

Advances in Hodgkin lymphoma (HL) treatment have dramatically improved prognosis, with 5-year relative survival now over 80% in the United States (US) and Europe. However, subsequent malignancies, often occurring as late adverse effects of treatment, are a leading cause of morbidity and mortality among HL survivors.
Radiotherapy has been an important component of HL treatment for decades. Despite substantial evolution in radiotherapy fields and techniques to reduce normal tissue exposure,1 the esophagus is commonly exposed to ionizing radiation even with current HL treatment approaches (e.g. involved-field radiotherapy, intensity-modulated radiotherapy) because more than 90% of HL patients present with involvement of the lymph nodes in the mediastinum and/or neck.2 Elevated esophageal cancer risk after HL has been reported in registry-based studies and clinical series,3–7 with higher risks among patients treated with radiotherapy.5,7 However, no previous study has investigated esophageal cancer risk among HL survivors with detailed treatment data and long-term follow up.
We conducted an international nested case-control study to quantify risk of esophageal cancer in relation to specific HL treatments among 19,882 patients who survived five years or more following diagnosis with first primary, histologically-confirmed HL. HL patients, diagnosed during 1943–1992 and followed through 2005, were identified through 6 population-based cancer registries in Europe and North America (n=17,447) and a Dutch hospital-based cohort (n=2435; additional detail provided in Online Supplementary Appendix). The 37 HL patients with a registry report of second primary esophageal cancer were eligible for inclusion (regardless of their treatment history). Two controls per case were individually matched by registry, race, birth date (±5 years), HL diagnosis date (±5 years), hospital of diagnosis (in Norway only; Radium Hospital vs. others), and survival without subsequent cancer at least as long as the matched case’s interval from HL to esophageal cancer. The final study population with available records included 36 cases and 71 controls. The study was approved by authorities in each study center and exempted from IRB review by the National Cancer Institute.
Detailed data on patient demographics, HL diagnosis, HL treatments (for both initial and relapsed disease), and potential esophageal cancer risk factors (cigarette smoking, alcohol consumption, height, weight, and family history of cancer in a first-degree relative) were abstracted from all available medical records. For cases, esophageal cancer diagnosis was also confirmed and information on tumor location was abstracted. Patients who received radiotherapy generally were treated with cumulative target doses of 25–40 Gy using conventional fractionation. Radiation doses were reconstructed for each patient at 24 points located centrally in the esophagus plus the gastroesophageal junction, summing doses received from all treatments. Chemotherapy analyses evaluated cumulative number of alkylating agent (AA)-containing cycles, receipt of specific regimens, and cumulative dose (mg/m2) for specific AAs. Abstracted data on cigarette smoking and alcohol consumption included amount and current use at the time of medical record report or year of quitting. To minimize potential bias arising from more complete information on smoking, alcohol, and family history of cancer for cases than controls, only data recorded at least one year preceding esophageal cancer diagnosis (comparable date for controls) were used. Former smokers were identified by medical record reports indicating that the patient quit five years or more preceding esophageal cancer diagnosis (comparable date for controls). Among patients with available data on cigarette smoking (24 of 36, 67% cases; 44 of 71, 62% controls), information was typically collected at the time of HL diagnosis (24 cases, 42 controls) or within two years of HL diagnosis (2 controls). Body mass index (BMI, kg/m2) was computed at HL diagnosis.
Conditional logistic regression models estimated the relative risk of esophageal cancer in relation to HL treatments with odds ratios (ORs) and corresponding 95% confidence intervals (CIs). Analyses of radiotherapy risks used dose to the esophageal tumor midpoint (comparable location for controls) considering both categorical and continuous radiation dose. For the continuous analysis, the excess odds ratio per Gy (EOR/Gy) was estimated by the model OR=exp(∑jαjxj)[1+βz], where z=radiation dose, β=EOR/Gy, and xj=covariates (e.g. chemotherapy). Heterogeneity in the radiation-related esophageal cancer risks in patient subgroups was evaluated under the multiplicative model with a likelihood ratio test. Cumulative incidence of second primary esophageal cancer was estimated with death and other second cancers as competing risks.8
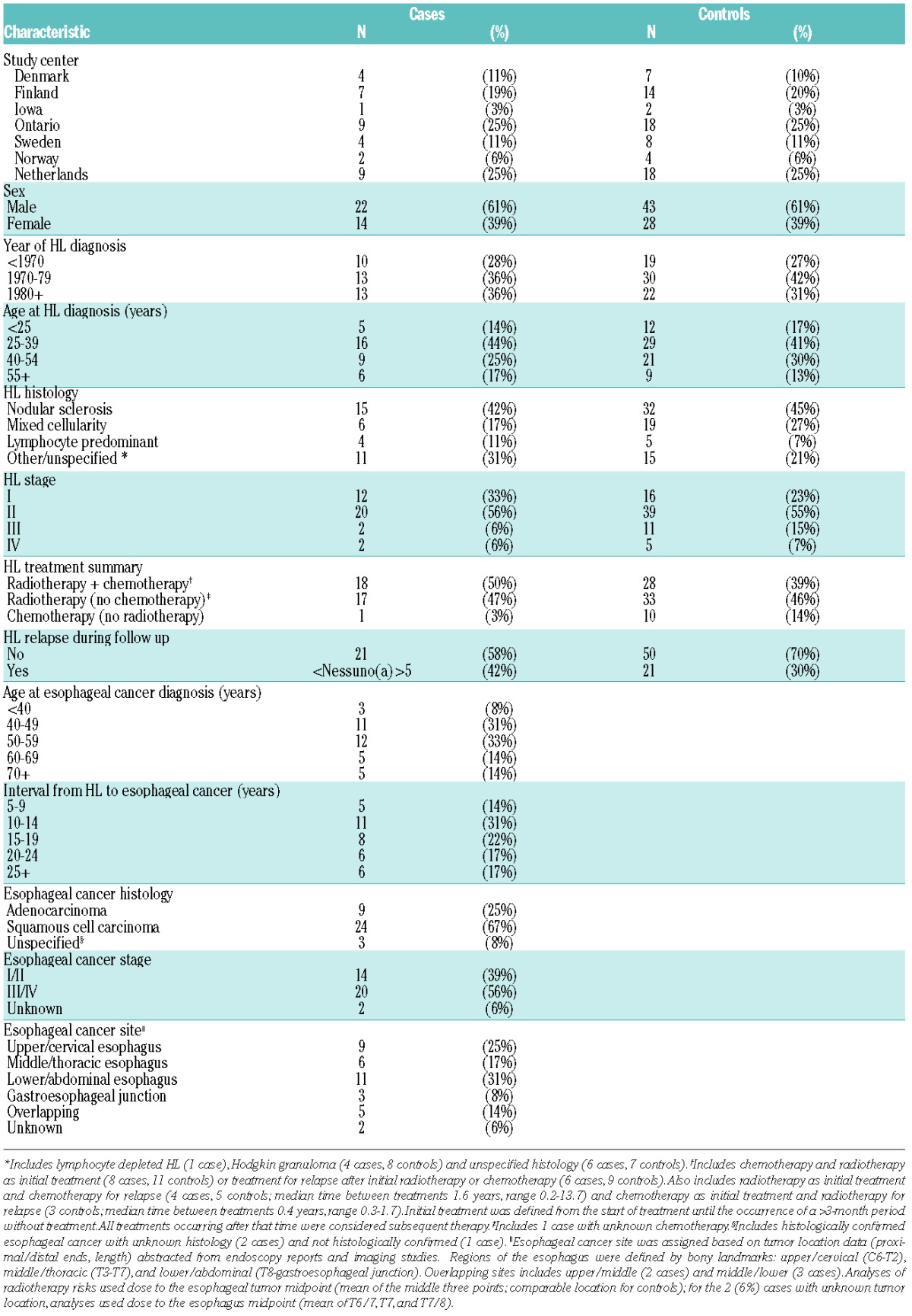
Median age at HL diagnosis in our study population was 34 years and half the cases were diagnosed in 1975 or later (Table 1). Most patients received radiotherapy, either with chemotherapy (50% cases, 39% controls) or without chemotherapy (47% cases, 46% controls). Occurrence of second primary esophageal cancer was rare, with an estimated cumulative incidence in the population-based cohort of 0.38% (95%CI: 0.23–0.53%) at 30 years. Median age at esophageal cancer was 54 years, with 75% of esophageal cancers arising 12 years or more after HL (median time from HL to esophageal cancer=16 years). Thirty-two (89%) cases were known to be deceased, with a median overall survival time following esophageal cancer diagnosis of seven months (range 0–5.6 years).
Table 1.
Characteristics of Hodgkin lymphoma (HL) patients who subsequently developed esophageal cancer (n=36) and matched controls (n=71).
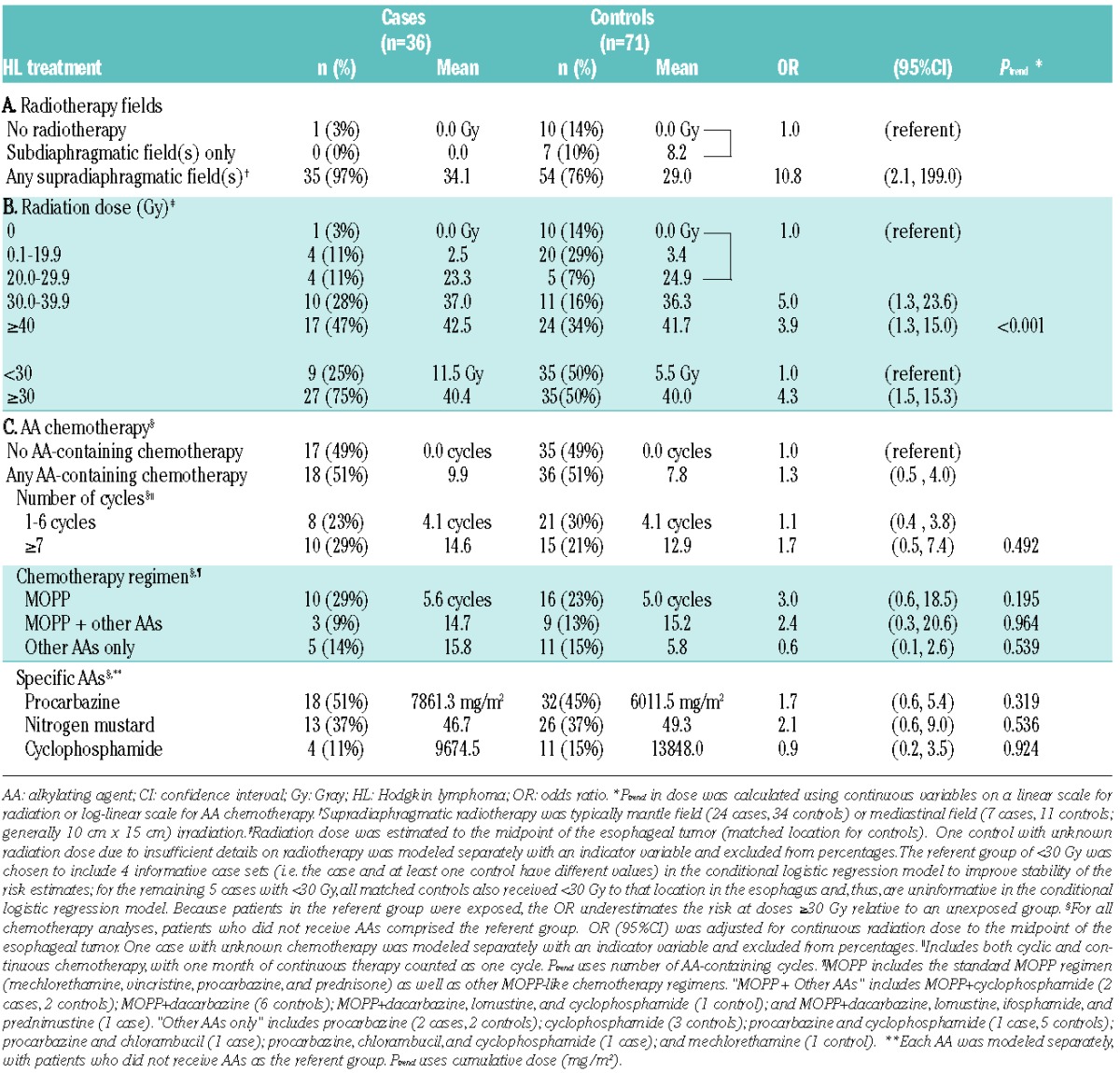
Nearly all cases (97%) and 76% of controls received supradiaphragmatic radiotherapy (OR=10.8: 95%CI: 2.1–199.0) (Table 2). Mean doses to the esophageal tumor location were 28.4 Gy for controls who received supradiaphragmatic radiotherapy versus 8.2 Gy for those who received only subdiaphragmatic radiotherapy. Esophageal cancer risk was 4.3-fold higher (95%CI: 1.5–15.3) among patients who received 30 Gy or more to the esophagus versus less than 30 Gy or no radiotherapy. Note that because patients in the referent group were exposed, the OR underestimates the risk at doses or 30 Gy or more relative to an unexposed group. The small numbers of cases receiving low doses precluded detailed evaluation of the shape of the radiation dose response, but data were compatible with linearity (EOR/Gy=0.38; 95%CI: 0.04–8.17; Ptrend <0.001). Radiation-related risks were consistent for esophageal adenocarcinoma and squamous cell carcinoma (Phomogeneity=0.847) and did not vary significantly according to age at exposure or sex, though risks were suggestively higher for esophageal cancer diagnosed at an older age (≥55 vs. <55 years; Phomogeneity=0.029) (Online Supplementary Table S1). However, statistical power was low for investigating such variation. Cases were somewhat more likely than controls to have relapsed disease (42% vs. 30%) (Table 1), but inclusion of an indicator variable for HL recurrence in the conditional logistic regression model was not statistically significant (P=0.230) and did not materially alter the radiation-related risk (data not shown).
Table 2.
Risk of esophageal cancer after specific treatments for Hodgkin lymphoma.
We provide the first investigation of esophageal cancer in a large cohort of HL survivors with long-term follow up, individual radiation dose reconstruction, and chemotherapy data. Combining our study results with the only other study of esophageal cancer with radiation dose reconstruction to the esophageal tumor (following radiotherapy for breast cancer)9 yielded a pooled EOR/Gy of 0.10 (95%CI: 0.05–0.18; Phomogeneity=0.202). These two studies substantially expand the evidence for a link between ionizing radiation exposure and esophageal cancer10 and complement previous studies of esophageal cancer in populations exposed to lower radiation doses, including patients treated for ankylosing spondylitis (ERR/Gy=0.17; 95%CI: 0.09–0.25)11 and Japanese atomic bomb survivors (ERR/Gy=0.52; 90%CI: 0.15–1.0).12
We observed little evidence of association between receiving AA-containing chemotherapy and esophageal cancer risk (OR=1.3; 95%CI: 0.5–4.0), even after considering the number of AA-containing cycles, specific regimens, and individual AAs (Table 2). A non-significant increased risk was observed for patients who received MOPP (mechlorethamine, vincristine, procarbazine, and prednisone), with or without other AAs (OR=2.4 and 3.0, respectively), but no trend was observed with increasing numbers of cycles (Ptrend=0.964 and 0.195, respectively). There was no significant difference in radiation-related risks according to whether patients received AA-containing chemotherapy (Phomogeneity=0.874) (Online Supplementary Table S1). The lack of association between chemotherapy and esophageal cancer contrasts with recent reports of AA-related increased risks for stomach and lung cancers following HL and colorectal cancer following childhood cancer (including HL).13,14 Our chemotherapy results should be interpreted with caution in the light of the relatively small number of patients and may not be applicable to current HL patients treated with ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine).1
Evaluation of other esophageal cancer risk factors (cigarette smoking, alcohol consumption, overweight/obesity, and family history of cancer) in multivariate models did not materially alter the radiation-related esophageal cancer risk (Online Supplementary Appendix). Nevertheless, patients receiving chest radiotherapy should avoid cigarette smoking.15
In summary, our study provides strong evidence that extended field supradiaphragmatic radiotherapy for HL is associated with a significantly increased risk of esophageal cancer, a rare but frequently fatal disease. The results should raise clinicians’ awareness of esophageal cancer risk among HL patients and lower the threshold for use of endoscopy to evaluate esophageal symptoms. Risks of esophageal cancer and other second cancers warrant consideration in future clinical trials of radiotherapy for HL, and future research should confirm whether the observed risks persist with current HL treatment approaches that use more limited radiotherapy fields.
Acknowledgments
we thank Diane Fuchs, Janet Lawler-Heavner, and their staff at Westat, Inc. (Rockville, MD, USA) for administrative assistance in conducting the field studies, and Jeremy Miller (Information Management Services, Silver Spring, MD, USA) for computer programming support.
Footnotes
The online version of this article has a Supplementary Appendix.
Funding: this work was supported by the Intramural Research Program of the National Cancer Institute, National Institutes of Health, Department of Health and Human Services; by National Cancer Institute contracts to Cancer Care Ontario, Toronto, Canada (N01-CP-31157), Danish Cancer Society, Copenhagen, Denmark (N01-CP-31019), Finnish Cancer Registry, Helsinki, Finland (N01-CP-31154), Information Management Services, Inc., Silver Spring, USA (N01-CP-31003), Karolinska Institute, Stockholm, Sweden (N01-CP-31156), University of Iowa, Iowa City, USA (N01-CP-31155), University of Texas MD Anderson Cancer Center, Houston, USA (N02-CP-55503), and Westat, Inc., Rockville, USA (N02-CP-31136); and by Oslo University Hospital, Radium Hospital.
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Engert A, Plutschow A, Eich HT, Lohri A, Dorken B, Borchmann P, et al. Reduced treatment intensity in patients with early-stage Hodgkin’s lymphoma. New Engl J Med. 2010;363(7):640–52 [DOI] [PubMed] [Google Scholar]
- 2.Mauch PM, Kalish LA, Kadin M, Coleman CN, Osteen R, Hellman S. Patterns of presentation of Hodgkin disease. Implications for etiology and pathogenesis. Cancer. 1993;71(6):2062–71 [DOI] [PubMed] [Google Scholar]
- 3.Sankila R, Garwicz S, Olsen JH, Dollner H, Hertz H, Kreuger A, et al. Risk of subsequent malignant neoplasms among 1,641 Hodgkin’s disease patients diagnosed in childhood and adolescence: a population-based cohort study in the five Nordic countries. Association of the Nordic Cancer Registries and the Nordic Society of Pediatric Hematology and Oncology. J Clin Oncol. 1996;14(5):1442–6 [DOI] [PubMed] [Google Scholar]
- 4.Metayer C, Lynch CF, Clarke EA, Glimelius B, Storm H, Pukkala E, et al. Second cancers among long-term survivors of Hodgkin’s disease diagnosed in childhood and adolescence. J Clin Oncol. 2000;18(12):2435–43 [DOI] [PubMed] [Google Scholar]
- 5.Dores GM, Metayer C, Curtis RE, Lynch CF, Clarke EA, Glimelius B, et al. Second malignant neoplasms among long-term survivors of Hodgkin’s disease: a population-based evaluation over 25 years. J Clin Oncol. 2002;20(16):3484–94 [DOI] [PubMed] [Google Scholar]
- 6.Hodgson DC, Gilbert ES, Dores GM, Schonfeld SJ, Lynch CF, Storm H, et al. Long-term solid cancer risk among 5-year survivors of Hodgkin’s lymphoma. J Clin Oncol. 2007;25(12):1489–97 [DOI] [PubMed] [Google Scholar]
- 7.Swerdlow AJ, Higgins CD, Smith P, Cunningham D, Hancock BW, Horwich A, et al. Second cancer risk after chemotherapy for Hodgkin’s lymphoma: a collaborative British cohort study. J Clin Oncol. 2011;29(31):4096–104 [DOI] [PubMed] [Google Scholar]
- 8.Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med. 1999;18(6):695–706 [DOI] [PubMed] [Google Scholar]
- 9.Morton LM, Gilbert ES, Hall P, Andersson M, Joensuu H, Vaalavirta L, et al. Risk of treatment-related esophageal cancer among breast cancer survivors. Ann Oncol. 2012;23(12):3081–91 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.United Nations. Effects of ionizing radiation: United Nations Scientific Committee on the Effects of Atomic Radiation -UNSCEAR 2006 Report, Volume 1 - Report to the General Assembly, with Scientific Annexes A and B. Vienna: United Nations; 2008 [Google Scholar]
- 11.Weiss HA, Darby SC, Doll R. Cancer mortality following X-ray treatment for ankylosing spondylitis. Int J Cancer. 1994;59(3):327–38 [DOI] [PubMed] [Google Scholar]
- 12.Preston DL, Ron E, Tokuoka S, Funamoto S, Nishi N, Soda M, et al. Solid cancer incidence in atomic bomb survivors: 1958–1998. Radiat Res. 2007;168(1):1–64 [DOI] [PubMed] [Google Scholar]
- 13.Morton LM, Dores GM, Curtis RE, Lynch CF, Stovall M, Hall P, et al. Stomach cancer risk after treatment for Hodgkin lymphoma. J Clin Oncol. 2013;31(27):3369–77 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Travis LB, Gospodarowicz M, Curtis RE, Clarke EA, Andersson M, Glimelius B, et al. Lung cancer following chemotherapy and radiotherapy for Hodgkin’s disease. J Natl Cancer Inst. 2002;94(3):182–92 [DOI] [PubMed] [Google Scholar]
- 15.Gilbert ES, Stovall M, Gospodarowicz M, van Leeuwen FE, Andersson M, Glimelius B, et al. Lung cancer after treatment for Hodgkin’s disease: focus on radiation effects. Radiat Res. 2003;159(2):161–73 [DOI] [PubMed] [Google Scholar]