

Abstract
Introduction
Dental anxiety is an important challenge for many patients and clinicians. It is thus of importance to know more about dental students’ own experiences with dental anxiety and their understanding of dental anxiety. The aim was to investigate differences in dental anxiety levels between dental students, psychology students, and biology students at a Norwegian university.
Materials and methods
A total of 510 students of dentistry, psychology, and biology at the University of Tromsø received a questionnaire consisting of the Modified Dental Anxiety Scale, demographic questions, and questions relating to their last visit to the dentist/dental hygienist; 169 students gave complete responses. Nonparametric tests were used to investigate differences between the student groups.
Results
The respondents were 78% female and 22% male; their mean age was 24 years. The dental students showed a significantly lower degree of dental anxiety than the psychology (P<0.001) and biology students (P<0.001). A significant decrease in dental anxiety levels was found between novice and experienced dentistry students (P<0.001).
Discussion
The dental students had less dental anxiety compared to psychology students and biology students. Experienced dental students also had less dental anxiety than novice dental students. This could indicate that the dentistry program structure at the university may influence dental anxiety levels.
Conclusion
Dental anxiety seemed to be less frequent in dentistry students compared to students of biology or clinical psychology. The practice-oriented dentistry education at the university might contribute to the differences in anxiety levels between new and experienced dentistry students.
Keywords: dentistry, Modified Dental Anxiety Scale, practice, training, education, questionnaire-study
Introduction
Fear of the dentist and dental treatment (dental anxiety or odontophobia) is a common problem. It can cause treatment difficulties for the practitioner, as well as severe consequences for the patient.1–3 Fearful patients might neglect their teeth and oral hygiene and avoid treatment.1–3 Patients with high levels of dental anxiety typically report psychological consequences as well, including psychological and social disability and reduced quality of life.4–6 Impaired dental status is a great source of shame among patients with dental anxiety.4–6 Embarrassment associated with smiling, talking, and eating can affect interactions, and deterioration of one’s social life can be a consequence.7
A number of theories have been proposed in order to explain why individuals develop dental anxiety. The theory of classic conditioning explains acquired fear as a result of previous negative or traumatic experiences.8 Consequently, negative experiences during dental treatment are possible factors that promote dental anxiety, and several studies have findings that support this.9,10 Moreover, de Jongh et al11 showed that distressing experiences in the dental setting was the most frequently reported negative experience among individuals with dental anxiety. These distressing experiences appear to be characterized by feelings of extreme helplessness during treatment, a lack of understanding from the dentist, and extreme embarrassment during treatment.12 Also, there is some evidence that dental anxiety is related to invasive or painful treatment.13 However, many common dental treatment procedures cause some amount of pain, but not all patients who experience pain will develop dental anxiety. This supports the notion that the relationship between pain and anxiety is more complex.14
Due to the large potential consequences to individual patients, as well as the treatment challenges this problem involves, the education and training of dentists is increasingly focused on the interpersonal aspects of the dental treatment situation.15–17 Consequently, dental students’ own experiences with dental anxiety and their understanding of dental anxiety have become of great importance in dental education.
The aim of this study was to reveal any differences in self-reported levels of dental anxiety between dental students, clinical psychology students, and biology students at the University of Tromsø (Tromsø, Norway). Dental students are a student group who get gradual experience and training in different dental procedures during their studies. This can be considered as a type of exposure therapy that will be advantageous for dental students with dental anxiety. Exposure to feared stimuli is a key component of cognitive behavioral therapy, as applied to dental phobia and anxiety.18 It is possible that this “environmental habituation” in addition to the dental education received will have positive effects on reducing the dental anxiety level of dental students. One could also assume that dental anxiety levels will decrease during the clinical part of the study (during the last 2 years) compared to the preclinical part of study (the first 2 years). This suggestion was supported by the longitudinal study of Peretz and Mann,19 who found a reduction in dental anxiety levels of female dental students during their dentistry studies.
Clinical psychology students acquire knowledge of the psychological mechanisms of anxiety through their field of study. They are also familiar with different psychological treatment approaches that could make them better able to cope with dental anxiety. In contrast, a student group outside the health sciences, such as biology students, could arguably have less knowledge (and fewer opportunities to obtain knowledge) about dental anxiety than either clinical psychology students or dentistry students. Hence, we suggest that psychology students will have a lower level of dental anxiety than biology students.
A comparison of dental anxiety between different student groups has previously been done by Al-Omari and Al-Omiri.20 They found that dental students had lower levels of dental anxiety than engineering students and medical students. Based on these assumptions related to the different student groups, we suggest the following hypotheses: 1) dental students will have lower dental anxiety levels than the other student groups; 2) clinical psychology students will have lower dental anxiety levels than the biology students; and 3) dental students in their last 2 years of study will have lower dental anxiety levels than dental students in their first 2 years of study.
Materials and methods
The study population consisted of 510 students at the University of Tromsø (now named UiT - The Arctic University of Norway), including students of dentistry (total number [N] =180), clinical psychology (N=171), and biology (N=159). The dentistry and clinical psychology programs are both professional studies that span 5 years. The biology students in the present study participated in the 3-year bachelor program in fisheries and aquaculture science.
The data collection was carried out in the autumn of 2012 using the Modified Dental Anxiety Scale (MDAS).21–23 In addition, students were asked for their sex, age, year of study, when they had had their last visit to the dentist/ dental hygienist, and if they go regularly to a dentist/dental hygienist.
A link to the questionnaire was sent to the students by Email. The questionnaire was made available online through use of a Web-based survey tool called “LimeSurvey”. All responses were recorded anonymously. After about 2 weeks, a reminder was sent by Email to the different student groups.
The study was approved by the Regional Committee for Medical and Health Research Ethics in North Norway, and permission to Email the survey to students was obtained from the study university.
Measuring of students’ dental anxiety was conducted using a Norwegian version of the MDAS.24 This survey is a modified version of the well-known Corah’s Dental Anxiety scale (DAS).23 Compared to the DAS, the MDAS contains an additional question about the responder’s anxiety towards injections with local anesthesia.22
The MDAS is a five-item questionnaire containing questions about the respondent’s anxiety level when visiting the dentist, with a response scale ranging from 1 (not anxious) to 5 (extremely anxious). The total score range is from 5–25. A score below 11 is normal, a score from 11–18 represents moderate anxiety, and a score above 18 represents extreme anxiety.25
The data collected through the questionnaires in the LimeSurvey was transferred to the IBM Corporation SPSS Statistics 19 program (Armonk, NY, USA).26 Descriptive statistics were measured to compare sex and age. Mean values (M) and standard deviations (SD) in all the groups together and separately were recorded. The respondents’ scores on the MDAS were summed together and made into a new variable. MDAS sum scores for the dental students, the biology students, and the clinical psychology students were compared using nonparametric tests (Kruskal–Wallis and Mann–Whitney U-test). In this way, we could assess whether the between-group differences in MDAS sum scores were statistically significant, according to hypotheses 1 and 2.
To reveal any differences within the dental students group in terms of year of study, as we suggested in hypothesis 3, we conducted an additional Mann–Whitney U-test, in which we compared dental anxiety levels for the first 2 years of study (sample number [n] =30) with the last 2 years of study (n=36).
Results
A total of 510 students were contacted and invited to participate in the study; 169 participants gave complete responses (193 responded in total). This resulted in a response rate of 33%. Divided by student group, the response rates were 23% (biology), 34% (clinical psychology), and 54% (dentistry).
The participants’ mean age was 24 (SD =4.86) years; 131 (78%) were female and 38 (22%) were male. Due to the skewed distribution with regard to the participants’ sex, a preliminary analysis was performed with regard to sex and MDAS score. An independent samples Mann–Whitney U-test showed that the difference between the MDAS scores of females (M =10.08; SD =4.21) and males (M =9.05; SD =2.72) was not statistically significant (P=0.41). No difference in dental anxiety levels relative to age was found.
Fifteen of 49 (30.6%) psychology students, ten of 85 (11.8%) dental students, and 17 of 35 (48.6%) biology students had a MDAS score >12 (Figure 1) (ie, they had moderate to high levels of dental anxiety). The mean MDAS score of the biology students (n=35) was 12.46 (SD =4.65), while dental students’ (n=85) and psychology students’ (n=49) mean scores were within the normal range (psychology: M =10.73, SD =3.79; dentistry: M =8.27, SD =2.87). The mean value of all students was 9.85 (SD =3.94). An independent samples Kruskal–Wallis test showed a significant difference in dental anxiety levels between the three student groups (P<0.001). The difference was further investigated in accordance with the hypotheses by post hoc comparisons using Mann–Whitney U-tests.
Figure 1.
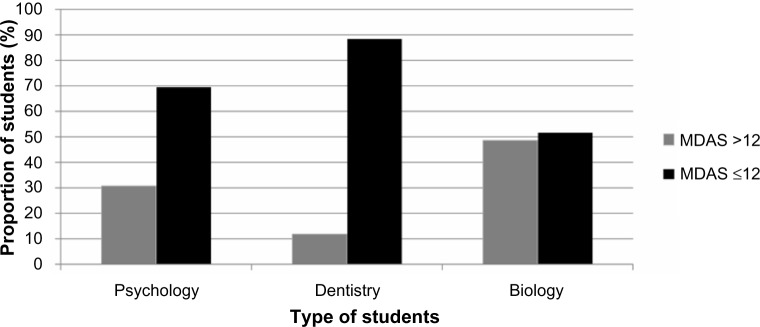
The number of students with MDAS levels above 12 or 12 and below.
Abbreviation: MDAS, Modified Dental Anxiety Scale.
The post hoc tests showed that the anxiety level of dental students (M =8.27; SD =2.87) was significantly different (P<0.001) than for the psychology students (M =10.73; SD =3.79) and biology students (M =12.46; SD =4.65). This was consistent with hypothesis 1. Hypothesis 2 proposed that there would be a difference in anxiety levels between psychology students and biology students, but this was not supported by the post hoc comparison Mann–Whitney U-test (P=0.13).
Hypothesis 3 was investigated by performing an independent samples Mann–Whitney U-test on the mean scores of MDAS for dental students in their last 2 years of study and dental students in their first 2 years of study (excluding year 3). The mean and SD of MDAS scores for the first- to second-year (n=30) students was 9.97 (SD =3.39), and for fourth- to fifth-year dental students (n=36) the score was 7.11 (SD =1.77). The test showed that the MDAS scores were significantly lower for years 4 and 5 compared to years 1 and 2 (P<0.001).
Discussion
This study shows that dental students have lower levels of dental anxiety than biology students and psychology students, respectively. The findings therefore support the first hypothesis. There was no significant difference in dental anxiety between the psychology students and the biology students, as suggested in the second hypothesis. The dental students in the last 2 years of study had lower levels of dental anxiety than did students in their first 2 years.
Several explanations might be suggested for the findings regarding the differences between the student groups. These might be 1) related to the contents of the field of study, 2) related to the individuals who seek out different fields of study (ie, personality), or 3) a combination of both.14 Put in simple terms, the finding that dental students have lower anxiety levels than psychology students and biology students could be related to the fact that dental students have more practical dental knowledge than the other two student groups. At the study university, dental students start their practical training in their third year with models of artificial teeth. Later in the same year, students move on to do simple treatment tasks on each other, such as applying anesthesia, and they start to treat their own patients. This represents a level of experience with dental treatment that the other two student groups obviously lack. Behavioral techniques that include in vivo exposure are most commonly used to treat phobic patients. The effect of the therapy is to reduce the fear of the frightening stimuli by eliminating avoidance behaviors and thereby – with repeated exposure – to experience decreased anxiety in previously feared situations.27,28 This is important because avoidance behaviors can be seen as a crucial mechanism for maintaining phobias. As in exposure techniques, dental students will gradually be exposed to a hierarchy of potentially anxiety-provoking situations. This might begin with reading theory on the subject (such as dental anatomy) and training on phantom dolls, and culminate in performing dental examinations and anesthesia on other students (including being subjected to such procedures). Another aspect with the dental study is that the students learn how to manage fearful patients, especially children. There is a focus on preventing the development of dental anxiety among children, and children are approached by means of verbal and visual procedures before the treatment is started. This method is commonly known as the “tell, show, do” method.29
The theory proposed here of gradual exposure to fear-provoking stimuli as part of the dentistry program can also be related to the fact that dental students in their early years have more signs of dental fear than do senior students. In the first 2 years, no practical training is conducted, and thus no behavioral therapeutic effect from exposure can be expected.
Other explanations for differences in dental anxiety could be that the dental students in the first years are more vulnerable to stress and anxiety because they are in an unfamiliar study environment. Students just starting their studies can experience more stress due to the challenge of transitioning from high school to university, and a study from the United States indicated that freshmen and sophomores have been shown to have higher stress reactions than juniors and seniors.30 Reduction in stress due to settling into university life might, therefore, be a nonspecific process contributing to reduction of specific anxiety (for example, dental anxiety).
To our knowledge, there has been only one prior study examining the development of dental anxiety among dental students.19 That study showed that the dental students’ DAS score went from 10.4 to 8.0 over a 4-year period, as compared to our cross-sectional study that showed mean MDAS scores of 9.9 (first to second year) and 7.1 (fourth to fifth year).19
The findings regarding our first hypothesis are also consistent with the study by Al-Omari and Al-Omiri,20 where significantly lower levels of dental anxiety were found among the dental students compared to the medical students and the engineering students. The authors concluded that a lack of dental education could be seen as an unfortunate factor in dental anxiety.
The biology students had the highest dental anxiety score among the student groups, followed by the psychology students. The clinical psychology students at the University of Tromsø start their clinical practice in the fourth year of study, which will enable them to be familiar with the mechanisms of anxiety and behavioral therapeutic approaches (similar to those used in the treatment of dental anxiety). The results could indicate that the theoretical knowledge acquired during the psychology study is not as important as could be assumed with respect to the students’ own levels of anxiety. But it could also be that the students who do not yet possess clinical knowledge (ie, first to third year) are more anxious than the clinical psychology students in the two last years of study and thereby contribute to increased levels of anxiety when we examine the the whole group of clinical psychology students together. A Brazilian study showed that 13% of undergraduate psychology students exhibited a high degree of dental fear.31
It should be noted that the number of female students was approximately 10% higher among the clinical psychology students than among those studying biology. Research shows that females have higher levels of dental anxiety,32–34 although this study did not find the difference between females and males to be significant (P=0.16). In general, sex differences might contribute to an increase in the level of dental anxiety in student groups with predominantly female students.
The study by Al-Omari and Al-Omiri20 also compared dental anxiety levels between health-related and nonhealth-related studies (medicine and engineering). Uniform with our findings, no statistical significant difference between the health-related (psychology) and the nonhealth-related (biology) studies were found when excluding dental students.
Also, the low MDAS score observed in dental students may be due to the interplay between the field of study and personality traits. Dentistry is a varied study where the students are continuously exposed to both theoretical and practical requirements. Students could, therefore, be able to cope with psychological stress in a better way, and this could make them less vulnerable to dental anxiety. On the other hand, the psychology students also experience a stressful academic life, but despite this, they still have higher dental anxiety levels. Hence, the practical part of dental education may be the key factor for reducing the level of anxiety. It can also be argued that individuals prone to dental anxiety would avoid choosing a field of study that could provoke their anxiety. Anxious individuals might exclude themselves from the study of dentistry; however, many students choose their field of study based on prestige and not according to what would match their personality traits.35 An Irish study of undergraduate dental students showed that factors influencing their decision to choose dentistry were the ease of getting employment, the possibility of being self-employed, being able to work regular hours, a good income, and an opportunity to help people.36
Negative and unsupportive dentist behavior has been reported as a significant factor in the development of dental anxiety,37 and a more empathic behavior has been associated with decreased dental anxiety.38 Dental students with dental anxiety will be familiar with the negative consequences of unfortunate dentist behavior, which could motivate them to work towards a more patient-centered style.39–42
The results might have been affected by the large group of dental students relative to the two other smaller groups. In addition, the number of individuals with dental anxiety was considerably lower in the dental student group versus the two other groups. Another bias could be the uneven sex distribution between the groups, as research shows a higher prevalence of anxiety among females.
The study by Peretz and Mann19 followed the same student group over a 4-year period. Since our study is not longitudinal, the results could not be directly compared. However, our findings can indicate that the dental program structure can be a significant factor in reducing dental anxiety. To our knowledge, there are no current studies investigating correlations of dental anxiety between biology students and psychology students. Further research on the subject is needed.
Conclusion
Compared to psychology students and biology students, the dental students demonstrated a lower degree of dental anxiety. Senior dental students with clinical experience also showed a lower dental anxiety level than junior dental students. The practice-oriented dentistry education at the study university might contribute to the differences in anxiety levels between new and experienced dentistry students.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Armfield JM, Slade GD, Spencer AJ. Dental fear and adult oral health in Australia. Community Dent Oral Epidemiol. 2009;37(3):220–230. doi: 10.1111/j.1600-0528.2009.00468.x. [DOI] [PubMed] [Google Scholar]
- 2.DeDonno MA. Dental anxiety, dental visits and oral hygiene practices. Oral Health Prev Dent. 2012;10(2):129–133. [PubMed] [Google Scholar]
- 3.Kesim S, Unalan D, Esen C, Ozturk A. The relationship between periodontal disease severity and state-trait anxiety level. J Pak Med Assoc. 2012;62(12):1304–1308. [PubMed] [Google Scholar]
- 4.Mehrstedt M, John MT, Tönnies S, Micheelis W. Oral health-related quality of life in patients with dental anxiety. Community Dent Oral Epidemiol. 2007;35(5):357–363. doi: 10.1111/j.1600-0528.2007.00376.x. [DOI] [PubMed] [Google Scholar]
- 5.Pohjola V, Mattila AK, Joukamaa M, Lahti S. Anxiety and depressive disorders and dental fear among adults in Finland. Eur J Oral Sci. 2011;119(1):55–60. doi: 10.1111/j.1600-0722.2010.00795.x. [DOI] [PubMed] [Google Scholar]
- 6.Janković SM, Aleksić D, Bahtijari Z, et al. Risk factors for severe dental anxiety among medical students. Vojnosanit Pregl. 2014;71(1):16–21. doi: 10.2298/vsp1401016j. [DOI] [PubMed] [Google Scholar]
- 7.Moore R, Brødsgaard I, Rosenberg N. The contribution of embarrassment to phobic dental anxiety: a qualitative research study. BMC Psychiatry. 2004;4:10. doi: 10.1186/1471-244X-4-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lavond D, Steinmetz J. Handbook of classical conditioning. New York, NY: Springer; 2003. [Google Scholar]
- 9.Skaret E, Raadal M, Berg E, Kvale G. Dental anxiety among 18-yr-olds in Norway. Prevalence and related factors. Eur J Oral Sci. 1998;106(4):835–843. doi: 10.1046/j.0909-8836.1998.eos106402.x. [DOI] [PubMed] [Google Scholar]
- 10.de Jongh A, ter Horst G. Dutch students’ dental anxiety and occurrence of thoughts related to treatment. Community Dent Oral Epidemiol. 1995;23(3):170–172. doi: 10.1111/j.1600-0528.1995.tb00223.x. [DOI] [PubMed] [Google Scholar]
- 11.de Jongh A, Fransen J, Oosterink-Wubbe F, Aartman I. Psychological trauma exposure and trauma symptoms among individuals with high and low levels of dental anxiety. Eur J Oral Sci. 2006;114(4):286–292. doi: 10.1111/j.1600-0722.2006.00384.x. [DOI] [PubMed] [Google Scholar]
- 12.Humphris G, King K. The prevalence of dental anxiety across previous distressing experiences. J Anxiety Disord. 2011;25(2):232–236. doi: 10.1016/j.janxdis.2010.09.007. [DOI] [PubMed] [Google Scholar]
- 13.Locker D, Shapiro D, Liddell A. Negative dental experiences and their relationship to dental anxiety. Community Dent Health. 1996;13(2):86–92. [PubMed] [Google Scholar]
- 14.Halonen H, Salo T, Hakko H, Räsänen P. Association of dental anxiety to personality traits in a general population sample of Finnish University students. Acta Odontol Scand. 2012;70(2):96–100. doi: 10.3109/00016357.2011.598182. [DOI] [PubMed] [Google Scholar]
- 15.Hannah A, Millichamp CJ, Ayers KM. A communication skills course for undergraduate dental students. J Dent Educ. 2004;68(9):970–977. [PubMed] [Google Scholar]
- 16.Wagner J, Arteaga S, D’Ambrosio J, et al. A patient-instructor program to promote dental students’ communication skills with diverse patients. J Dent Educ. 2007;71(12):1554–1560. [PubMed] [Google Scholar]
- 17.Lodge J, Tripp G. Dental students’ perception of patient anxiety. N Z Dent J. 1993;89(395):50–52. [PubMed] [Google Scholar]
- 18.Öst LG, Clark DM. Cognitive behavior therapy: principles, procedures and evidence base. In: Öst LG, Skaret E, editors. Cognitive Behavioral Therapy for Dental Phobia and Anxiety. 1st ed. Wiley-Blackwell; 2013. pp. 91–108. [Google Scholar]
- 19.Peretz B, Mann J. Dental anxiety among Israeli dental students: a 4-year longitudinal study. Eur J Dent Educ. 2000;4(3):133–137. doi: 10.1034/j.1600-0579.2000.040308.x. [DOI] [PubMed] [Google Scholar]
- 20.Al-Omari WM, Al-Omiri MK. Dental anxiety among university students and its correlation with their field of study. J Appl Oral Sci. 2009;17(3):199–203. doi: 10.1590/S1678-77572009000300013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Humphris GM, Freeman R, Campbell J, Tuutti H, D’Souza V. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int Dent J. 2000;50(6):367–370. doi: 10.1111/j.1875-595x.2000.tb00570.x. [DOI] [PubMed] [Google Scholar]
- 22.Humphris GM, Morrison T, Lindsay SJ. The Modified Dental Anxiety Scale: validation and United Kingdom norms. Community Dent Health. 1995;12(3):143–150. [PubMed] [Google Scholar]
- 23.Corah NL, Gale EN, Illig SJ. Assessment of a dental anxiety scale. J Am Dent Assoc. 1978;97(5):816–819. doi: 10.14219/jada.archive.1978.0394. [DOI] [PubMed] [Google Scholar]
- 24.Haugejorden O, Klock KS. Avoidance of dental visits: the predictive validity of three dental anxiety scales. Acta Odontol Scand. 2000;58(6):255–259. doi: 10.1080/00016350050217091. [DOI] [PubMed] [Google Scholar]
- 25.Freeman R, Clarke HM, Humphris GM. Conversion s for the Corah and Modified Dental Anxiety Scales. Community Dent Health. 2007;24(1):49–54. [PubMed] [Google Scholar]
- 26.IBM SPSS statistics. Armonk, NY: IBM Corporation; 2014. [Accessed May 1, 2014]. IBM Corporation [webpage on the Internet] Available from: http://www-01.ibm.com/software/analytics/spss/products/statistics/ [Google Scholar]
- 27.Löhr HD, Rosenvinge JH, Wynn R. Integrating psychoeducation in a basic computer skills course for people suffering from social anxiety: participants’ experiences. J Multidiscip Healthc. 2011;4:311–319. doi: 10.2147/JMDH.S23691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pettersen G, Rosenvinge JH, Wynn R. Eating disorders and psychoeducation - patients’ experiences of healing processes. Scand J Caring Sci. 2010;25(1):12–18. doi: 10.1111/j.1471-6712.2010.00783.x. [DOI] [PubMed] [Google Scholar]
- 29.American Academy of Pediatric Dentistry Guideline on behavior guidance for the pediatric dental patient. [Accessed 29 August, 2014]. Available from: http://www.aapd.org/media/Policies_Guidelines/G_BehavGuide.pdf.
- 30.Misra R, McKean M. College students’ academic stress and its relation to their anxiety, time management, and leisure satisfaction. Am J Health Stud. 2000;16(1):41–51. [Google Scholar]
- 31.Cesar J, de Moraes AB, Milgrom P, Kleinknecht RA. Cross validation of a Brazilian version of the Dental Fear Survey. Community Dent Oral Epidemiol. 1993;21(3):148–150. doi: 10.1111/j.1600-0528.1993.tb00740.x. [DOI] [PubMed] [Google Scholar]
- 32.Armfield JM, Spencer AJ, Stewart JF. Dental fear in Australia: who’s afraid of the dentist? Aust Dent J. 2006;51(1):78–85. doi: 10.1111/j.1834-7819.2006.tb00405.x. [DOI] [PubMed] [Google Scholar]
- 33.Enkling N, Marwinski G, Jöhren P. Dental anxiety in a representative sample of residents of a large German city. Clin Oral Investig. 2006;10(1):84–91. doi: 10.1007/s00784-006-0035-6. [DOI] [PubMed] [Google Scholar]
- 34.Hakeberg M, Hallonsten A-L, Hägglin C, Skaret E. Tandvårdsrädslans epidemiologi. [The epidemiology of dental anxiety] Tandläkartidningen. 2003;95:22–29. Swedish. [Google Scholar]
- 35.Onoyase D, Onoyase A. The relationship between personality types and career choice of secondary school students in federal government colleges in Nigeria. Anthropologist. 2009;11(2):109–115. [Google Scholar]
- 36.Hallissey J, Hannigan A, Ray N. Reasons for choosing dentistry as a career – a survey of dental students attending a dental school in Ireland during 1998–1999. Eur J Dent Educ. 2000;4(2):77–81. doi: 10.1034/j.1600-0579.2000.040205.x. [DOI] [PubMed] [Google Scholar]
- 37.Abrahamsson KH, Berggren U, Hallberg L, Carlsson SG. Dental phobic patients’ view of dental anxiety and experiences in dental care: a qualitative study. Scand J Caring Sci. 2002;16(2):188–196. doi: 10.1046/j.1471-6712.2002.00083.x. [DOI] [PubMed] [Google Scholar]
- 38.Corah NL, O’Shea RM, Bissell GD, Thines TJ, Mendola P. The dentist-patient relationship: perceived dentist behaviors that reduce patient anxiety and increase satisfaction. J Am Dent Assoc. 1988;116(1):73–76. doi: 10.14219/jada.archive.1988.0162. [DOI] [PubMed] [Google Scholar]
- 39.Wynn R. The Linguistics of Doctor-Patient Communication: An Analysis of the Methodology of Doctor-Patient Communication Research. Oslo, Norway: Novus Press; 1995. [Google Scholar]
- 40.Bergvik S, Wynn R, Sørlie T. Nurse training of a patient-centered information procedure for CABG patients. Patient Educ Couns. 2008;70(2):227–233. doi: 10.1016/j.pec.2007.10.013. [DOI] [PubMed] [Google Scholar]
- 41.Wynn R. Empathy in general practice consultations: a qualitative analysis. Epidemiol Psichiatr Soc. 2005;14(3):163–169. doi: 10.1017/s1121189x00006412. [DOI] [PubMed] [Google Scholar]
- 42.Wynn R. Medical students, doctors: is there a difference? Text. 1996;16(3):423–448. [Google Scholar]