

Sir,
Chikungunya fever, an arboviral disease caused by chikungunya virus (CHIKV), manifests as an acute illness with fever, skin rash and severe and incapacitating arthralgia1 that may persist for several months or even years2. Cytokines and chemokines such as interleukin (IL)-6, IL- 8, monocyte chemoattractant protein (MCP)-1 and macrophage inflammatory protein (MIP)-1 appear to play important roles in the pathogenesis of chronic arthritis in CHIKV infection3. The persistence of the specific IgM antibodies for months after the initial infection has been observed in several alpha viral infections, probably due to viral persistence but the underlying mechanism is poorly understood4. The present report is an update of our earlier study5 on evolution of joint lesions and arthritic symptoms in patients who had developed chronic arthritis following CHIKV infection and on the immunological response in these patients.
The original study group cohort consisted of 203 patients with chikungunya fever identified during an outbreak in Dakshina Kannada district of Karnataka State, India, in 2008. The presence of CHIKV infection in these patients was confirmed by the presence of anti-CHIKV IgM antibodies. These patients were followed up for a period of 10 months. Ninety four of these 203 patients continued to have arthritic symptoms at the end of 10 months. A subsample of 20 such patients with unresolved arthritic symptoms was subjected to magnetic resonance imaging (MRI) studies, the results of which were reported earlier5.
The present study was conducted in April 2011, three years after the onset of chikungunya disease in these patients. MRI was repeated in 14 of the 20 patients who had been subjected to MRI at the end of 10 months. These 14 patients were interviewed for the changes in their arthritic symptoms. Blood samples were collected and tested for anti-CHIKV IgM and IgG antibodies by IgM capture ELISA6 and NovaLisa™ Chikungunya virus IgG capture ELISA (Nova Tec Immundiagnostica GmbH, Germany) respectively. Detailed history of treatment for their arthritic symptoms could not be obtained for these patients because of non-availability of any medical records. The study was approved by the institutional ethics committee of the Regional Medical Research Centre, Port Blair, Andaman and Nicobar Islands, India, and written informed consent was obtained from patients.
Thirteen of these 14 patients had mono-arthritis and one had oligoarthritis. Arthritic symptoms and signs in one of the 14 patients had completely resolved and in two others, the joint pain had substantially reduced. Four patients reported slight improvement and in the remaining seven, the symptoms persisted without change. None of the patients experienced worsening of symptoms. The mean age of the patients who reported that their symptoms persisted was 58.4 yr whereas that of the patients who showed improvement in symptoms was 49.4 yr. Among the five male patients in the study group, two showed persistence of symptoms while among the nine female patients, five showed persistence of symptoms.
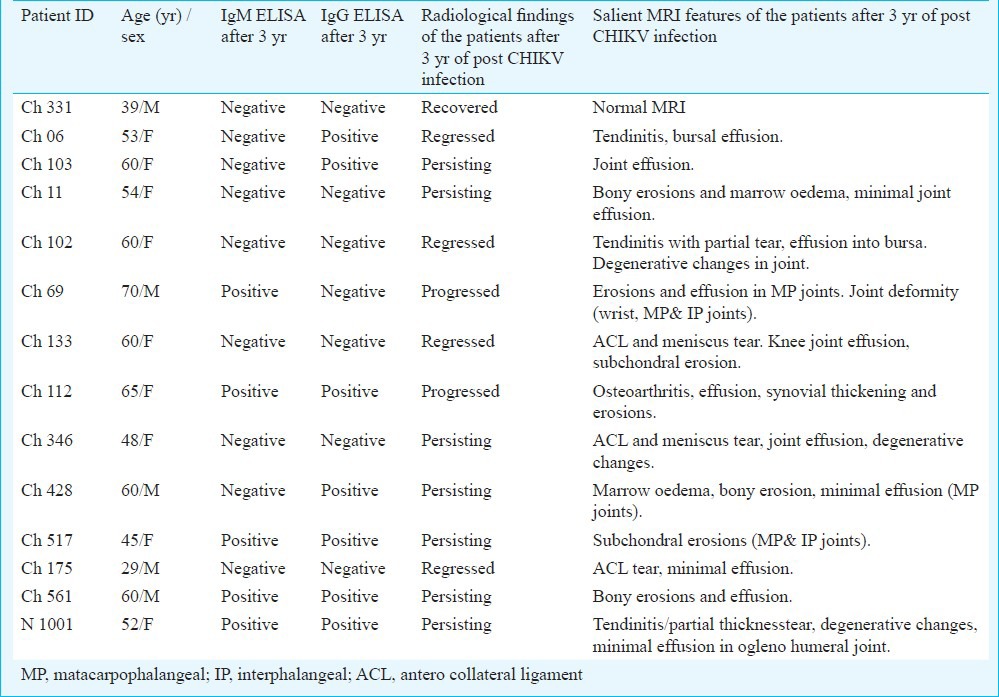
The MRI showed that in one patient, there was complete resolution of the lesions and in four others the lesions were regressing. In two patients the lesions appeared to be progressing with involvement of new joints (Carpal and inter-carpal joints, lower ends of radius and ulna). In the remaining seven patients, the radiological abnormalities remained unaltered. Thus in five of the fourteen patients, the radiological abnormalities regressed and in the remaining nine either persisted or progressed (Table). The mean age of the former group of patients was 48.2 yr and that of the latter was 57.1 yr. Among the five male patients in the study group, three showed persistence or progression of radiological abnormalities while among the nine female patients, six showed persistence of progression of lesions.
Table.
ELISA results and symptoms of the patients after three years post chikungunya virus infection
The patient who showed complete resolution of lesions had focal bony erosions and bursitis in the MRI earlier5. Although these lesions have disappeared completely, mild joint pain still persisted. Three of the four patients who showed signs of radiological resolution of lesions had tendinitis, calcification and effusion into joints and bursae earlier. The seven patients with persistent lesions had sub-chondral bony erosions, joint effusion and synovial thickening (Fig. A) earlier. While two of these seven patients reported reduction in the intensity of pain since the last follow up, the remaining five patients reported that their joint pain was persisting without any change. The two patients whose lesions were progressing had bony erosions in metacarpals and effusion in metacarpo-phalangeal joints in earlier MRIs. These lesions progressed and the new lesions including erosions and joint effusion appeared in carpal bones, inter-carpal joints and lower ends of radius and ulna (Fig. B).
Fig.
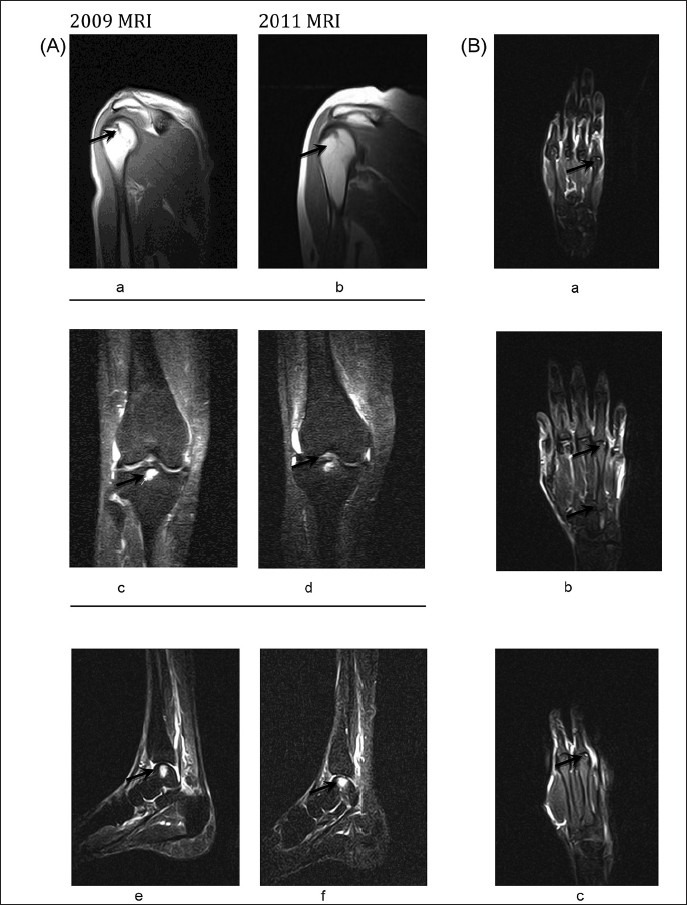
(A). Persisting Focal Altered signal intensity lesions; (a, b) hypointense on T1 weighed sequence in posterior aspect of head of humerus; (c, d) lesion in intercondylar region of tibia; (e, f) Right Ankle. Fig. (B). (a) Lesion in 5th metacarpal with minimal effusion in MP joints of 2nd and 5th fingers at the end of 10th month of post CHIKV infection (2009). Lesions in sub-articular region of head of 3rd, 4th and 5th metacarpal with minimum effusion observed in 3rd to 5th MP joints, new erosion in 3rd and 4th metacarpals. (b, c) at the end of 3 years of post CHIKV infection (2011).
Among the nine patients with either persistent or progressing lesions, five were positive of IgM anti-CHIKV antibodies, while none of the five patients whose lesions had regressed completely or partially was positive for IgM antibodies. Seven patients were positive for IgG antibodies.
In seven of these patients with post-CHIKV arthritis who could be followed up at the end of three years,the arthritic symptoms remained unabated. In two of the patients the lesions appeared to have progressed and affected new joints.
This group of patients was tested for rheumatoid factor (RF) and anti- cyclic citrullinated protein (CCP) antibody during the follow up at 10 months and all except one patients were found negative for these5. These tests were not repeated during the present follow up.
Persistent polyarthralgia and arthritis have been reported in 10 to 20 per cent of patients who suffer CHIKV infection, 20 to 36 months of post infection2, which mimicked rheumatoid arthritic syndrome. Studies have shown nerosive arthritis and tenosynovitis in patients during the convalescent stage of CHIKV infection7. A study on patients with chronic arthritic disability (CAD) after CHIKV infection in Sri Lanka showed that in 6.1 per cent of the patients the debilities persisted at the end of three years of follow up8.
The present study showed the persistence of detectable gM against CHIKV after three years post-infection in five of 14 patients with arthritis and in all these patients the joint lesions either persisted or had worsened.
Studies have shown high levels of CHIKV IgM antibodies in Indian patients with post-CHIKV rheumatoid arthritis (RA)-like illnesses9. Chronic rheumatism, IgM-anti CHIKV antibodies and elevated IL-6 levels have been shown to persist for a long duration after CHIKV infection9,10. Long-term existence of CHIKV in joints, muscles, lymphoid organs, liver and, macrophages in non-human primates has also been documented11. Persistence of other alphaviruses such as Ross River virus (RRV) in synovial macrophages has been reported12 and suggested to be responsible for log-term persistence of IgM antibodies. The present study, although confined to a small number of patients, suggests a possible association of persistent anti-CHIKV IgM antibodies with persistence of arthritic lesions and symptoms.
Acknowledgment
Authors acknowledge the District Health and Family Welfare Officer, Mangalore, Dr Jagannath, for his support, and other staff of Adyanadka Primary Health Centre, and thank Shri Bhaskar, Health Inspector from PCH Adyanadka for his extensive support during the working period in the remote villages. The study was financially supported by the Department of Biotechnology, Government of India, Ministry of Science and Technology, New Delhi, India (Grant No. BT/PR9372/Med/29/24/2007 dated 17-02-2009).
References
- 1.Robinson MC. An epidemic of virus disease in Southern Province, Tanganyika Territory, in 1952-1953.I. Clinical features. Trans R Soc Trop Med Hyg. 1955;49:28–32. doi: 10.1016/0035-9203(55)90080-8. [DOI] [PubMed] [Google Scholar]
- 2.Brighton SW, Prozesky OW, de la Harpe AL. Chikungunya virus infection. A retrospective study of 107 cases. S Afr Med J. 1983;63:313–5. [PubMed] [Google Scholar]
- 3.Chaaitanya IK, Muruganandam N, Sundaram SG, Kawalekar O, Sugunan AP, Manimunda SP, et al. Role of pro-inflammatory cytokines and chemokines in chronic arthropathy in CHIKV infection. Viral Immunol. 2011;24:265–71. doi: 10.1089/vim.2010.0123. [DOI] [PubMed] [Google Scholar]
- 4.Kuno G. Persistence of arboviruses and antiviral antibodies in vertebrate hosts: its occurrence and impacts. Rev Med Virol. 2001;11:165–90. doi: 10.1002/rmv.314. [DOI] [PubMed] [Google Scholar]
- 5.Manimunda SP, Vijayachari P, Uppoor R, Sugunan AP, Singh SS, Rai SK, et al. Clinical progression of chikungunya fever during acute and chronic arthritic stages and the changes in joint morphology as revealed by imaging. Trans R Soc Trop Med Hyg. 2010;104:392–99. doi: 10.1016/j.trstmh.2010.01.011. [DOI] [PubMed] [Google Scholar]
- 6.Gadkari DA, Shaikh BH. IgM antibody capture ELISA in the diagnosis of Japanese encephalitis, West Nile & dengue virus infections. Indian J Med Res. 1984;80:613–9. [PubMed] [Google Scholar]
- 7.Mizuno Y, Kato Y, Takeshita N, Ujiie M, Kobayashi T, Kanagawa S, et al. Clinical and radiological feature of imported chikungunya fever in Japan: a study of six cases at the National Centre for Global Health and Medicine. J Infect Chemother. 2011;17:419–23. doi: 10.1007/s10156-010-0124-y. [DOI] [PubMed] [Google Scholar]
- 8.Kularatne SA, Weerasinghe SC, Gihan C, Wickramasinghe S, Dharmarathne S, Abeyrathna A, et al. Epidemiology, clinical manifestations, and long-term outcomes of a major outbreak of chikungunya in a hamlet in Srilanka, in 2007: a longitudinal cohort study. J Trop Med 2012. 2012:1–60. doi: 10.1155/2012/639178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chopra A, Anuradha V, Ghorpade R, Saluja M. Acute Chikungunya and persistent musculoskeletal pain following the 2006 Indian epidemic: a 2 year prospective rural community study. Epidemiol Infect. 2012;140:842–50. doi: 10.1017/S0950268811001300. [DOI] [PubMed] [Google Scholar]
- 10.Chopra A, Anuradha V, Lagoo-Joshi V, Kunjir V, Salvi S, Saluja M. Chikungunya virus aches and pains: an emerging challenge. Arthritis Rheum. 2008;58:2921–2. doi: 10.1002/art.23753. [DOI] [PubMed] [Google Scholar]
- 11.Labadie K, Larcher T, Joubert C, Mannioui A, Delache B, Brochard P, et al. Chikungunya disease in nonhuman primates involves long-term viral persistence in macrophages. J Clin Invest. 2010;120:894–906. doi: 10.1172/JCI40104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lee CY, Kam YW, Fric J, Malleret B, Koh EG, Prakash C, et al. Chikungunya virus neutralization antigens and direct cell-to-cell transmission are revealed by human antibody-escape mutants. PLoS Pathog. 2011;7:e1002390. doi: 10.1371/journal.ppat.1002390. [DOI] [PMC free article] [PubMed] [Google Scholar]