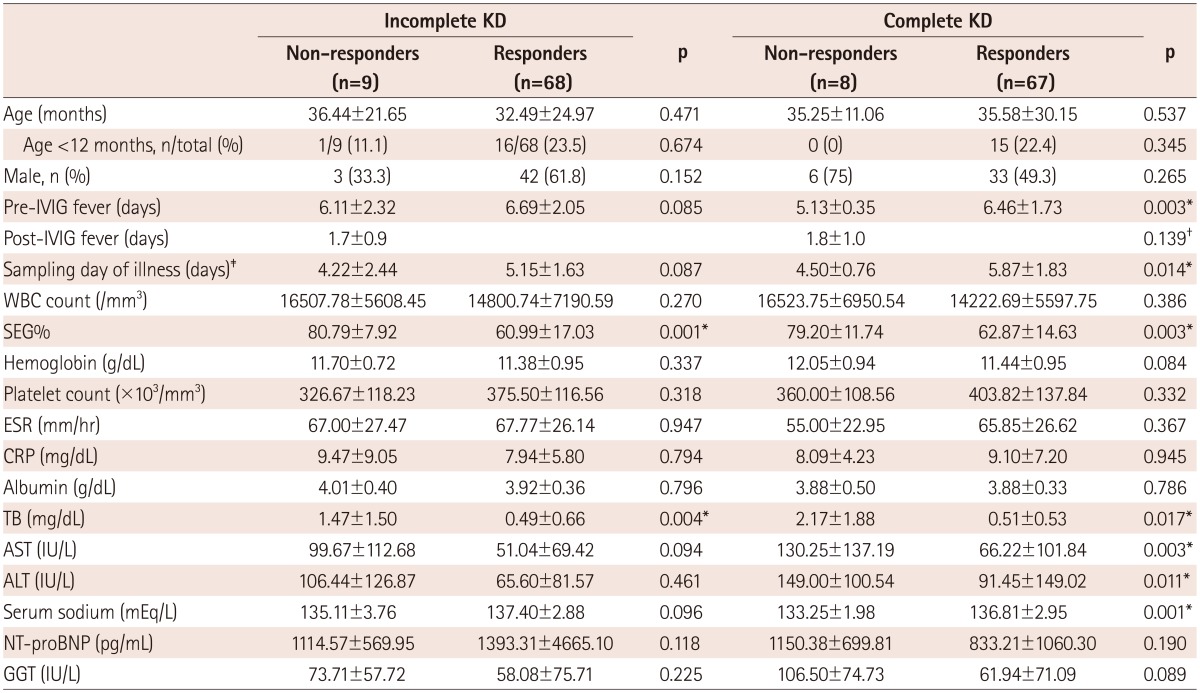
Data are expressed as mean±SD. *p<0.05, †p of comparison between IVIG non-responders in the incomplete and complete KD group, ‡Sampling day of illness: day of sampling calculated as days elapsed from the first day of illness. KD: Kawasaki disease, Non-responders: IVIG non-responders, Responders: IVIG responders, IVIG: intravenous immunoglobulin, WBC: white blood cell, SEG%: percentage of segmented neutrophils, ESR: erythrocyte sedimentation rate, CRP: C-reactive protein, TB: total bilirubin, AST: aspartate aminotransferase, ALT: alanine aminotransferase, NT-proBNP: N-terminal pro-B-type natriuretic peptide, GGT: gamma glutamyltransferase
Table 4.
Multivariable logistic regression analysis of predictors of IVIG resistance in patients with incomplete and complete KD

*p<0.05. KD: Kawasaki disease, SEG%: percentage of segmented neutrophils, TB: total bilirubin, OR: odds ratio, CI: confidence interval
Table 5.
Comparison of fractional changes of laboratory values before and after initial treatment with IVIG in patients with incomplete and complete KD
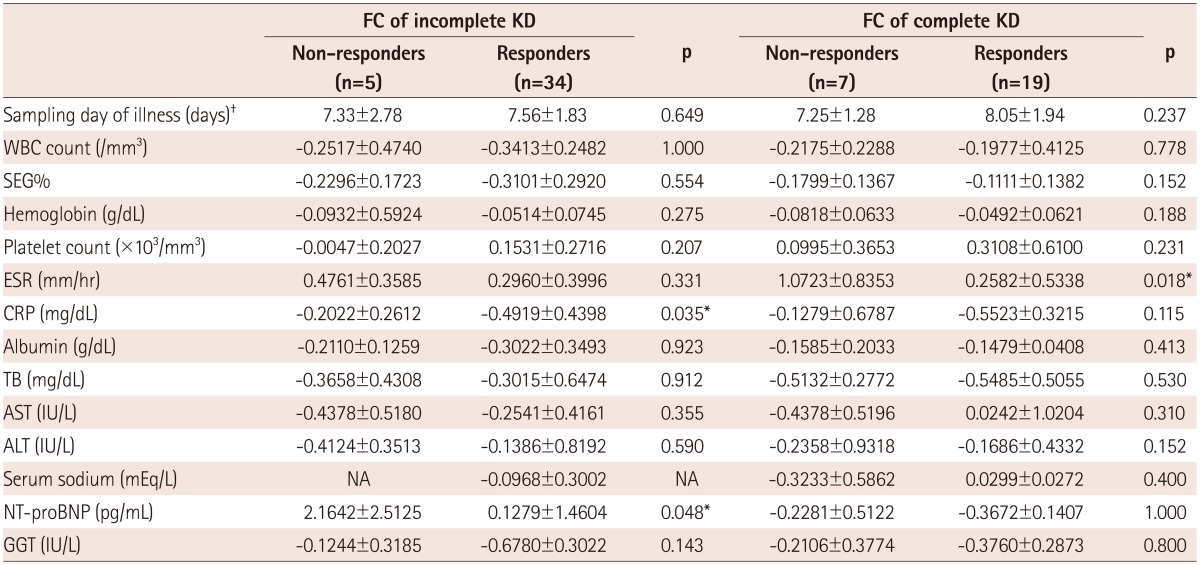
Data are expressed as mean±SD. FC=(Data at 2 to 3 days after IVIG)-(Data before IVIG)/Data before IVIG. *p<0.05, †SampliWBC: white blood cell, SEG%: percentage of segmented neutrophils, ESR: erythrocyte sedimentation rate,ng day of illness: day of sampling calculated as days elapsed from the first day of illness. IVIG: intravenous immunoglobulin, KD: Kawasaki disease, FC: fractional change, Non-responders IVIG non-responders, Responders: IVIG responders, CRP: C-reactive protein, TB: total bilirubin, AST: aspartate aminotransferase, ALT: alanine aminotransferase, NT-proBNP: N-terminal pro-B-type natriuretic peptide, GGT: gamma glutamyltransferase, NA: data not available
Follow-up echocardiogram was performed at 3 months (71-91 days) in 63 iKD and 56 cKD patients, and at 10 months (260-432 days) in 41 iKD and 25 cKD patients. The prevalence of CALs over time tended to be higher in the IVIG non-responders compared to the IVIG responders in the iKD group, when compared to those in the cKD group (Table 6). Individual z-scores of coronary arteries in patients with CALs in both the iKD and cKD groups after 10 months of follow-up showed that the RCA (n=7/10 vs. 5/5) was the most frequently involved coronary artery and the LM (n=1/10 vs. 0/5) was the least frequently involved coronary artery in both groups. Among the IVIG non-responders in both groups, z-scores of coronary arteries in patients of the iKD group were higher than those in patients of the cKD group. Among the IVIG responders, one patient in the iKD group showed a z score of the RCA >7 (Table 7).
Table 6.
Prevalence of coronary artery lesions (defined as z scores of coronary arteries ≥2.5) over time in patients with incomplete and complete KD
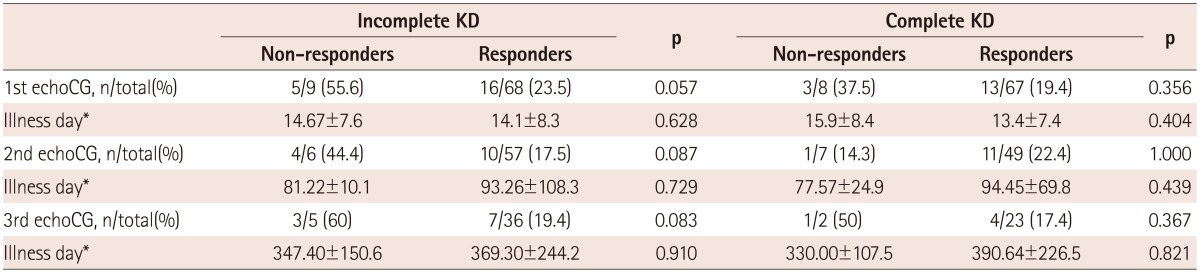
Data are expressed as mean±SD. *Illness day is defined as days elapsed from the 1st day of illness at the time of echocardiogram. KD: Kawasaki disease, Non-responders: IVIG non-responders, Responders: IVIG responders, EchoCG: echocardiogram
Table 7.
Z-scores of coronary arteries in patients with incomplete and complete KD having coronary artery lesions (defined as z scores of coronary arteries ≥2.5) at 10 months after onset of illness
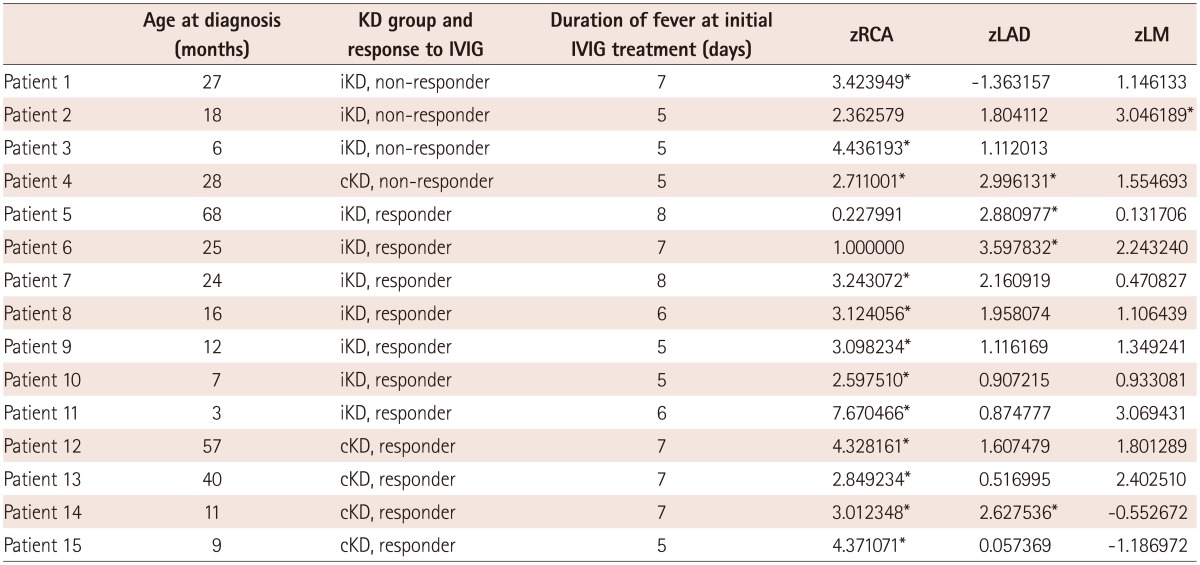
*Z score ≥2.5. KD: Kawasaki disease, iKD: incomplete Kawasaki disease, cKD: complete Kawasaki disease, non-responder: IVIG non-responder, responder: IVIG responder, RCA: right coronary artery, LAD: left anterior descending artery, LM: left main coronary artery, IVIG: intravenous immunoglobulin
Discussion
We found that elevated SEG% predicted IVIG resistance in the iKD group with higher sensitivity than the published scoring systems, while elevated SEG% and TB predicted IVIG resistance with higher sensitivity in the cKD group compared to the iKD group. FCs of laboratory data before and after IVIG treatment showed that CRP and NT-pro BNP levels were found to be significantly elevated after IVIG treatment in IVIG non-responders of the iKD group, whereas ESR was found to be significantly elevated in IVIG non-responders of the cKD group.
We found that in the iKD group, IVIG non-responders showed worse prognosis of CALs over time compared to IVIG responders, as indicated by the higher prevalence of CALs in IVIG non-responders over time and higher z scores of coronary arteries over time, while in the cKD group, no significant difference was found between IVIG non-responders and IVIG responders.
This is the first study to investigate and compare the predictors of IVIG resistance in both the iKD and cKD groups. Previously published studies on predictors of IVIG resistance have focused only on patients with cKD.7),10),11),12),15) Among the published studies, the value of elevated SEG% in predicting IVIG resistance in cKD patients has also been reported by Durongpisitkul et al.7) They reported an IVIG treatment failure rate of up to 11.6% in KD, and also that a high neutrophil count (>75%), low hemoglobin (<10 g/dL), and a low albumin level were associated with the requirement for retreatment with IVIG.7) However, they excluded the patients with iKD in their study. We found that elevated SEG% was also valuable for predicting IVIG resistance in the iKD group with a sensitivity of 66.7%. Our results also support the finding that leukocytosis is a characteristic finding during the acute phase in KD patients, especially the dominance of polymorphonuclear leukocytes.16) Predictors of IVIG resistance in patients with cKD who remained febrile on the 6th day of IVIG treatment have been studied by Fukunishi et al.15) with the exclusion of patients with iKD. They reported elevated CRP, lactate dehydrogenase, or low hemoglobin value as risk factors for IVIG resistance with 84.6% sensitivity and 87.0% specificity.15) Although in our study, CRP levels at 2 days after initial IVIG treatment in the IVIG non-responders appeared to remain higher compared to those in the IVIG responders of the iKD group, the difference failed to reach statistical significance. The difference in the value of CRP for predicting IVIG resistance between the study by Fukunishi et al.15) and our study can be explained by the difference in the IVIG infusion protocol (400 mg/kg/day for 5 days in the study by Fukunishi et al.15)), resulting in the shorter duration of fever before second IVIG treatment in our study group and possibly lower levels of CRP. In addition, CRP tends to rise later during the course of the disease;17) therefore, its use as a predictor of IVIG resistance may be limited during the early course of KD. However, the FC of CRP was significant in the iKD group in our study; hence, FC of CRP may be useful as a predictor of IVIG resistance as proposed by Kim et al.18) Kim et al. suggested that elevated SEG%, CRP, and NT-proBNP would be predictive values for necessitating IVIG retreatment in cKD patients. Our study group also included patients with iKD, and thus there are limitations in applying the results of the study by Fukunishi et al.15) to the patients with iKD. Of note, Ashouri et al.19) included patients with iKD in their study for assessing IVIG unresponsiveness, but their study does not provide information about the predictive factors of IVIG resistance in the iKD group.
The significance of other laboratory parameters such as serum NT-proBNP levels in predicting IVIG resistance was determined in patients with iKD as well as in patients with cKD in our study. After IVIG treatment, NT-proBNP levels remained higher in the IVIG non-responders (3038.20±4360.80 pg/mL) compared to IVIG responders (683.53±671.93 pg/mL; p=0.053) in the iKD group of our study, but the results narrowly failed to reach statistical significance. However, the FC of NT-proBNP was significant in IVIG non-responders in the iKD group. As previously suggested by Kim et al.18) FC of NT-proBNP might be useful in predicting IVIG resistance in iKD patients, but, the small number of patients in our study limits the generalizability and utility of our findings. However, the FC of NT-proBNP was not significant in predicting IVIG resistance in cKD in our study, which may be explained by the late sampling date from the start of illness. The degree of inflammation may have decreased over time. The clinical usefulness of NT-proBNP levels in diagnosing KD has been demonstrated by McNeal-Davidson et al.20); however, in their report, the difference in NT-proBNP levels between IVIG non-responders and IVIG responders did not reach statistical significance. In addition, the relative lack of value of TB in predicting IVIG resistance in iKD patients compared with cKD patients in our study may be correlated with more systemic inflammation in cKD patients compared with iKD patients since elevated TB levels probably reflect inflammation of the bile duct.21)
Our results suggest that IVIG resistance can lead to worse outcomes of coronary artery lesions in patients with iKD compared to patients with cKD. In our present study, IVIG non-responders in the iKD group showed consistently higher prevalence of coronary artery lesions over time compared to those in the cKD group. We found that in the cKD group, the relationship between IVIG resistance and CALs seemed to be nonlinear, as reported by Kobayashi et al.12) Conflicting reports on the outcomes of CALs in patients with iKD have been published previously.3),4),5),17),22) A possible cause of increased prevalence of CALs in patients with iKD has previously been reported to be delayed diagnosis of KD and resulting treatment delay.3) Sonobe et al.3) reported that fewer patients with iKD received IVIG treatment compared to patients with cKD, and the prevalence of CALs in KD tended to increase as the number of symptoms decre-ased. The duration of fever has been known to be associated with the prognosis of coronary artery lesions.17) Yeo et al.16) reported that prolonged inflammatory challenge of coronary arteries due to prolonged fever increases their vulnerability to dilatation. Since all of the patients in our study, in both the iKD and cKD groups, received IVIG treatment, and since the duration of fever before initial IVIG treatment was not significantly different, higher z scores of coronary arteries in IVIG non-responders in the iKD group might not be due to missed treatment or longer duration of fever but due to elevated SEG%. Manlhiot et al.5) reported that despite delayed diagnosis of iKD, a similar response to IVIG treatment and similar outcomes of coronary artery lesions are observed in patients with iKD, and they emphasized that iKD and cKD are two sides of the same coin. Interestingly, in our present study, although the duration of fever before treatment was shorter in the iKD group compared with that in the study by Manlhiot et al.,5) we observed worse outcomes of coronary artery lesions in IVIG non-responders in the iKD group only. Therefore, we speculate that worse outcomes of coronary artery lesions in IVIG non-responders in the iKD group only might be due to an intrinsic difference that led to incomplete presentation of KD.
In our study, 2 patients who failed to respond to second IVIG treatment received third IVIG treatment. One patient was lost to follow-up, and the other showed CAL in the RCA after 10 months. Although the evaluation of efficacy of steroid treatment in preventing CALs is beyond the scope of the present study, conflicting results of steroid treatment in IVIG non-responders still exist, thereby influencing the clinical judgement for treating IVIG non-responders with steroids. Kobayashi et al.12) suggested early administration of prednisolone in addition to IVIG in IVIG non-responders. On the other hand, Millar et al.23) reported that pulsed doses of methylprednisolone as a rescue therapy for IVIG non-responders might impair regression of the coronary artery wall.
There are several limitations to our study. First, our study is a retrospective study, so we did not have a separate validation dataset for validating the predictive value of elevated SEG% in predicting IVIG resistance in a separate iKD group. Second, this is a single-center study with a small number of patients. Furthermore, in our study, many patients with KD were lost to follow-up; therefore, unfortunately, echocardiography data at the 3-month and 10-month follow-up are limited to a few patients. Third, since we tried to select age-matched patients, we did not enroll all of the cKD patients at our institution; therefore, there may be an unknown selection bias. Lastly, we cannot rule out the possibility that at least some patients with iKD in our study might not have had KD but another illness closely resembling KD. We hopefully minimized this possibility by carefully trying to exclude patients with a more plausible cause of other febrile illnesses.
In conclusion, we demonstrated that elevated SEG%, changes in CRP and NT-proBNP may help in early detection of IVIG resistance in patients of the iKD group, which may aid in predicting the prognosis of CALs in these patients. Elevated SEG% may be a useful predictor of IVIG resistance in patients with iKD. Patients with iKD who are show IVIG non-responders may present with worse prognosis of CALs at follow-up compared to patients with cKD. A better understanding of the pathogenesis of KD will help to elucidate the mechanism underlying IVIG resistance in patients with iKD, and to identify other important factors that will help in selecting the patients at risk in this group. Further study in a larger group of patients is warranted to determine the plausibility of our findings. Furthermore, our results may be beneficial for selecting patients with iKD who are at risk of IVIG resistance during the early stage of the disease to allow for considering a more advanced therapy.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110:2747–2771. doi: 10.1161/01.CIR.0000145143.19711.78. [DOI] [PubMed] [Google Scholar]
- 2.Ghelani SJ, Sable C, Wiedermann BL, Spurney CF. Increased incidence of incomplete Kawasaki disease at a pediatric hospital after publication of the 2004 American Heart Association guidelines. Pediatr Cardiol. 2012;33:1097–1103. doi: 10.1007/s00246-012-0232-9. [DOI] [PubMed] [Google Scholar]
- 3.Sonobe T, Kiyosawa N, Tsuchiya K, et al. Prevalence of coronary artery abnormality in incomplete Kawasaki disease. Pediatr Int. 2007;49:421–426. doi: 10.1111/j.1442-200X.2007.02396.x. [DOI] [PubMed] [Google Scholar]
- 4.Witt MT, Minich LL, Bohnsack JF, Young PC. Kawasaki disease: more patients are being diagnosed who do not meet American Heart Association criteria. Pediatrics. 1999;104:e10. doi: 10.1542/peds.104.1.e10. [DOI] [PubMed] [Google Scholar]
- 5.Manlhiot C, Christie E, McCrindle BW, Rosenberg H, Chahal N, Yeung RS. Complete and incomplete Kawasaki disease: two sides of the same coin. Eur J Pediatr. 2012;171:657–662. doi: 10.1007/s00431-011-1631-2. [DOI] [PubMed] [Google Scholar]
- 6.Sudo D, Monobe Y, Yashiro M, et al. Coronary artery lesions of incomplete Kawasaki disease: a nationwide survey in Japan. Eur J Pediatr. 2012;171:651–656. doi: 10.1007/s00431-011-1630-3. [DOI] [PubMed] [Google Scholar]
- 7.Durongpisitkul K, Soongswang J, Laohaprasitiporn D, Nana A, Prachuabmoh C, Kangkagate C. Immunoglobulin failure and retreatment in Kawasaki disease. Pediatr Cardiol. 2003;24:145–148. doi: 10.1007/s00246-002-0216-2. [DOI] [PubMed] [Google Scholar]
- 8.Tremoulet AH, Best BM, Song S, et al. Resistance to intravenous immunoglobulin in children with Kawasaki disease. J Pediatr. 2008;153:117–121. doi: 10.1016/j.jpeds.2007.12.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Honkanen VE, McCrindle BW, Laxer RM, Feldman BM, Schneider R, Silverman ED. Clinical relevance of the risk factors for coronary artery inflammation in Kawasaki disease. Pediatr Cardiol. 2003;24:122–126. doi: 10.1007/s00246-002-0063-1. [DOI] [PubMed] [Google Scholar]
- 10.Egami K, Muta H, Ishii M, et al. Prediction of resistance to intravenous immunoglobulin treatment in patients with Kawasaki disease. J Pediatr. 2006;149:237–240. doi: 10.1016/j.jpeds.2006.03.050. [DOI] [PubMed] [Google Scholar]
- 11.Sano T, Kurotobi S, Matsuzaki K, et al. Prediction of non-responsiveness to standard high-dose gamma-globulin therapy in patients with acute Kawasaki disease before starting initial treatment. Eur J Pediatr. 2007;166:131–137. doi: 10.1007/s00431-006-0223-z. [DOI] [PubMed] [Google Scholar]
- 12.Kobayashi T, Inoue Y, Takeuchi K, et al. Prediction of intravenous immunoglobulin unresponsiveness in patients with Kawasaki disease. Circulation. 2006;113:2606–2612. doi: 10.1161/CIRCULATIONAHA.105.592865. [DOI] [PubMed] [Google Scholar]
- 13.McCrindle BW, Li JS, Minich LL, et al. Coronary artery involvement in children with Kawasaki disease: risk factors from analysis of serial normalized measurements. Circulation. 2007;116:174–179. doi: 10.1161/CIRCULATIONAHA.107.690875. [DOI] [PubMed] [Google Scholar]
- 14.Mori M, Imagawa T, Yasui K, Kanaya A, Yokota S. Predictors of coronary artery lesions after intravenous gamma-globulin treatment in Kawasaki disease. J Pediatr. 2000;137:177–180. doi: 10.1067/mpd.2000.107890. [DOI] [PubMed] [Google Scholar]
- 15.Fukunishi M, Kikkawa M, Hamana K, et al. Prediction of non-responsiveness to intravenous high-dose gamma-globulin therapy in patients with Kawasaki disease at onset. J Pediatr. 2000;137:172–176. doi: 10.1067/mpd.2000.104815. [DOI] [PubMed] [Google Scholar]
- 16.Yeo Y, Kim T, Ha K, et al. Incomplete Kawasaki disease in patients younger than 1 year of age: a possible inherent risk factor. Eur J Pediatr. 2009;168:157–162. doi: 10.1007/s00431-008-0722-1. [DOI] [PubMed] [Google Scholar]
- 17.Giannouli G, Tzoumaka-Bakoula C, Kopsidas I, Papadogeorgou P, Chrousos GP, Michos A. Epidemiology and risk factors for coronary artery abnormalities in children with complete and incomplete Kawasaki disease during a 10-year period. Pediatr Cardiol. 2013;34:1476–1481. doi: 10.1007/s00246-013-0673-9. [DOI] [PubMed] [Google Scholar]
- 18.Kim HK, Oh J, Hong YM, Sohn S. Parameters to guide retreatment after initial intravenous immunoglobulin therapy in kawasaki disease. Korean Circ J. 2011;41:379–384. doi: 10.4070/kcj.2011.41.7.379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ashouri N, Takahashi M, Dorey F, Mason W. Risk factors for nonresponse to therapy in Kawasaki disease. J Pediatr. 2008;153:365–368. doi: 10.1016/j.jpeds.2008.03.014. [DOI] [PubMed] [Google Scholar]
- 20.McNeal-Davidson A, Fournier A, Spigelblatt L, et al. Value of aminoterminal pro B-natriuretic peptide in diagnosing Kawasaki disease. Pediatr Int. 2012;54:627–633. doi: 10.1111/j.1442-200X.2012.03609.x. [DOI] [PubMed] [Google Scholar]
- 21.Seki S, Habu Y, Kawamura T, et al. The liver as a crucial organ in the first line of host defense: the roles of Kupffer cells, natural killer (NK)cells and NK1.1 Ag+ T cells in T helper 1 immune responses. Immunol Rev. 2000;174:35–46. doi: 10.1034/j.1600-0528.2002.017404.x. [DOI] [PubMed] [Google Scholar]
- 22.Ha KS, Jang G, Lee J, et al. Incomplete clinical manifestation as a risk factor for coronary artery abnormalities in Kawasaki disease: a metaanalysis. Eur J Pediatr. 2013;172:343–349. doi: 10.1007/s00431-012-1891-5. [DOI] [PubMed] [Google Scholar]
- 23.Millar K, Manlhiot C, Yeung RS, Somji Z, McCrindle BW. Corticosteroid administration for patients with coronary artery aneurysms after Kawasaki disease may be associated with impaired regression. Int J Cardiol. 2012;154:9–13. doi: 10.1016/j.ijcard.2010.08.070. [DOI] [PubMed] [Google Scholar]